
Abstract
Abstract
Background:
Chronic wound discomfort and intercostal neuralgia are well-known postoperative complications of video-assisted thoracoscopic surgery (VATS). To explore the possibility of a surgical platform that would cause less postoperative discomfort and avoid these complications, this study evaluated the feasibility of transumbilical lung wedge resection in a canine model.
Materials and Methods:
Twelve dogs (4 in the nonsurvival group and 8 in the survival group) were used in this study. Transumbilical thoracoscopy was performed using a homemade metallic tube via umbilical and diaphragmatic incisions with the animal in a supine position. After thoracic exploration, wedge resection was performed on the lung using an endoscopic stapling device placed through the transumbilical and transdiaphragmatic incisions under direct bronchoscopic guidance. The animals were sacrificed 30 minutes after the procedure (nonsurvival group) or 14 days postsurgery (survival group) for necropsy and histological evaluations.
Results:
Eleven preplanned lung wedge resections were completed in a median time of 101 minutes (range, 65–175 minutes) with one exception due to inadequate stapling in the early phase of the experiment. There was one death directly related to postoperative massive airleaks and sepsis in the survival group. The other 7 animals had an uneventful postoperative period. Necropsies at 2 weeks after surgery confirmed successful lung resections and revealed no evidence of vital organ injury. Two animals exhibited complete healing of the diaphragmatic incision. Liver herniation was identified in 1 of 5 animals with partial wound healing.
Conclusions:
This preliminary animal study demonstrates that large lung wedge resection can be performed with mechanical staplers via a single transumbilical incision. Future studies will investigate the cardiopulmonary and immunologic effects of transumbilical VATS compared with conventional VATS.
Introduction
Because this approach has never been previously used, we aimed to evaluate the feasibility of transumbilical lung wedge resection in a canine model. The main goal was to collect evidence that might enable the introduction of transumbilical thoracoscopy into clinical practice.
Materials and Methods
The study was conducted in the animal laboratory center of Chang Gung Memorial Hospital (Taoyuan, Taiwan) with the approval of the local ethics committee on animal research. The study was conducted in two parts: Part 1 comprised an acute study including 4 beagle dogs conducted to practice lung resection with endoscopic stapling devices via a transumbilical incision, and Part 2 comprised a survival study performed in 8 living beagle dogs to evaluate the feasibility of lung wedge resection via a transumbilical incision.
With the animal in the supine position, surgery was carried out using 2% isoflurane general anesthesia with a 5.0-mm homemade endotracheal tube selectively intubated to the contralateral main bronchus for single-lung ventilation (tidal volume, 15 mL/kg; respiratory rate, 12/minute). The pre-anesthesia medication consisted of an intramuscular injection of ketamine (5 mg/kg) and xylazine HCl (5 mg/kg). An intravenous line was placed in the cephalic vein, and a single dose of antibiotic (cefamezin, 20 mg/kg) was injected intravenously before the procedure to reduce the risks of infection. After closure of the umbilical wound, 2% xylocaine (0.6 mL) was injected subcutaneously. Acetaminophen (25 mg/kg, daily) was used for additional pain relief after surgery.
