
Abstract
Abstract
Background:
Paraumbilical hernia with benign gallbladder disease forms a challenging combination for offering benefits of single-incision surgery. The purpose of this prospective observational study was to assess the outcomes of paraumbilical hernia repair performed concomitantly with three-port laparoscopic cholecystectomy through the same periumbilical incision using routine instruments.
Patients and Methods:
In total, 126 subjects formed the patient cohort. The mean age for females was 38.5 years, and that for the males was 40 years. The periumbilical curved incision accommodated three independent ports for conducting the cholecystectomy. The subsequent choice for the hernia repair was subject to the size (diameter) of the defect. Defects <4 cm in diameter (n=96) were suture-closed without mesh reinforcement. For defects 5–8-cm in diameter (n=33), an innovative technique of inserting all three ports directly into the peritoneal/hernial sac in a triangular manner was used for the cholecystectomy. Such a hernia defect was then reinforced with preperitoneal polypropylene mesh before closing it primarily after releasing the posterior rectus sheath. However, defects >8 cm were excluded from the study.
Results:
The mean operative time was 75 minutes. Patients were discharged after a mean of 1.5 days. Four patients were converted to conventional laparoscopic cholecystectomy owing to technical difficulty. An umbilical seroma occurred in 3 patients. Over the mean follow-up of 38.5 months, none of the patients had paraumbilical hernia recurrence. A hernial sac was used to space out the ports. The morbidity of the procedure was acceptable.
Conclusions:
Concomitant paraumbilical repair and cholecystectomy by the technique described is effective and safe for select patients. Prosthetic reinforcement is advisable for hernia defects with a diameter of 5–8 cm.
Introduction
T
Patients and Methods
In total, 126 patients were operated between August 2009 and March 2011. Approval of the Institute's ethics committee was obtained before commencement. Only those patients who were symptomatic for both the pathologies—PUH and BGD—were selected for the concomitant surgery (Table 1). All the patients received an explanation about the nature of the surgery and the likely advantages/complications. Written informed consent was obtained accordingly. All the surgeries were performed by the same surgeon using routine laparoscopic instruments. The clinical data were prospectively collected and analyzed.
BMI, body mass index; PUH, paraumbilical hernia.
Of the 126 patients, 86 patients were females, and 40 patients were males. The mean age of the females was 38.5 years (range, 23–56 years), and that for the males was 40 years (range, 32–58 years). The average body mass index of the females was 28.8 kg/m2 (range, 20–33 kg/m2) and that for the males was 26.1 kg/m2 (range, 21–32 kg/m2). Fifteen patients were diabetic with good glycemic control. Two patients were hypertensive under control with medications. Ten patients had concomitant hypertension and diabetes. Thirteen patients had chronic obstructive pulmonary disease (Table 2). On the basis of the method of PUH repair offered, we divided the patients into two groups. Group A comprised patients for whom the diameter of their PUH was <4 cm (n=93) and who were offered only suture-closure of the defect without using mesh. Group B consisted of 33 subjects for whom the diameter of their PUH was 5–8 cm and it was reinforced by preperitoneal polypropylene mesh. The mean duration of history noted for the study was 3.8 years (range, 1–7 years). Of the 126 patients of this series, 5 patients (with a defect size <4 cm in diameter) had a supraumbilical defect. The rest of the patients had an infraumbilical hernia defect.
ASA, American Society of Anesthesiologists; BMI, body mass index; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; HTN, hypertension; USG, ultrasonography.
The size and the anatomical location of the defects were assessed by preoperative high-resolution ultrasonography of the umbilical region. The postoperative pain was assessed by a visual analog scale ranging from 0 to 10. Bearing in mind the restricted literacy level of our rural patients, we devised a simple “aesthetic scale” (from 0 to 10) as per the subjective assessment of the scars they received. Because our Institute is a government tertiary-care center offering free medical services to society, it was not possible to conduct a cost analysis for this series.
Surgical technique
The procedure was carried out with the patient under general anesthesia and positioned supine in a 25°–30° reverse Trendelenburg position with the right side up. A nasogastric tube was inserted, and single-dose cefotamxime (1.0 g) antibiotic was administered at induction. The monitor placed at the right shoulder of the patient. We performed all the surgeries with the operating surgeon standing at the left-hand side of the patient and the camera assistant on the left of the surgeon.
