
Abstract
Abstract
Objective:
To compare muscular fatigue and postural stability of surgeons before and after laparoscopic and robotic surgery.
Subjects and Methods:
The design of this study is Class II. A consecutive cohort of patients presenting at an academic tertiary-care center for scheduled gynecologic surgery was used. Routine surgical care was examined with testing of surgeon fatigue and postural measures before and after the procedure. Motor fatigue was measured using a quantitative grip dynamometer, and postural stability was measured using a nondominant, single-leg stance. A subjective fatigue score was recorded following surgery.
Results:
Primary surgeons completed testing before and after 56 surgeries. A trend toward decline in postural stability was observed more in the laparoscopy group than in the robotic group (P=.29). The fatigue index and subjective fatigue scores were not significantly different.
Conclusions:
Similar changes in postural stability and muscular strength were observed following laparoscopic and robotic surgery. The optimal measurement tool to capture surgical fatigue remains elusive. Fatigue differences may have been more pronounced if surgical procedure degree of difficulty had been more consistent between groups.
Introduction
Many studies exist comparing the surgical outcomes between laparoscopy and robotics, but few have compared the physical strain on the practicing surgeon.5–7 Additional studies have displayed improved technical performance and reduced physiologic stress using robotics compared with laparoscopy.8,9 Robotic surgery has preserved the advantages of laparoscopic minimal invasive surgery, but also offers the surgeon less ergonomic constraints: operating in sitting position, increased degrees of freedom, three-dimensional visualization through the console, and minimal or no resistance upon movement of instruments. 10 We hypothesize that the ergonomic constraints of laparoscopy may result in undue surgeon fatigue and injury that may be overcome with the use of robotic technology. The aim of this study was to compare surgeon muscular fatigue and postural stability before and after laparoscopic and robotic surgery.
Subjects and Methods
Measures of muscular fatigue and postural stability were collected before and after laparoscopic and robotic cases among six gynecologic surgeons at a single institution. Consecutively scheduled laparoscopic or robotic surgeries were offered inclusion if the anticipated operative time was greater than 30 minutes. The study was approved by the Institutional Review Board (protocol number 10-000543), and patients were made aware of the study protocol and offered the option to decline participation. The da Vinci® Surgical System (standard) and S systems were used for robotic cases (Intuitive Surgical Inc., Sunnyvale, CA). Muscle fatigue was measured using a Jamar® hydraulic hand grip dynamometer (Sammons Preston Rolyan, Chicago, IL) with analog output and graphic analysis. Using the surgeon's dominant hand, a maximum grip was sustained for 30 seconds. The maximum voluntary isometric contraction force was used to calculate a fatigue index. The fatigue index model has been shown to provide optimal test–retest reliability and sensitivity for detecting increased fatigue. Quantitative muscle analysis software (QMA®; Aeverl Medical, Gainesville, GA) plotted curves of force versus time (Fig. 1). 11 Static fatigue was expressed as a fatigue index, defined as the percentage of maximum voluntary isometric contraction unable to be sustained over a 30-second period.
