
Abstract
Abstract
Background:
The preemptive intravenous injection of local anesthetics is known to improve postoperative pains in abdominal surgery. The aim of this study is to assess the effect of intravenous lidocaine injection and analyze the precise amount of pain by computerized patient-controlled analgesia (PCA) in patients who had undergone laparoscopy-assisted distal gastrectomy (LADG).
Patients and Methods:
A double-blind placebo control study was designed, and 34 patients undergoing LADG for early gastric cancer were divided into two groups. Preoperatively and throughout the surgery, Group I received intravenous lidocaine injection, and Group C received normal saline injection for placebo. Postoperative outcomes, including the visual analog scale (VAS), the button hit counts (BHC) from PCA, and amount of fentanyl consumed, were measured.
Results:
The demographic data were similar between the groups. The VAS score, BHC, and fentanyl consumption were lower in Group I compared with Group C (P<.05). In particular, fentanyl consumption and BHC in Group I showed a significant decrease during the first 12 hours of the study (P<.05). Postoperative adverse events showed no difference except that nausea was more frequent in the placebo group (P=.039).
Conclusions:
In this study, intravenous lidocaine injection showed a significant reduction in fentanyl consumption and pain during the earlier postoperative time with more favorable outcomes.
Introduction
Lidocaine is safe, economical, and feasible when administered intravenously. A perioperative administration of lidocaine significantly dilutes surgery-induced levels of pro-inflammatory cytokines, which diminishes hyperalgesia and blocks voltage-sensitive sodium channels responsible for the generation of ongoing ectopic activity in the afferent neurons without conduction block.2,5,6 Because the former shows a more dominant action between the two, surgical stress and impact should be grave enough to elicit the pro-inflammatory cytokines. Therefore, the effect of lidocaine differs in various types of surgery, and thus a greater effect is expected in major abdominal surgery.4,7,8
Recently, laparoscopy-assisted distal gastrectomy (LADG) has become one of the most popular minimally invasive surgeries throughout the world in treating early gastric cancer.9,10 Although LADG presents superior postoperative outcomes over conventional gastrectomy, postoperative pain can still occur after LADG. 11
Therefore, we hypothesized that systemic lidocaine benefits postoperative pain. We designed this study to assess the effect of intravenous lidocaine injection and analyze the precise amount of pain by computerized patient-controlled analgesia (PCA) in patients who underwent LADG. The secondary outcome measures were amount of fentanyl consumptions and postoperative adverse events.
Patients and Methods
Patients
The study protocol was approved by the Institutional Review Board from the College of Medicine, Chung-Ang University, Seoul, Korea, and was carried out following the 2000Declaration of Helsinki. Written informed consent was obtained from all participants prior to study inclusion.
In total, 34 patients who required LADG for preoperatively diagnosed early gastric cancer at Chung-Ang University Hospital between March 2011 and December 2011 were eligible for enrollment in the study. Patients with advanced renal and pulmonary disease, heart failure, and hypersensitivity to lidocaine were excluded; those who were required to convert to laparotomies were also excluded. The decision to enroll and exclude patients was made by the principal investigator, who did not otherwise participate in conducting the study and data collection.
Study design and randomization
We created a randomized, double-blind, placebo-controlled study. Randomization into one of the two groups (Group C or Group I) was based on a computer-generated random table. Block randomization was used in order to prevent imbalances in treatment assignments. The details of the series were unknown to the investigators, and the group assignments were kept in sealed envelopes, each bearing only the case number on the outside. After the patient was admitted into the operating room and just before the induction of anesthesia, the numbered envelope was opened, and the card inside determined the group into which the patient would be placed. In order to keep the anesthesiologist “blind” to the patients' assigned group, the patients were given lidocaine or normal saline as placebo, without a label. The preparations of bolus and continuous injections were arranged by an additional investigator who read the card. Patients assigned to Group I received an intravenous bolus injection of 1.5 mg/kg lidocaine followed by a continuous infusion of 2 mg/kg/hour; Group C received the same amount of normal saline injection for placebo.