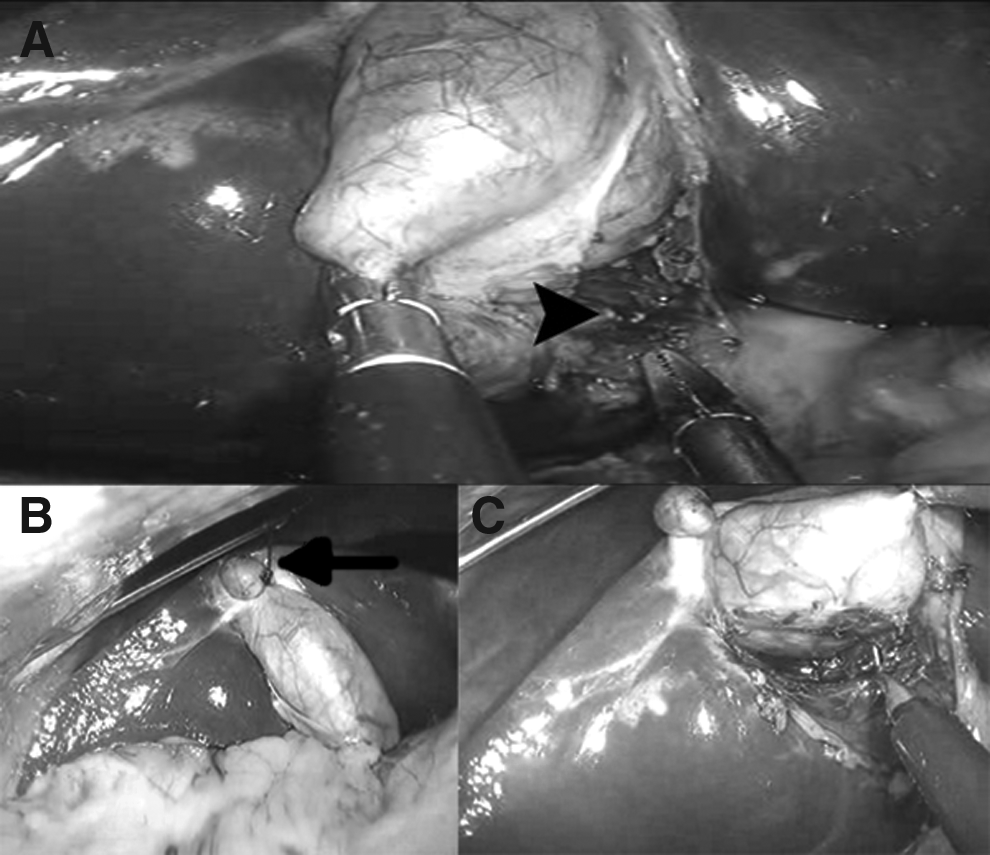
For subjects with a defect <4 cm in diameter (Group A), a 4-cm curvilinear infraumbilical incision was placed to expose the hernia sac. Once it was opened, the index finger was inserted into the defect to rule out any omental/enteric adhesions. Then a 10-mm cannula was introduced into the peritoneal cavity (Fig. 1). This was made “air-tight” by double pursestring 3-0 silk sutures (which were removed at the end of the procedure). A 12 mm Hg pneumoperitoneum was then created. Two 5-mm working trocars were inserted under vision at the corners of the incision. This achieved a wider ergonomic triangle for unobstructed working (Fig. 2). The fundus of the gallbladder was retracted cephalad with a catgut loop held by the standard port-closure needle passed through a 2-mm stab wound at the midclavicular line in the right hypochondrium. This gave a good exposure of the cystohepatic triangle for the safe dissection to accomplish the “critical view of safety” (Fig. 3). We used monopolar electrosurgery as the energy source for hemostasis. The cystic duct and the artery were clipped by the 5-mm clip applier passed through the right-hand working port. However, in 6 patients, we changed the 10-mm laparoscope to the 5-mm one for accommodating the 10-mm clip applier. Once the gallbladder was completely dissected, a thorough saline wash was given, and the hemostasis was checked. The 10-mm port was used for the specimen extraction via an endobag. When required, large stones were crushed and removed. We did not join the port sites for the specimen extraction. PUH defects <4 cm in diameter were suture-closed with 1-0 polypropylene interrupted sutures (the so-called “anatomical repair”) without prosthetic reinforcement. Furthermore, both the 5-mm working ports were closed under direct vision. The stretched-out umbilical cutis was reconstructed, and the skin was closed with 3-0 subcuticular monofilament absorbable suture to achieve a good cosmetic result (Fig. 4). However, for the subgroup of patients with a supraumbilical PUH defect (n=5), we modified the technique by using a supraumbilical 4-cm curvilinear incision (instead of infraumbilical) for rather direct access to the hernia defect. This eased out on dissection needed for lifting the umbilical flap and potentially reduced the postoperative seroma formation. The rest of the port positioning remained mirror-opposite to what was discussed earlier.