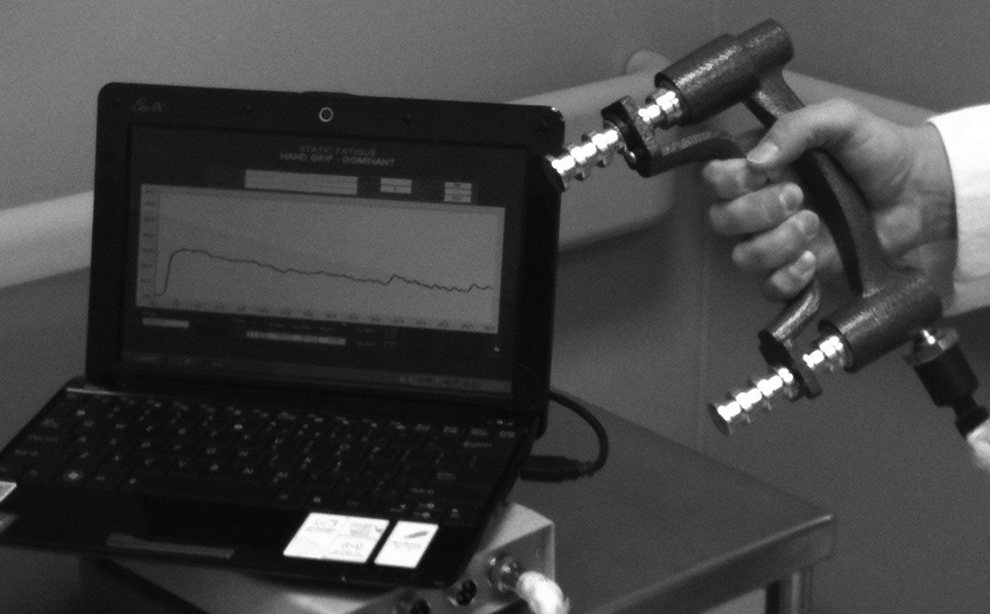
Quantitative muscle analysis: plotted curve of force versus time.
Postural stability was measured using a nondominant, 20-second, single-leg stance on a foam pad. 12 The hip was flexed 30°, and the knee was flexed 45°. Hands rested on the hips, and eyes were closed. The nondominant leg was defined as the opposite leg preferred for kicking. An unstable foam surface provided a more challenging balance task compared with a firm surface. A balance error scoring system (BESS) was used, and a postural stability score was recorded for the subject when any of the following occurred: opening the eyes, step stumble or fall, moving the hands off of the iliac crests, abduction or flexion of the hip beyond 30°, lifting the forefoot or heel off of the testing surface, or remaining out of the proper testing position for greater than 5 seconds. The maximum total number of points was 10. When multiple errors occurred simultaneously, only one error was recorded. Subjects were given 5 seconds to resume appropriate positioning following deviation before additional error points were collected. Higher BESS totals indicate decreased postural stability. The BESS has been shown to reliably evaluate postural stability as a result of fatigue. 13 Perceived overall mental and physical fatigue was documented using a subjective visual analog scale fatigue score by the surgeon following surgery. A 10-cm-long horizontal line with end points labeled as “no fatigue” and “severe fatigue” was marked. Scores were categorized as mild, moderate, and severe for analysis.
Changes of postoperative measures from baseline including the fatigue index, maximum voluntary isometric contraction, area under the curve, and postural stability were compared between the laparoscopic group and robotic group using the Wilcoxon rank-sum test. Visual analog perceived fatigue scores were compared using a χ2 test. Subgroup analysis was also performed looking at patient body mass index greater than 25 kg/m2 and length of surgery greater than 60 minutes, and the Wilcoxon rank-sum test was used to compare group differences. Comparisons in body mass index and length of surgery between groups were performed by the Wilcoxon rank-sum test. P values of<.05 were considered statistically significant. All analyses were performed using SAS version 9.2 software (SAS Institute, Cary, NC).
Results
Primary surgeons completed testing before and after 56 consecutive cases meeting inclusion criteria (71% robotic, 29% laparoscopic). All six surgeons were subspecialty trained in gynecologic oncology and/or urogynecology. Four were staff attending surgeons, and two were fellows. Surgical procedures included hysterectomy, oophorectomy, sacrocolpopexy, lymphadenectomy, trachelectomy, vaginectomy, ovarian cystectomy, excision of endometriosis, presacral neurectomy, and appendectomy (Table 1). In some cases more than one procedure was performed on a single patient. More procedures requiring advanced dissection were performed robotically. There were no significant differences between laparoscopic and robotic procedures in patient body mass index (median, 26.5 and 25.2 kg/m2, respectively) or length of surgery (median, 89 and 114 minutes, respectively).