All parties involved, including the patients, the surgeon, the anesthesiologists, and the investigator collecting the data, were unaware of the study drugs or the patients' group assignment.
General anesthesia
All patients entered the operation room without premedication. Anesthesia was induced intravenously with 5 mg/kg thiopental and 0.6 mg/kg rocuronium. The trachea was intubated, and ventilation was adjusted to keep the end-tidal CO2 between 35 and 40 mm Hg. Anesthesia was maintained using 2–3% sevoflurane in 1.5 L/minute nitrous oxide and 1.5 L/minute O2. The noninvasive arterial blood pressure, electrocardiography, and pulse oximetry were monitored continuously. During surgery, the patients received an intravenous infusion of lactated Ringer's solution at a rate of 5–10 mL/kg/h. No additional analgesics were injected during the surgery.
Surgical technique
All surgical procedures were carried out identically with five trocar techniques. After mobilization of the great omentum, a right-to-left infrapyloric lymphatic dissection was performed. Consecutive sequential lymphadenectomy of the named arteries were carried out, and dissection of the lesser curvature was followed by double ligation of the left gastric artery. Extracorporeal anastomosis was performed using a 4-cm-length transverse incision. The Billroth I anastomosis was formed between the posterior wall of the stomach and the duodenal stump. A Silastic® (Dow Corning, Midland, MI) drain was inserted under the liver along the gastroduodenostomy.
Postoperative pain control
A computerized intravenous PCA system (Automed 3300™; ACE Medical Corp. Ltd., Seoul) was used to control postoperative pain.
The PCA regimen contained 20 μg/kg fentanyl in 100 mL of solution. The PCA system was programmed to administer a basal flow of 1 mL/hour and a PCA level of 1 mL/dose with a lockout interval of 15 minutes. The PCA was prepared by a nurse. The patients were taught to push the button of the PCA system, which delivered a bolus of the drug, each time pain occurred. In the case of persistent pain exceeding a visual analog scale (VAS) pain score of 30 mm, an additional 50 μg of fentanyl was intravenously injected by an investigator until the pain was relieved to a level falling below a VAS pain score of 30 mm.
Studied variables
During the preoperative visit, the patients were instructed in the use of the 100-mm VAS (from 0=“no pain” to 100=“worst pain”) for pain assessment and of the PCA device.
Two investigators who were responsible for data collection during the study were instructed the use of the VAS and PCA device, and a protocol to instruct the use of the VAS and PCA device was standardized.
Age, American Society of Anesthesiologists (ASA) physical status, duration of anesthesia (from injection of thiopental to extubation), and duration of surgery (from skin incision to end of closure) of each patient were determined and recorded.
To measure pain intensity, the VAS pain score was measured at 2, 4, 8, 12, 24, and 48 hours after surgery. The button hit counts (BHC) from PCA and the fentanyl consumption (the sum of additional intravenous fentanyl bolus injections and the fentanyl delivered by the PCA system) were evaluated at similar time points: up to 2 hours, 2–4 hours, 4–8 hours, 8–12 hours, 12–24 hours, and 24–48 hours. Satisfaction scores regarding pain control and with the overall recovery process were obtained at 48 hours (on a numeric rating scale of 11, with 0=“very dissatisfied” and 10=“very satisfied”).
The incidence of postoperative nausea and vomiting was collected from each patient. Furthermore, time values that represented the recovery rate were collected from each patient; these included the time of first regular diet ingestion and the length of hospital stay.
Statistical analysis
The primary outcome variable was the VAS pain score. In order to estimate the group size, a pilot study was conducted with measurements of the VAS pain score at 2 hours after surgery for 8 patients who received normal saline intravenously. The standard deviation of the VAS pain score in this group was 21 mm. For our power calculation, we assumed an equal standard deviation in Group I. We wanted to demonstrate a difference of 20 mm in the VAS pain score at 2 hours after surgery between the groups. With a two-tailed α=0.05 and a power of 80%, we needed 17 patients in each group.
