
Abstract
Abstract
Aims:
Recent systematic reviews have suggested an increased incidence of intraabdominal abscess (IAA) formation following laparoscopic appendicectomy (LA) compared with the open approach (OA). As the majority of these analyses have focused on appendicectomy in adults, our aim was to review the evidence base for pediatric patients.
Subjects and Methods:
We performed a comprehensive review of relevant studies published between 1990 and 2012. Specific inclusion and exclusion criteria were used to identify studies that investigated the incidence of IAA following LA and OA in pediatric patients. The primary outcome measure in the present meta-analysis was IAA formation, and secondary outcomes included wound infection (WI) and incidence of postoperative small bowel obstruction (SBO).
Results:
Sixty-six studies with a total of 22,060 pediatric patients were included: 56.5% OA and 43.5% LA. There was no overall difference in the incidence of IAA formation: 2.7% for OA (333/12,460) versus 2.9% for LA (282/9600) (P=.25). However, OA patients had a higher incidence of wound infection: 3.7% for OA (337/9228) versus 2.2% for LA (183/8154) (P<.001). Moreover, the incidence of SBO was lower in patients undergoing LA: 0.4% LA (86/5767) versus 1.5% (29/6840) (P<.001).
Conclusions:
The IAA incidence is comparable in LA versus OA in pediatric patients. LA confers a significantly lower risk of other postoperative complications, including WI and SBO.
Introduction
Subjects and Methods
Study design
We performed a systematic review and meta-analysis of all relevant studies published between 1990 and 2012. The main outcome measure was the incidence of postoperative IAA formation following either LA or OA in pediatric patients. Secondary outcome measures included the incidence of WI or SBO in these patients.
Protocol and registration
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was used in the formulation of the systematic review and meta-analysis. 8 The study was not registered with PROSPERO (International Prospective Register of Systematic Reviews), 9 as the study had progressed beyond the point of completing data extraction.
Data sources and search strategy
A review of the literature was performed to identify all published evidence relating to the development of a pediatric IAA postoperatively after either LA or OA. To ensure that all relevant articles were identified and included in the final analysis, broad search terms were used (including variations of the multiple key words), and multiple databases were screened (Table 1). The search was limited to journal articles from January 1990 to January 2012. Studies prior to 1990 were not included as prior to this date LA was not routinely used in children and therefore not reported in the medical literature.
Study selection
Once identification of possible relevant articles had occurred, a single reviewer screened abstracts. Those that related to pediatric LA and/or OA with data reporting on the incidence of postoperative IAA, as well as the incidence of WI and/or SBO, were included. Once the titles and abstracts had been screened and the relevant articles had been identified, full text articles in the English language were retrieved and screened in detail. Abstracts relating to presentations that had not been published in a peer-reviewed journal were not included in the final analysis. When required, authors confirmed details of patient cohort characteristics and outcomes.
Inclusion and exclusion criteria
All studies that included a cohort of pediatric patients having undergone LA or OA with IAA incidence reporting were included. The full inclusion and exclusion criteria are summarized in Table 2. Studies reporting data obtained from coding databases were not included, as the majority focused on the incidence of IAA drainage (rather than the incidence of IAA). In our retrospective review we ascertained that only 28% of patients underwent a surgical drainage of their IAA, and therefore these studies greatly underestimate the true incidence of IAA following appendicectomy in children.7,10 Moreover, studies were excluded if they included patients treated with single-incision laparoscopic surgery. This was to minimize bias, as it is currently unclear whether this technique will influence the postoperative complication rate or IAA formation. Studies were carefully examined for duplication of previously published data.
IAA, intraabdominal abscess.
Data analysis
Data were extracted from the individual studies and collated on a database. The main analysis included data from all studies selected for our systematic review. Subset analyses were performed on (1) studies reporting direct comparisons between LA and OA and (2) patients with complicated appendicitis (presence of perforation, intraabdominal pus, or an intraoperative phlegmon/mass).
Contingency tables were designed for each of the outcome measures, and data were analyzed using Fisher's exact test. ORs and 95% CIs were calculated (an OR of >1 indicated a more favorable outcome for LA compared with OA), and corresponding Forrest plots were constructed using summary data. Publication bias was assessed for each of the outcome measures using funnel plots (OR plotted against corresponding patient number for individual studies). Analysis was performed using GraphPad Prism® (GraphPad Software Inc., La Jolla, CA). P values of <.05 were considered statistically significant.