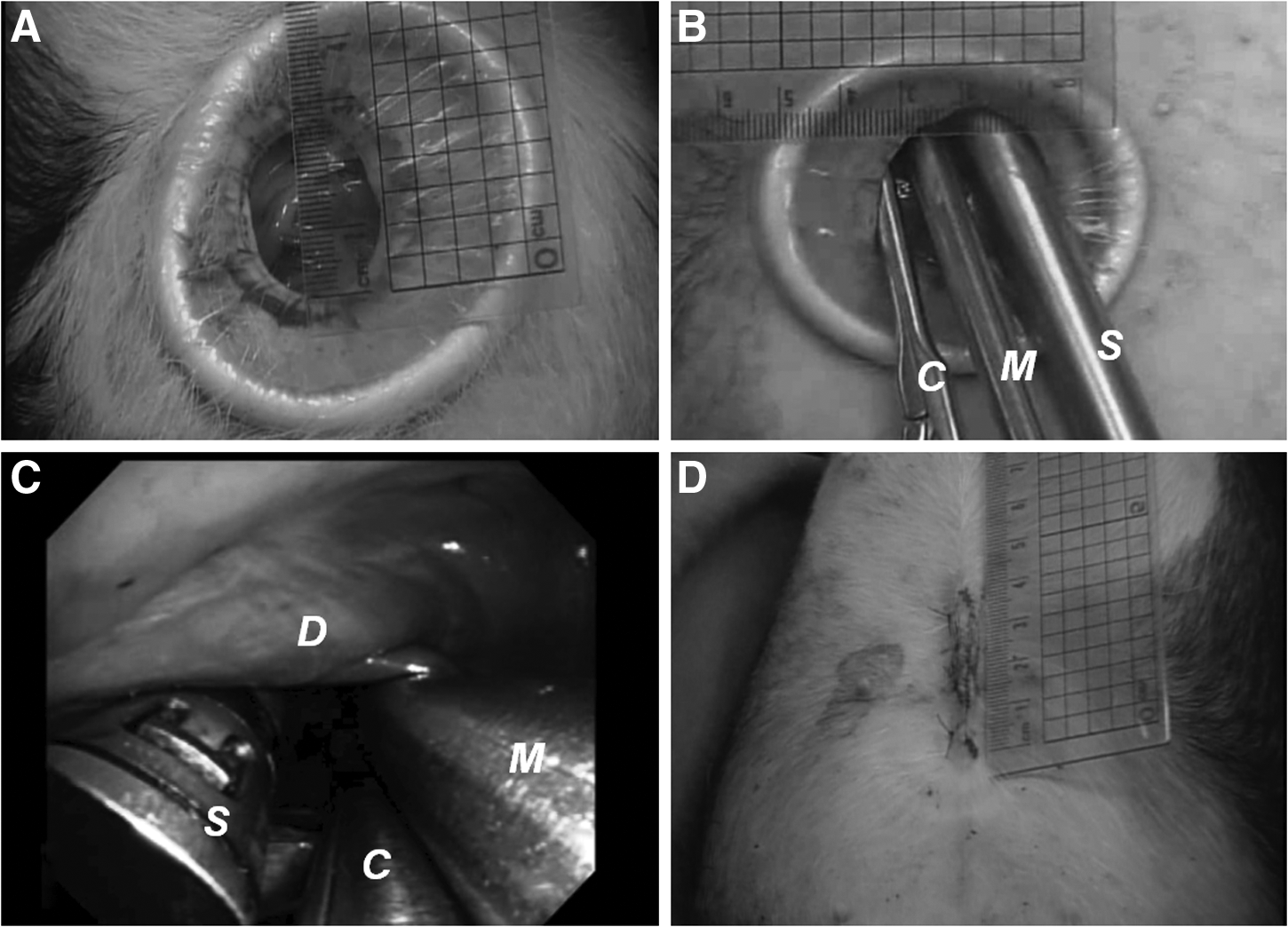
The predetermined wedge lung resections were performed in four right upper lobes in the acute study and in four right upper lobes (one right middle lobe, one right lower lobe, one left upper lobe, and one left lower lobe) in the survival study. With the animal in the supine position, the following steps were used in order to perform lung resection: (1) A 2–3-cm longitudinal incision was made through the umbilicus and drawn down to the peritoneum. (2) The umbilicus incision was retracted using a wound protector (Alexis® wound retractor; Applied Medical, Rancho Santa Margarita, CA) and used as the entrance for the lung wedge resection. (3) The bronchoscope (outer diameter, 4.9 mm; Olympus Optical Co Ltd., Tokyo, Japan) was inserted through the umbilical incision for abdominal cavity exploration and the diaphragmatic incision. (4) A needle knife (Olympus Optical Co., Ltd.) was inserted through the working channel of the flexible bronchoscope to perform a diaphragmatic incision at the junction of the diaphragm and subxiphoid process. (5) The diaphragmatic incision was sequentially dilated to accommodate a 9-mm homemade metal tube for exploration of the pleural cavity. (6) A second diaphragmatic incision was made 3 cm lateral to the first diaphragmatic incision and sequentially dilated to accommodate a 15-mm homemade metal tube for insertion of the staples (staple length, 45 mm; staple leg, 2.5 mm; Ethicon Endo-Surgery, Cincinnati, OH) and lung resection. (7) The flexible bronchoscope was introduced into the thoracic cavity through a 9-mm homemade metal tube for selection of the predetermined wedge resection lung lobe. (8) Staples were inserted through the 15-mm homemade metal tube to perform a lung resection. (9) An endoscopic lung grasping clamp was also inserted adjacent to the 15-mm working port to position the targeted segment between the linear stapler. (10) The security of the resected lung margin was checked under water for any air leaks. (11) The metal tube was removed under direct bronchoscopic guidance, and the animal was monitored for vital organ injury. (12) The diaphragmatic incision was allowed to heal through the normal healing processes. (13) The umbilical incision was closed with a 3-0 nylon suture.