For intergroup comparisons, the distribution of the data was first evaluated for normality using the Kolmogorov–Smirnov test. The normally distributed data were presented as mean±standard deviation values, and the groups were compared by Student's t test. The non-normally distributed data were expressed in medians (interquartile range), and these data were analyzed the Mann-Whitney U test.
Descriptive variables were subjected to chi-squared analysis or Fisher's exact test, as appropriate, and P values of <.05 were regarded as statistically significant. The data in the figures were reported as mean±standard error values. Statistical analysis was conducted using SPSS version 18.0 software (IBM Corp., Armonk, NY).
Results
There were no significant differences between the groups in terms of age, gender, ASA class, height, weight, duration of anesthesia, and surgery (Table 1).
Data are mean±standard deviation values, except for American Society of Anesthesiologists (ASA) grade and gender, which are number of patients.
Kruskal–Wallis test is used, and data are expressed as median (interquartile range) because of abnormal distribution.
F, female; M, male.
One patient in Group I was excluded from this study as LADG was converted to laparotomy because of technical failure of the laparoscopic apparatus. One patient in Group C was excluded as the patient required meperidine because of postoperative shivering. Subsequently, two patients who fulfilled our inclusion criteria replaced this excluded patient.
The results of the VAS pain score are shown in Figure 1. Until the first 24 hours, Group C experienced a significantly higher VAS score compared with Group I, and the tendency of a higher score was observed throughout the study. In both groups, the pain levels were highest during the earliest period of observation and showed a tendency to diminish gradually. However, in the 8th postoperative hour, Group I showed a slight increase over the previous time interval.