Results
Study selection
In total, 2874 titles and abstracts were identified from the combined searches from the databases listed in Table 1 for the period from January 1, 1990 to January 5, 2012. From these, 284 full-text journal articles were retrieved and reviewed in detail. Sixty-six of the latter studies contained data that was relevant to the formation of an IAA following a pediatric LA or OA and were therefore included in our analysis. The majority of the articles identified contained Level II-1 or II-2 evidence, with only seven articles containing Level I evidence. The search strategy and results are summarized in Figure 1.

Flowchart of the selection process for studies included in the systematic review and meta-analysis. IAA, intraabdominal abscess; LA, laparoscopic appendicectomy; OA, open approach.
Study characteristics
The 66 studies included in the present analysis contained data on 22,060 pediatric patients who underwent LA or OA for acute appendicitis: LA, 9600 (43.5%); OA, 12,460 (56.5%). Table 3 summarizes data from all studies included in our systematic review and meta-analysis.
Reported values are absolute patient numbers.
IAA, intraabdominal abscess; LA, laparoscopic appendicectomy; ntotal, total number of patients; OA, open approach; SBO, small bowel obstruction; WI, wound infection.
Main analysis outcomes
IAA
Appendicectomy was complicated by IAA formation in a total of 615 of 22,060 patients (2.8%). There was no significant difference between LA and OA in the incidence of postoperative IAA: 2.9% (282/9600) for LA versus 2.7% (333/12,460) for OA (P=.25). The OR (95% CI) for IAA formation was 0.91 (0.77, 1.07) (Fig. 2).
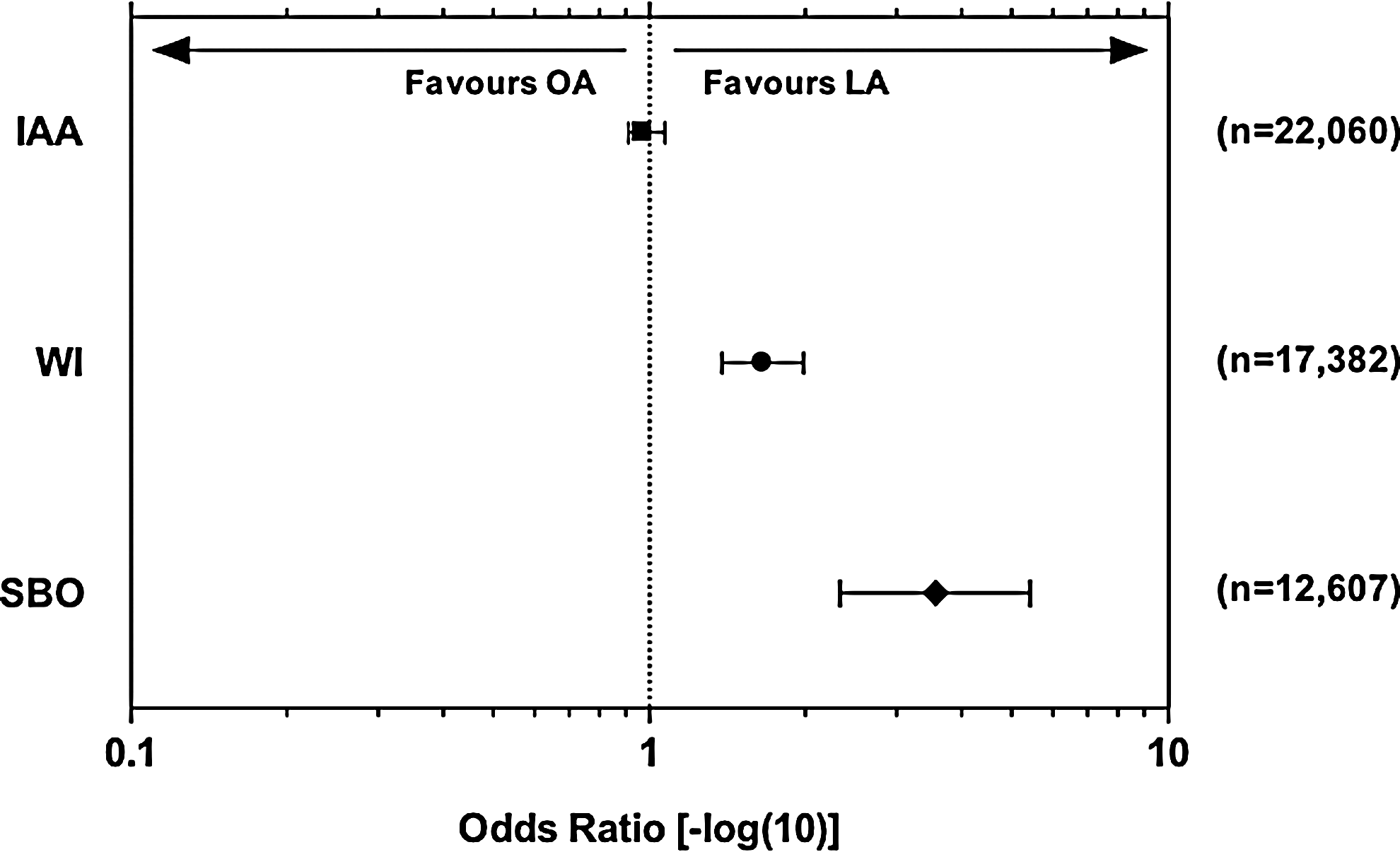
Forest plot of odds ratios (expressed as −log10) for primary and secondary outcome measures from the meta-analysis of 66 studies of laparoscopic appendicectomy (LA) and/or the open approach (OA) in pediatric patients. Error bars represent 95% confidence intervals. An odds ratio of >1 indicates a favorable outcome for LA. IAA, intraabdominal abscess; SBO, small bowel obstruction; WI, wound infection.