In the acute study, the animals were euthanized with intravenous xylocaine (200 mg) 30 minutes after surgery. A necropsy was performed to evaluate the success of the procedure and check for evidence of intrathoracic organ injury. The 8 animals in the survival study were extubated immediately after surgery and allowed to resume a normal diet 8 hours after surgery. The animals were closely monitored for signs of respiratory distress, postoperative infection, or bleeding complications. Rectal body temperature and respiratory rate were measured before surgery and 1, 3, 7, and 14 days after surgery. To evaluate the impact of transumbilical lung wedge resection on respiratory function, arterial blood gasses were measured preoperatively, postoperatively, and at Day 14. Blood was also obtained for the measurement of complete blood count, C-reactive protein level, and interleukin-6 level before surgery and 1, 3, 7, and 14 days after surgery to evaluate the inflammatory response. The animals were sacrificed at 2 weeks and examined for surgical outcome. Success of the procedure, signs of infection, surgical complications, and healing of the diaphragmatic incision were evaluated.
Results
General measurements (Table 1)
Transumbilical exploration of the thoracic cavity and access to a predetermined lung lobe were achieved successfully for all animals (n=12). The mean operating time was 101 minutes (range, 65–175 minutes). There was one major complication (massive airleaks leading to death) in the survival study. The other 7 animals in the survival group exhibited uneventful good clinical recovery by the end of the study (14 days). The median weight gain after surgery was 0.6 kg, representing a 9% increase compared with presurgery weight.
LLL, left lower lobe; LUL, left upper lobe; RLL, right lower lobe; RML, right middle lobe; RUL, right upper lobe.
Biopsy (Figures 1–4)
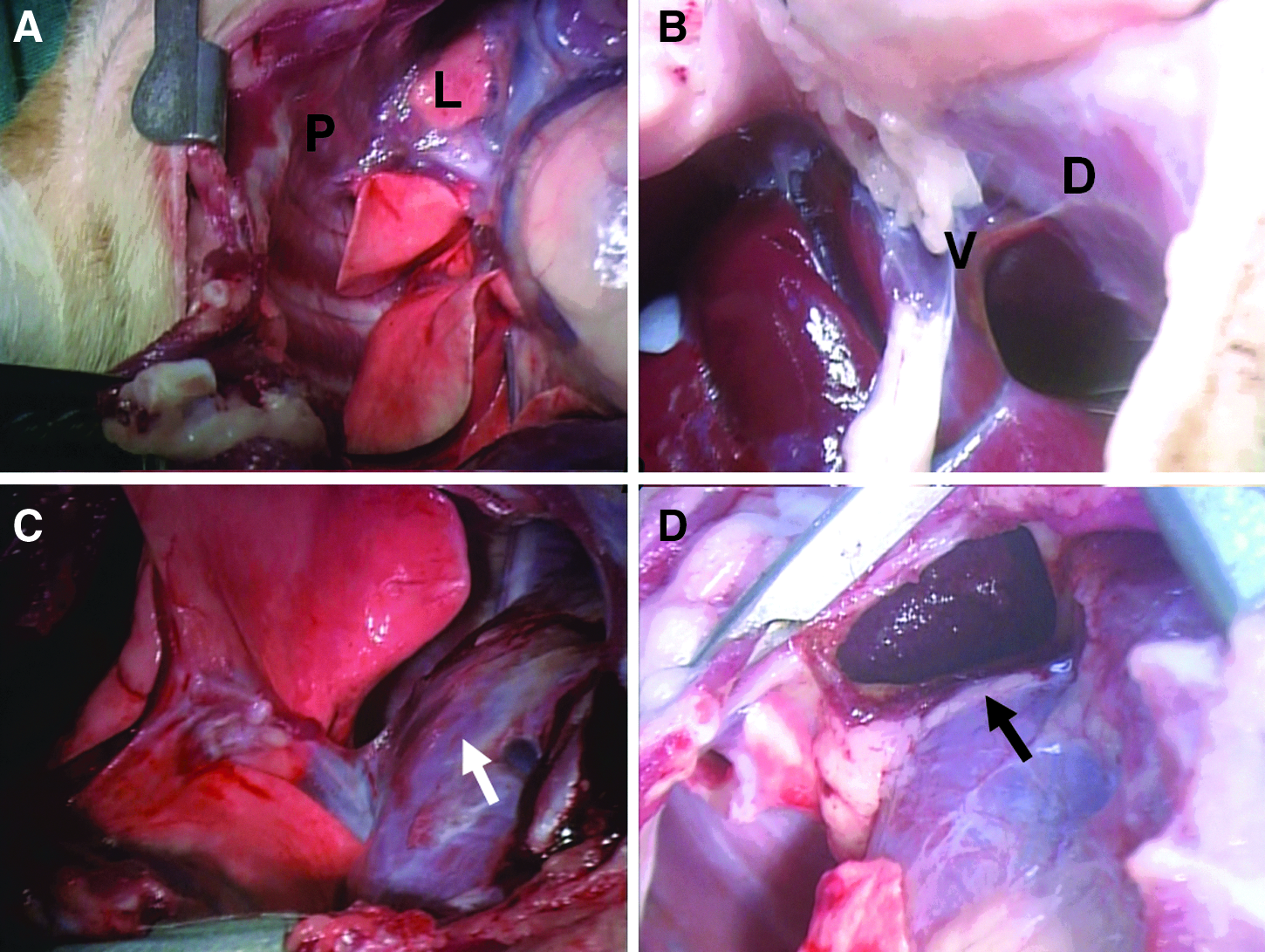