Visual analog scale (VAS) score. Data are mean±standard error values. *P<.05.
Group I showed significantly favorable outcomes compared with Group C in terms of fentanyl consumption and BHC during the first 12 postoperative hours (Figs. 2 and 3). The clinical difference among the groups gradually diminished with passage of time. Thus, the total amount of fentanyl consumption and BHC were significantly lower in Group I compared with Group C (Table 2).

Button hit counts for patient-controlled analgesia (PCA). Data are mean±standard error values. *P<.05.
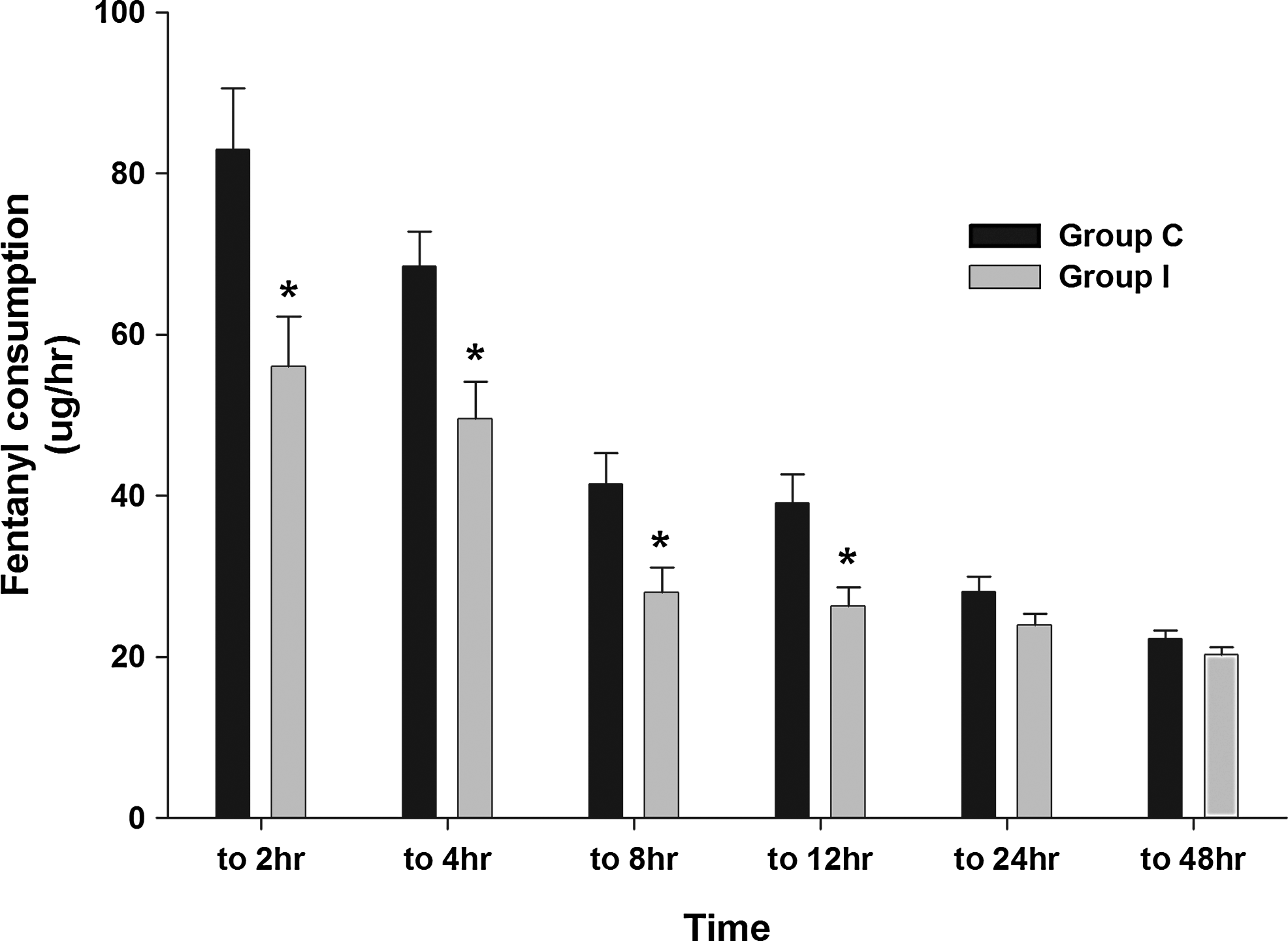
Fentanyl consumption. Data are mean±standard error values. *P<0.05.
Data are mean±standard deviation values or median (interquartile range).
P<.05 compared with Group C.
Mann–Whitney U test is used, and data are expressed as median (interquartile range) because of abnormal distribution.
BHC, button hit counts.
Nausea was less frequent in Group I than in Group C. No significant differences were noted between groups for the satisfaction score, vomiting, hospital stay, and regular diet (Tables 2 and 3).
P<.05 compared with Group C.
HD, hospital days; RD, regular diet start.
Discussion
Until now, lidocaine has exerted effects that cannot be explained by voltage-gated sodium channels. Various explanations for the analgesic activity of systemic lidocaine, including both anti-inflammatory and antinociceptive mechanisms, have been discussed.12–15 Very few investigators, including Werdehausen et al., 13 conducted studies to support the central analgesic activity of lidocaine metabolites by way of inhibition in the glycinergic pathways. 16 According to the study of Werdehausen et al. 13 in the central nervous system, monoethylglycinexylidide, which is the major metabolite of lidocaine, inhibits glycine uptake even in a low serum dose, resulting in extracellular glycine concentrations and demonstrating the principal mechanism of antinociceptive action.