WI
Fifty-five of the 66 studies (83.3%) reported data on postoperative WI following LA or OA. The total incidence of WI was 2.9% (520/17,382). WI was significantly less frequent in patients who underwent LA compared with OA: 2.2% (183/8154) for LA versus 3.7% (337/9228) for OA (P<.001). The OR (95% CI) for postoperative WI was 1.65 (1.38, 1.98) (Fig. 2).
SBO
Thirty-four of the 66 studies (51.5%) reported data on postoperative SBO following LA or OA. SBO occurred in 0.9% of the patients (115/12,607). The incidence of SBO was significantly lower following LA compared with OA: 0.4% (29/6,840) for LA versus 1.5% (86/5767) for OA (P<.001). The OR (95% CI) for postoperative SBO was 3.64 (2.37, 5.58) (Fig. 2).
Subset analyses outcomes
Comparative studies
Twenty-nine of the 66 studies (43.9%; n=6931) reported direct comparisons between LA and OA for IAA formation. There was no significant difference in the incidence of postoperative IAA between groups: 3.7% (127/3391) for LA versus 3.9% (138/3538) for OA (P=.78). The OR (95% CI) for IAA formation was 1.04 (0.82, 1.33) (Fig. 3).
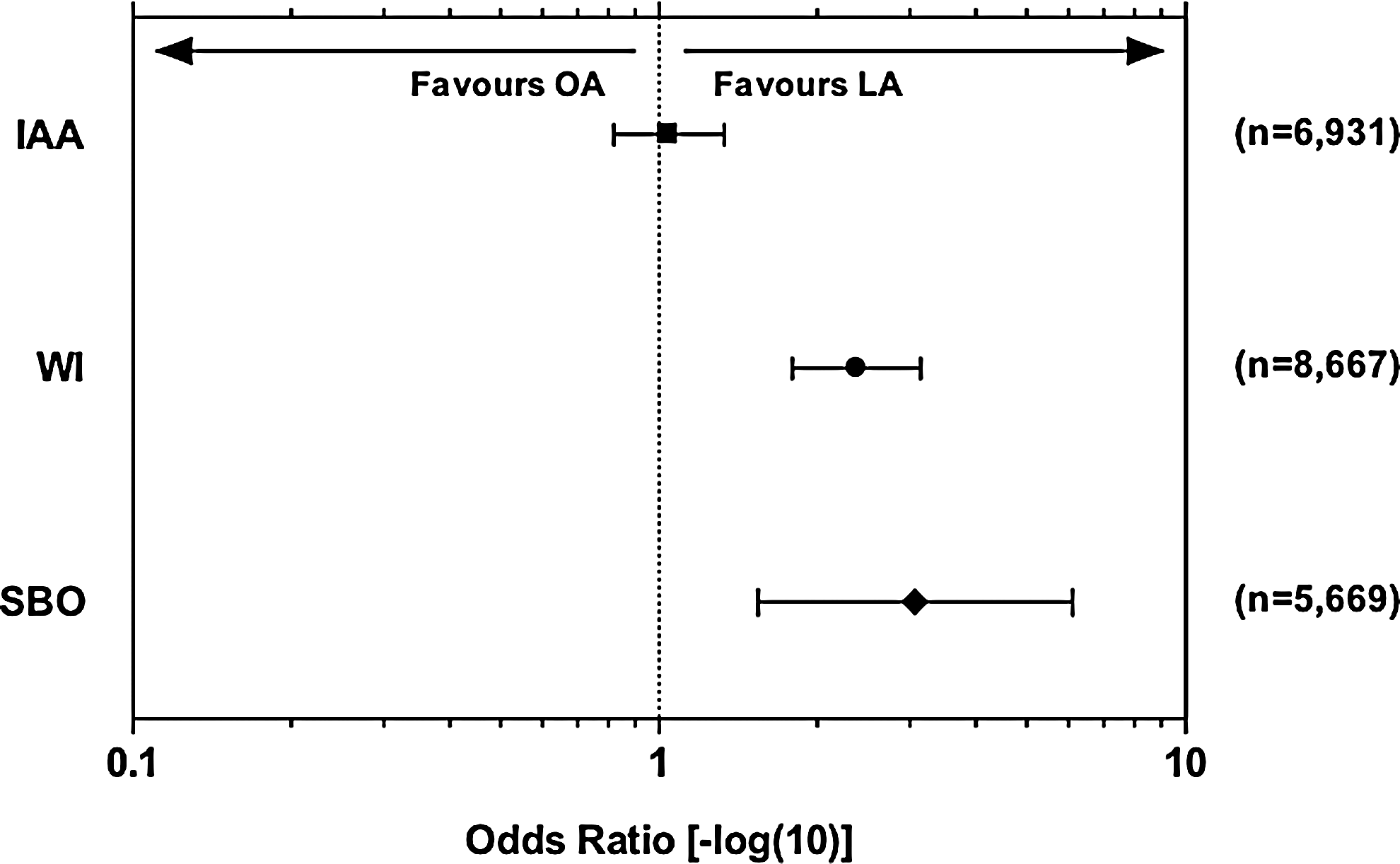
Forest plot of odds ratios (expressed as −log10) for primary and secondary outcome measures from the subset analysis of 29 studies comparing outcomes of laparoscopic appendicectomy (LA) and the open approach (OA) in pediatric patients. Error bars represent 95% confidence intervals. An odds ratio of >1 indicates a favorable outcome for LA. IAA, intraabdominal abscess; SBO, small bowel obstruction; WI, wound infection.
Twenty-four studies (36.4%; n=8667) compared the incidence of WI following LA or OA. OA was associated with significantly higher rates of postoperative WI compared with LA: 1.6% (76/4719) for LA versus 3.7% (148/3956) for OA (P<.001). The OR (95% CI) for postoperative WI was 2.37 (1.79, 3.14) (Fig. 3).
Thirteen studies (19.7%; n=5669) reported comparative data for postoperative SBO following LA and OA. The incidence of SBO was significantly lower following LA: 0.4% (11/2939) for LA versus 1.1% (31/2695) for OA (P<.01). The OR (95% CI) for postoperative SBO was 3.06 (1.54, 6.10) (Fig. 3).