Exploration of the upper and middle parts of the thoracic cavity was easily achieved with a flexible bronchoscope. Access to the lower portion of the thoracic cavity was limited because of a partial blockage of the surgical field by the heart and liver. However, all 12 predetermined lung lobes were successfully identified, and lung wedge resections were successfully performed using endostaplers in 10 of 12 animals through an umbilical incision and two diaphragmatic incisions. In an animal in the acute study, we observed an incomplete lung resection because of insufficient stapling in the early phase of the experiment. One animal in the survival study received lung resection by stapler, concurrent with an electrocautery snare. This animal required three endoloop ligatures because of air leak from the resected margins. The median length of the specimen was 5.6 cm (range, 3.5–8.0 cm).

Operating room setup.


Physiological parameters (Fig. 5)
Changes in respiratory rates and rectal temperature are shown in Figure 5A. The respiratory rates rose above normal on Days 1–7 and returned to normal 14 days after surgery. The change in the rectal temperature before and after surgery was not statistically significant (Fig. 3B).

Change in
Pulmonary parameters (Fig. 6)
There was a significant decrease in the pH values and a significant increase in arterial pressure of CO2 values immediately after surgery. However, both values returned to the preoperative levels on Day 14 after surgery. The arterial pressure of O2 values were increased over preoperative levels immediate after the surgery; however, there was no significant difference in the these values before surgery and Day 14.

Change in arterial blood gasses in the 7 animals that survived transumbilical lung wedge resection. Data are mean values±95% confidence interval (n=7). *P<.05, compared with previous time point; #P<.05, compared with preoperative (Pre-OP), by Wilcoxon signed-rank test. paCO2 and paCO2, arterial pressure of CO2 and O2, respectively; Post-OP, postoperative.