The curvilinear infraumbilical incision. Note that the hernia sac (arrow) is being used for 10-mm laparoscopic port insertion.

The port assembly. Note that the two 5-mm working ports are inserted after stretching out the angles of incision to achieve a wider triangulation.
Dissecting the cystohepatic triangle.

The reconstructed umbilicus.
However, for the patients with PUH defects of 5–8 cm in diameter (Group B), we used an innovative technique of using the hernia sac for accommodating all the operating ports. For this, we placed an infraumbilical curvilinear incision equivalent to half the circumference of the hernia defect with 2-cm lateral extensions on both the sides for better exposure (the “inverted omega” incision). Such an incision helped us to better delineate the hernia sac. Once the umbilical flap was raised, the hernia sac was defined and held stretched by a Babcock's tissue-holding forceps. Subsequently, an 11-mm rent was created directly in the peritoneal sac at the 6 o'clock position for initial confirmation for the absence of adhesions with an index finger. A 10-mm camera trocar was then inserted through this rent and was made “air-tight” by double-layer pursestring 3-0 silk sutures before creating a pneumoperitoneum (12 mm Hg). Two other 5-mm working trocars were inserted at the 10 and 2 o'clock positions to purchase some extra intertrocar space while maintaining the triangulation. These port trajectories were also rendered “air-tight” similarly. Once the gallbladder was dissected completely, the ports along with their silk pursestring sutures were removed, all the three rents joined together, and the gallbladder was extracted in an endobag through this larger rent. This rent was then closed with 3/0 polyglactin continuous suture. Furthermore, the preperitoneal space was gently worked out circumferentially to accommodate a polypropylene mesh that reinforced the defect at least 3 cm beyond the margin. It was then fixed to the peritoneum at its four corners and the center. The posterior rectus sheath was then released, and the hernia defect was closed with 1-0 polypropylene interrupted sutures to create a neo-midline. To achieve “tension-less” closure we did not close the anterior rectus sheath. The umbilical cutis was trimmed, and the incision was closed with 3-0 subcuticular monofilament absorbable suture.
Results
The mean operative time and blood loss were 75 minutes (range, 45–120 minutes) and 15 mL (range, 5–40 mL), respectively. All patients were allowed solid food by 6 hours (range, 4–8 hours) after surgery and were ambulatory by then. No extra port was required in any patient. We converted 4 (3.17%) patients to conventional laparoscopic cholecystectomy because of fibrotic adhesions around the cystohepatic triangle. However, we did not have to convert any patient to open cholecystectomy. Thus, we could complete the surgery in 122 patients out of 126 patients.
There were no bile duct/vascular injuries. We had one inadvertent electrosurgical injury to the first part of the duodenum that was successfully repaired by intracorporeal suturing with 2-0 silk. The patient had an uneventful postoperative course without needing any surgical/percutaneous intervention. Two patients (1.59%) with paraumbilical defects <4 cm in diameter had inadvertent gallbladder perforations during dissection. These were small perforations with no stone spillage and needed only a local saline wash.
The visual analog scale scores on Days 0, 1, 7, and 30 of surgery were on average 2 (range, 1–4), 1.5 (range, 1–2), 0.5 (range, 0–1), and 0, respectively. The patients were discharged after a mean of 1.5 days (range, 1–5 days). Three patients (2.38%) had umbilical seroma (Table 3). Two of them had a PUH defect 6 and 7 cm in diameter; the third had a 4-cm-diameter defect. All three recovered with the expectant line of treatment. None of the patients of this series had a surgical site infection.
All our patients are receiving regular follow-up. The first case in this series has completed 4 years of follow-up, and the last case has finished 2 years 4 months of follow-up. Although a long-term follow-up is necessary for the final comments, none of the patients in this series developed PUH recurrence during our mean follow-up of 38.5 months (range, 28–48 months). The cosmetic outcome of the technique was good with a mean aesthetic scale score of 8.8 (range, 6–10). There was no mortality in this series.
Discussion
PUH presenting with BGD remains a unique clinical scenario. Offering all the advantages of the recently developed technique of single-incision surgery to these patients at the same sitting may be a rather challenging task owing to involvement of different abdominal quadrants in the dissections. Single-port cholecystectomy, although popular, has showed mixed results in the most recent meta-analysis. 3 Nevertheless, a surgical approach that amalgamates the advantages of standard laparoscopy (by using common laparoscopic instruments) with the single-site surgery (by using the umbilicus) to achieve favorable results may appear as a valuable option, especially for resource-poor nations. The three-port technique described in this article tends to circumvent the “chopstick effect” of the instruments apart from maintaining their triangulation. Moreover, as only routine laparoscopic instruments are used, this procedure has the potential to reduce the learning curve of a beginner. To the best of our knowledge, such a technique has not been reported in the literature.