Complicated appendicitis
Forty-one of the 66 studies (62%; n=13,410) reported separate data on IAA formation following LA and OA in complicated appendicitis in children. In these studies, in total, 5467 patients (40.8%) were found to have a perforated appendix, intraabdominal pus, or a phlegmon/mass intraoperatively. LA was associated with a significantly higher incidence of IAA formation in this subset of patients compared with OA: 8.6% (198/2293) for LA versus 5.9% (190/3174) for OA (P<.01). The OR (95% CI) for IAA formation was 0.67 (0.55, 0.82) (Fig. 4). In the 25 studies (38%; n=6822) that reported data on IAA following noncomplicated appendicitis in children, LA was associated with a lower incidence of IAA formation: 0.5% (17/3353) for LA versus 1.0% (34/3469) for OA (P=.026). The OR (95% CI) for IAA formation in uncomplicated appendicitis was 0.52 (0.28,0.92).

Forest plot of odds ratios (expressed as −log10) for primary and secondary outcome measures from the subset analysis of 41 studies comparing outcomes of laparoscopic appendicectomy (LA) and the open approach (OA) in pediatric patients with complicated appendicitis. Error bars represent 95% confidence intervals. An odds ratio of >1 indicates a favorable outcome for LA. IAA, intraabdominal abscess; SBO, small bowel obstruction; WI, wound infection.
Thirty-two studies (48.5%; ntotal=10,251) compared the incidence of WI following LA or OA in complicated appendicitis (ncomplicated appendicitis=4509). LA was associated with significantly lower rates of WI: 3.5% (65/1868) for LA versus 7.1% (176/2641) for OA (P<.001). The OR (95% CI) for postoperative WI was 1.96 (1.46, 2.62) (Fig. 4). With the 23 studies (34.8%, n=6350) reporting the incidence of WI following either technique, there was no difference noted following either modality: 1.0% (29/3009) for LA versus 1.1% (37/3341) for OA (P=.57) (OR 0.87 [95% CI 0.53,1.42]).