Inflammatory parameters (Fig. 7)
Changes in white blood cell levels are shown in Figure 7A. The white blood cell level was elevated 1 day after surgery and gradually returned to preoperative levels 2 weeks after surgery. As shown in Figure 7B, the plasma levels of C-reactive protein increased significantly 1 day after surgery and returned to preoperative levels on Day 7. Changes in interleukin-6 levels are shown in Figure 7C. The serum concentration of IL-6 was significantly elevated in the early postoperative period and returned to preoperative levels 3 days after surgery.

Change in

Complications
One massive airleak complication was encountered in the survival study. This complication resulted from resection of lung parenchyma using an electrocautery snare in the early phase of the experiment. Pleural drainage was required after surgery to prevent a tension pneumothorax. This animal had lethargy and poor peroral intake during the postoperative course and died 5 days after surgery because of sepsis and respiratory failure. Other animal had air leaks due to accidental injury of the right middle lobe during bronchoscopically evacuation of effusion after lung resection. A 1-cm laceration over the right middle lobe was repaired by partial lung resection using the endostapler. This animal had uneventful clinical course during the 2-week postoperative examination.
Necropsies (Fig. 8)
Necropsies of the 4 animals in the acute study confirmed corrected lung resection and an absence of intrathoracic organ damage. In the animal with an incomplete lung resection, there was a 2-cm residual lung parenchyma at the planned resection line on the right upper lobes. In the 8 survival study animals, postmortem examinations confirmed success in lung wedge resections and no evidence of injury to the thoracic and mediastinal structure in the 7 surviving animals. The animal that died 5 days after surgery had a complete collapse of the right lung with massive purulent effusion. During necropsy, 4 of 7 surviving animals had pleural or mediastinal adhesions on the stapling line, 4 of the 7 animals had liver adhesion in the diaphragmatic incision region, and 1 of the 7 animals had adhesion between the lung and the diaphragm. During necropsy, complete healing of the diaphragmatic incision was observed in 2 animals; partial healing was seen in 5 animals, and 1 of them had liver herniated into the right hemithorax.
Histology (Fig. 9)
Histopathologic examination of the diaphragmatic incision region was performed in the 7 animals that survived for 2 weeks after surgery. All specimens exhibited inflammation, fibrosis, and no evidence of infection or abscess formation. With regard to microscopic findings, inflammation, fibrosis, and liver adhesion were observed in all 7 animals, mesentery adhesion was present in 1 animal, pleural adhesion was noted in 1 animal, and lung adhesion was found in 1 animal.
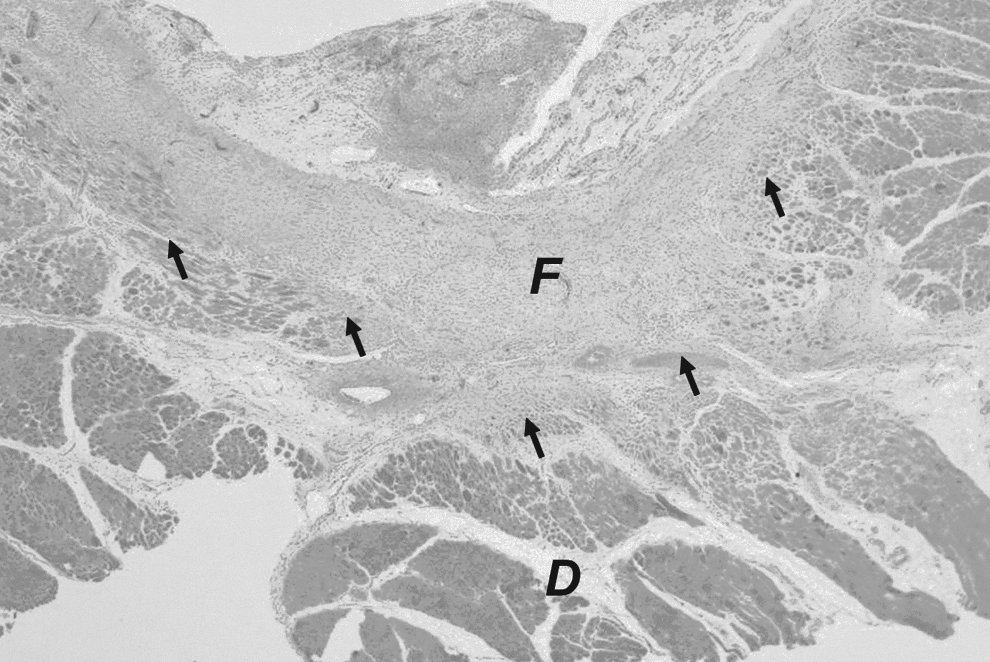
Histological examination showed inflammation and fibrotic healing (F) over the region of the diaphragmatic incision. D, diaphragm. Black arrows indicate the healing margin.