Postural stability decreased more in the laparoscopy group than the robotic group with balance error scores 33% higher following laparoscopy (P=.29). Fatigue index scores were not significantly different between groups, with the mean grip strength changing less than 1 kg between measurements before and after surgery (P=.96) (median pre- and postoperative fatigue indices: laparoscopy, from 25.17% to 26.49%; robotic, from 26.21% to 26.40%). The subjective visual analog scale fatigue scores were not significantly different (for laparoscopic versus robotic: mild fatigue, 50% and 41%, respectively; severe fatigue, 13% and 15%, respectively). Over 75% of cases lasted greater than 60 minutes.
Discussion
Similar changes in postural stability and muscular strength were observed following laparoscopic and robotic surgery. Significant mental and physical elements are used during laparoscopic and robotic surgery, and the optimal measurement tool to capture surgical fatigue remains elusive. Postural control is maintained through the contribution of many body systems, including musculoskeletal, neuromuscular, and sensorimotor integration, making postural control a testable modality to evaluate global fatigue. Balance has been shown to decrease reliably following muscle and central fatigue. 13 A slight, but insignificant, decline in balance function was observed in our study following laparoscopic surgery, suggesting that whole body fatigue may be experienced but was perhaps unrecognized because of insufficient power. Despite laparoscopic surgeons having performed less complex surgery (Table 1), their postural stability declined compared with that during robotic surgery. Fatigue differences may have been more pronounced if surgical degree of difficulty had been more consistent between groups. Less fatigue was reported by urologic surgeons (n=73) following robotic surgery compared with laparoscopy. 3
Fatigue has many subjective and physical dimensions. Motor fatigue, defined as the loss of the maximal capacity to generate force during exercise, is the most amenable to physiologic analysis. Motor fatigue has been assessed using a variety of techniques to provoke and to measure a decline in function over time.11,14 The portable quantitative muscle analysis system with hand grip dynamometry has been shown to be a reproducible and rapid test.15,16 Isolated muscular weakness in grip strength did not reveal significant decline between groups. Muscle weakness can be measured as a reduced force output with loss in maximum voluntary isometric contraction and may not therefore correlate with the calculated fatigue index. 17 The ideal test offering both reproducibility and accuracy in capturing surgeon fatigue has yet to be established.
Strengths of our study included a diverse variety of procedures and degrees of difficulty. Surgeons studied had varying levels of experience and training with both surgical approaches. Study limitations included a limited and unequal volume of laparoscopic and robotic surgeries for comparison. Our surgical practice adopted the use of robotic technology in 2003, and its use supersedes laparoscopy, particularly when complex dissection is anticipated. This introduces bias toward robotic use; however, all surgeons routinely perform laparoscopic cases annually. An a priori power analysis proposal was not reached during the allotted time that study funding was available. A projected sample of 48 cases was planned: 24 laparoscopic and 24 robotic. Additionally, the operative case time of day was not captured. Cases performed later in the day may have resulted in different changes in fatigue than those cases that began first in the morning. Moreover, any test with repeated performance may be learned over time. Surgeons undergoing repeated task testing may experience a “practice effect,” thereby masking more significant fatigue and postural deficits. 13
Conclusions
In conclusion, laparoscopic surgery resulted in similar surgeon postural stability compared with robotics. No difference was noted between groups for isolated muscular strength. Fatigue differences may have been more pronounced if surgical degree of difficulty had been more consistent between groups. The ideal test offering both reproducibility and accuracy in capturing surgeon fatigue has yet to be established.
Footnotes
Acknowledgments
This project was funded by the Mayo Clinic Foundation. Sincere appreciation is extended to the Departments of Gynecology and Surgical Services, Mayo Clinic Hospital in Phoenix, AZ, and Drs. Francesc Fargas Fàbregas, Clare Colome, and Marta Carrasco for their time and effort.
Disclosure Statement
No competing financial interests exist. All authors contributed to the study design, analysis, and manuscript completion.