The incidence of SBO following LA or OA in pediatric complicated appendicitis was reported in 19 studies (28.8%; ncomplicated appendicitis=4,509; ntotal=7013). There was a trend for a higher risk of SBO following OA compared with LA, but this was not found to be statistically significant: 1.6% (19/1205) for LA versus 2.6% (48/1843) for OA (P=.06). The OR (95% CI) for postoperative SBO was 1.67 (0.98, 2.85) (Fig. 4).
Publication bias
Funnel plots of data from studies reporting direct comparisons between LA and OA in pediatric patients were used to assess for possible publication bias. There was no obvious bias noted for any of the outcome measures of the present meta-analysis (Fig. 5).

Funnel plots for the assessment of publication bias for comparative studies included in the meta-analysis. Odds ratios (laparoscopic appendicectomy versus the open approach; expressed as −log10) were plotted against the total patient number (expressed as log10) for individual studies:
Discussion
Several interesting points are raised by this review. The first is that there is a scarcity of Level I evidence for the treatment of pediatric acute appendicitis by either operative modality, despite this condition being one of the most common emergencies that a pediatric surgeon will encounter. One possible reason for this is that the power needed for a well-constructed randomized controlled trial is thousands of patients, as the difference in incidence between the two techniques is minimal in some of the larger comparative retrospective reviews.7,11 This is obviously difficult to achieve even in a multicenter pediatric study. A well-constructed multicenter prospective trial may be the highest level of evidence in an individual study on this topic.
We have also found that when all the patients are analyzed, there is no difference between the IAA incidences following either LA or OA in a pediatric patient. This is in contrast to the findings of the Cochrane review. 3 There is also a protective effect of using the laparoscopic technique in terms of the occurrence of WI or SBO in the postoperative period. The subset analysis revealed that there is a greater incidence of IAA formation following LA in patients presenting with complicated appendicitis. This may potentially be explained by the increased time required for a thorough washout with the LA technique, or that there may be a negative effect on the pneumoperitoneum on the intraperitoneal distribution of purulent material.12,13 However, there is a lack of a standardized definition of complicated appendicitis in the 41 studies included in this subset analysis, which limits the interpretation of these data. As overall there is no difference in the IAA incidence, patients from these two subgroups may have been included in different analysis groups in the various studies, making the subset analysis potentially biased. This issue will need to be addressed in a future well-constructed prospective randomized trial using a standardized definition of complicated appendicitis.
This systematic review included studies over a significant period of time, and therefore undoubtedly there is inclusion of the learning curve in the technique of pediatric LA. As the majority of included studies grouped patients with an intention-to-treat basis, this is unlikely to have affected the overall results.
There was a decreased WI incidence noted after LA both when the whole cohort was analyzed and also with the complicated subset analysis. As the majority of studies included in this systematic review did not contain Level I evidence, there will undoubtedly be an element of bias in terms of the WI incidence. With either an IAA or SBO the patient will be likely to re-present to the pediatric surgical center; with WI, however, different follow-up practices and treatment at the primary healthcare level will influence the accurate reporting of this complication.
With the analysis of all patients, the incidence of SBO is decreased following LA compared with OA. The complicated appendicitis subset analysis revealed no difference, which may indicate that the underlying disease process rather than the technique used is the most important factor in the formation of this postoperative complication.
This review was centered specifically on the incidence of IAA and other postoperative complications rather than other traditional outcome measures such as the length of hospital stay and the individual operative duration. The length of hospital stay is an inaccurate comparative factor for pediatric patients. The presence of complicated appendicitis and therefore the length of the indicated intravenous antibiotics course determine the length of hospital stay, rather than the operative modality. The operative time also was not used, as this has become comparable in recent trials, and only serious complications should dictate the surgical approach. There is a much larger debate centered over the differences between the laparoscopic approach and the OA, which include the financial cost, cosmetic result, and increased visualization for alternate pathology, but these are beyond the scope of this review. These are, however, important factors to be considered when comparing the laparoscopic approach and the OA.
Overall, this systematic review of pediatric patients has shown that there is no difference between the LA and OA techniques in terms of IAA formation, which is different from the findings of the Cochrane review. 3 The LA technique decreases the incidence of WI and also has a protective effect on the formation of postoperative SBO.
Footnotes
Disclosure Statement
No competing financial interests exist.