Patients with smaller (<4 cm in diameter) paraumbilical fascial defects are the ideal candidates for this technique as prosthetic reinforcement is likely to be deferred in such patients. However, to offer a purely transumbilical approach to those patients with BGD associated with PUH having defects >5 cm in diameter remains a challenging situation because of the lack of secure placement of the operating ports and the subsequent need for prosthetic reinforcement. Our series presents a large number of patients (n=33) with large-sized (5–8 cm in diameter) PUH defects. This could probably be due to the suboptimal educational background of our rural patients and lack of physical exercise, especially in multiparous women. We have further observed that these factors are generally compounded by the general tendency of these patients in delaying to consult a physician. For these patients, our technique makes use of the hernia sac for porting, thus ensuring greater spacing between the working channels. Moreover, regarding the 33 patients with PUH defects 5–8 cm in diameter, we observed that the hernia sac was thick enough for easy “leak-proof” port placements as well as subsequent creation of the preperitoneal space. This may be attributed to the long duration of their hernias. 4 Moreover, reinforcing the PUH defect with the preperitoneal prosthesis is likely to limit the incidence of hernia recurrence. However, in a situation where in the hernia sac remains thin, this technique may have a limited use. Although we did not face such a scenario in this series, we feel that this may turn out to be a major restriction for secure porting and creation of adequate preperitoneal space without damaging the sac. In these cases, one may opt for an upfront single-port cholecystectomy (if facilities available) or go ahead for creation of a neo-midline with the released posterior sheath followed by the three-port technique via the medially displaced posterior rectus sheath. Subsequently, polypropylene mesh may be deployed in a retrorectus plane.
The rate of umbilical infection in laparoscopic single-incision surgery is reported to be in the range of 0%–14%. 5 None of the patients in this study developed this complication. The probable reasons for this could be (1) our policy of meticulous chlorhexidine cleaning of the umbilicus, both the day prior and “on-table,” and (2) routine use of endobags uniformly for all the gallbladder extractions as reported earlier. 6 Also, the conversion rate in this series remained at a par with the literature for single-incision surgery (0%–24%).5,6 Nevertheless, we should keep a low threshold for conversion to standard multiport laparoscopy or open surgery.5,7 A similar technique reported the use of all 5-mm ports and joined two port sites for specimen extraction. 8 However, our technique uses a 10-mm port (for the 10-mm laparoscope) from the start of the surgery as it gives much brighter, clearer, and wider vision. It can subsequently be used for a 10-mm clip applier and specimen extraction.
Recurrence of PUH remains one of the major issues that merit focus. In this regard, a recent multicenter randomized trial has reported significantly higher rate of port-site hernia for single-port cholecystectomy (8.4%) than for the standard four-port cholecystectomy (1.2%). 9 It was 5.8% and 1.8%, respectively, in another comparative study. 1 Thus, as of mid-2013, the rate of post–single-port surgery incisional hernia appears to be directly proportional to the increasing size of the fascial incision, especially at the inherently weak area like the umbilicus. PUH further adds to the weakness of the umbilical region, thus likely making it more prone for recurrence after single-port surgery. Although high-quality studies are required to settle this controversy, it is likely that reducing the size of fascial cut(s) may play a vital role in decreasing the rate of post–single-port surgery incisional hernia. Therefore, absence of PUH recurrence in our series could possibly be due to the following reasons: (1) we used three small incisions instead of a bigger incision, (2) we performed closure under direct vision of all the three port sites regardless of the caliber of the port, (3) we did not connect the incisions for specimen extraction, (4) >76% of the patients in our series had PUH defects <4 cm in diameter, (5) obese patients with a body mass index of >35 kg/m2 were excluded, (6) prosthetic reinforcement was used for defects 5–8 cm in diameter, and (7) the suboptimal follow-up may have given false-negative results. Nevertheless, the overall trend seems to be on the lower side. However, this study has certain limitations: (1) it is not a randomized trial, (2) the duration of follow-up is inadequate, especially to assess the rate of hernia recurrence, and (3) it lacks a cost–benefit analysis.
Conclusions
For a select subgroup of patients, the single-incision three-port technique described here seems effective, safe, and a valuable choice for concomitant PUH repair and cholecystectomy through the same periumbilical incision using routine laparoscopic instruments. However, further large-volume studies are needed to substantiate these conclusions.
Footnotes
Disclosure Statement
No competing financial interests exist.