Discussion
Currently, most thoracic surgical procedures are performed thoracoscopically. Two troublesome complications of chronic thoracotomy—discomfort and intercostal neuraglia, occurring in 10%–23% of patients—have been described in the literature.1,3,7 To further minimize the postsurgery discomfort caused by the transthoracic approach, the next logical step is the invention of an alternative platform for performing endoscopic surgery in the thoracic cavity. As advances have been made in laparoscopy, the use of the abdominal rather than the transthoracic access is a reasonable and acceptable approach to reducing thoracotomy complication and achieving better cosmetic results. In this study, we found transumbilical thoracoscopic lung resection to be technically feasible in dogs.
Many surgeons have reported their clinical experiences of accessing the pleural cavity and performing thoracic procedures using the laparoscopic approach. Tsubokawa et al. 8 performed thoracic duct clipping for persistent chylothorax after extrapleural pneumonectomy using laparoscopy. Tanaka et al. 9 performed posterior mediastinal tumor removal via the transdiaphragmatic approach, using two or three abdominal trocars. Moskowitz et al. 10 reported the transdiaphragmatic robotic-assisted laparoscopic resection of a left thoracolumbar neurofibroma in a male patient without complications. Aujesky et al. 11 further described good outcomes following video-assisted laparoscopic resection of the esophagus for carcinoma after neoadjuvant therapy in 43 patients. We believe that well-developed endoscopic devices can provide rapid and secure lung resection via a single transumbilical incision, as achieved in the current study.
The healing of diaphragmatic wounds after surgery was a major concern in this study. Based on our previous experience of transumbilical thoracoscopy, the diaphragmatic wound was left to heal spontaneously, and we found that the vast majority of diaphragmatic wounds did not heal well. In addition, 1 animal exhibited visceral herniation complications. Therefore, we can conclude that diaphragmatic repair is mandatory in larger incisions after surgery in order to ensure efficient healing and minimize complications. Many authors have reported their clinical experiences of laparoscopic repair of diaphragmatic injury. Marks et al. 12 reported that diaphragmatic laceration after penetrating trauma was successfully repaired using the laparoscopic technique. Koehler and Smith 13 used the thoracoscopic approach to repair a diaphragmatic rupture following gunshot injury. Shaw et al. 14 further presented their experience of successful laparoscopy-assisted repair of diaphragm injuries in 24 patients. More recently, Danelson and Chandler 15 also reported that the single transumbilical approach is feasible and safe in performing endoscopic repair of diaphragmatic defect in a pediatric patient with Morgagni diaphragmatic hernia. This evidence suggests that diaphragmatic postsurgical wounds can be managed by laparoscopic intracorporeal suturing without any difficulty. Furthermore, the use of endoclips may simplify surgery.
In this study, standard pleural drainage was not used because drainage causes acute post-thoracotomy pain. Chronic post-thoracotomy pain was also a concern because thoracotomy incisions can damage the intercostal nerve and lead to chronic neuropathy. Therefore, pneumothorax and fluid collection after surgery represented major challenges after lung resection in the current study. However, Satherley et al. 16 reported that the use of an intercostal chest drain after lung biopsy increases the period of hospitalization. In contrast, Nakashima et al. 17 reported that omitting chest tube placement did not increase postoperative morbidity after thoracoscopic lung wedge resection in 76 patients. Similarly, Luckraz et al. 18 performed a randomized control trial in 60 patients and found that there is no need for an intercostal chest drain in patients receiving VATS lung resection if no air leak is noted at surgery. In the present study, we achieved similar results: a postmortem examination of the 7 animals that received lung resection stapling showed no signs of lung atelectasis, intrapleural fluid collection, or infection 2 weeks later. This study demonstrates the safety and efficacy of transumbilical endoscopic stapler lung resection without chest tube drainage in a canine model. Furthermore, simple pneumothorax and effusions were successfully treated with pigtail drainage.