Pain encompasses an immunologic response correlated with the severity of inflammation and is beyond the concept of mere sensitization in peripheral nerve endings by secreting neural mediators. In surgical trauma, the immune system increases levels of pro-inflammatory cytokines, including interleukin-1 and interleukin-6, which induce peripheral and central nervous system sensitizations leading to hyperalgesia. Interleukin-1 induces a long-lasting synthesis and release of substance P from the peripheral nerve terminals of primary afferent neurons, eventually leading to a systemic inflammatory response syndrome, followed by an overcompensated anti-inflammatory cytokine production. Consequently, the patient becomes immunosuppressed and therefore is more vulnerable to opportunistic infections and a spectrum of postoperative adverse events.17,18 Thus, previous studies have indicated lidocaine as a modulator in the reciprocal interaction between pro-inflammatory cytokines and pain sensitivity.14,19,20
Lidocaine is known to suppress lymphocyte proliferation and attenuate production of both pro- and anti-inflammatory cytokines, which influence acute-phase inflammation reactions.21,22 Like all anti-inflammatory agents, lidocaine shares the properties of adherence inhibition of leukocytes—suppressing the movements of leukocytes to migrate from intravascular space into the inflamed tissues, resulting in decreased levels of exudates and postoperative edema.21,23 It is also suggested that lidocaine inhibits phagocytosis and lysosomal enzyme release in the post-phagocytic phase. 24 MacGregor et al. 21 have reported that in terms of leukocyte congregation, the inhibition of inflammation was more than 10-fold greater with lidocaine compared with methylprednisolone.
In experimental studies, laparoscopic surgery has demonstrated a reduced impairment of the delayed-type hypersensitivity response compared with conventional surgery.25,26 Accumulative clinical data have also supported that a reduction of surgical trauma using a minimally invasive approach restores immunity and spares inflammatory cytokines.27,28 However in a recent randomized controlled trial, laparoscopic procedures were reported to cause more intense pain during the immediate postoperative period, and even the most minimally invasive procedures are not pain free.29,30
The consensus among the different attempts performed in various types of operations is that preemptive analgesics are most effective in major abdominal surgeries accompanying extensive tissue trauma and pronounced postoperative pain.7,31,32 Therefore, the current study was focused on evaluating the preemptive analgesic effect of perioperative intravenous lidocaine injection in laparoscopic gastrectomy patients. Corresponding to the hypothesis that a lidocaine injection attenuates postoperative pain and decreases the supplement of opioid analgesic more than placebo, Group I showed superior outcomes in all measured variables.
The favorable effects of lidocaine were diminished with the passage of time between the groups, thus indicating that lidocaine benefits most in the immediate postoperative period. It is known that the benefits of lidocaine are influenced by its elimination half-life (90–120 minutes). This phenomenon raises the issue of whether the limited intraoperative period of lidocaine administration may have affected its potential benefits. New study models are needed to compare the effects of additional continuous lidocaine injections in the postoperative period with perioperative injections and to correlate serum lidocaine concentrations with clinical presentations.
In our study, there were no significant demographic differences between the groups. Nausea was more frequent in the control group compared with the injection group. This is best explained by an increased opioid consumption in the control groups inducing nausea, which indirectly reflects the effect of uncontrolled increased levels of pro-inflammatory cytokines in the control group.
Besides adverse cardiac effects, lidocaine may have undesirable effects on neurologic functions as it interrupts nerve conduction by way of blocking the sodium channels. Proportional to its plasma levels, systemic lidocaine produces central nervous effects, such as paranoid ideation, agitation with hallucinations, dizziness, and light headiness at high concentrations (>5 μg/mL.33–35 However, in our study, no neuropsychiatric events were observed throughout the process.
A limitation of our study is that data on the first flatus could not be compared in this series, as it was difficult to obtain objective patient records. As hospitalization costs for cancer patients in Korea are mostly tendered by the government insurance system, patients were reluctant and unsafe to be discharged earlier. When we applied the same clinical path for each patient, postoperative courses were similar between the study groups. Therefore, although the injection group showed a tendency for an earlier discharge, the delineation for shorter hospital stays remains uncertain. However, as lidocaine injection have yielded earlier bowel recovery and reduced pain in previous studies, an earlier soft diet intake and shorter hospital stay is expected in the future.2,4
Lidocaine injection is economical, easy to access, feasible, and safe when administered in appropriate dosages. We have demonstrated that a preemptive administration of intravenous lidocaine injection is safe and delivers a clear benefit of perioperative outcomes in laparoscopic gastrectomy.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology (grant 2012R1A1A1003700).
Disclosure Statement
No competing financial interests exist.