Iatrogenic injury is another concern during access of the thoracic cavity. To prevent the inadvertent injury of intrathoracic structures, all procedures (diaphragmatic incision, thoracic cavity accession via the peritoneal cavity, and lung resection with mechanical staplers) were completed under direct view. The use of transdiaphragmatic access to the thoracic cavity via transumbilical incision was similar to our previously described technique of applying the transoral approach to the thoracic cavity. 19 In brief, the metallic tube was used to establish a working tract between the prepericardial and substernal space via the diaphragmatic incision (the ventilator was turned off to decrease the risk of lung injury during introduction of the metallic tube into the pleural cavity). This technique allows both thoracic exploration and excision of the predetermined lung lobe and completely eliminated organ injury in our study.
The stapler remains the gold standard for both lung resection and airleak management, but various techniques including ligation, suturing, and coagulation have been reported in several patient series.20,21 We have used endoloop ligation in the management of bullae in primary spontaneous pneumothorax since 1993 and have found it to be an inexpensive, safe, and effective technique in preventing primary spontaneous pneumothorax recurrence. Sawabata et al. 22 performed heat ablation of broad-base superficial bullae and achieved effective control of the air leak in patients with spontaneous pneumothorax. In contrast, Lewis et al. 21 used an argon beam coagulator in the treatment of patients with end-stage bullous disease and encountered postoperative air leakage in 8 of 10 patients. In the present study, we found that resection of lung parenchyma using electrocautery does not provide reliable closure of air leaks and led to the development of massive airleaks and consequent mortality. These results demonstrate that correct selection of the optimal endoscopic device to seal and prevent airleaks following lung resection is an important part of the surgeon's armamentarium. Similarly, intervention using simple, reliable, and secure endoscopic devices may facilitate the development of a novel and less invasive platform for thoracic intervention and surgical lung resection.
There are three potential advantages of transumbilical thoracoscopic lung resection. First, the skin of the umbilical area is less innervated than the rest of the abdominal and chest wall and may cause less postoperative pain than traditional VATS in the early postoperative period. Second, this approach eliminates the chest wall incision and avoids the potential complications of thoracotomy, including respiratory problems and intercostal neuraglia. Third, the operation can give a more cosmetically pleasing result after surgery as the incision can be hidden in the umbilicus.
This study had some limitations. First, there was restricted surgical vision during the lung resections and restricted movement of the endoscopic staplers because of collisions between the staplers and the bronchoscope. Future studies with a larger number of subjects should be conducted to find a solution for this issue. Second, lung resection requires two operators skilled in endoscopy: one to introduce and fire the endoscopic staplers and another to maintain endoscopic visualization. Third, resection of the lower lung region could be restricted by liver and heart blockage and should be further assessed in larger studies. Fourth, we did not repair the diaphragmatic incision and observed visceral herniation complications. However, we believe that these complications could be overcome by repairing the diaphragmatic wound with endoscopic clips. Fifth, there are anatomical differences between humans and animals, including the longer distance to the apical lung region from the umbilicus in humans; this problem could be overcome by using longer endoscopic instruments and staplers to facilitate lung resection in tall human subjects. Despite these limitations, the preliminary outcomes demonstrate that transumbilical thoracic exploration and large lung resection can be performed successfully in a canine model. This appears to be a reasonable, novel alternative to simple thoracoscopic procedures and could be used in the resection of bullae in simple spontaneous pneumothorax, open lung biopsy in interstitial lung disease, and resection of peripheral pulmonary neoplasm.
In summary, our study demonstrates that the transumbilical and transdiaphragmatic approach for lung wedge resection is feasible in a canine model. Further studies with a larger sample size should be conducted to evaluate the safety, efficacy, and outcome in an evidence-based evaluation of this surgical procedure before this technique is used in clinical practice in humans.
Footnotes
Disclosure Statement
No competing financial interests exist.