
Abstract
Abstract
Background:
Surgical management of the lower end of the ureter during laparoscopic nephroureterectomy remains a matter of debate. The commonest method during laparoscopic nephroureterectomy—endoscopic incision—has been shown to have a higher recurrence rate compared with open surgical excision with a cuff of bladder. In addition, the literature still lacks comparative studies between different approaches to support and guide the current clinical practice.
Patients and Methods:
Three consecutive series of patients undergoing laparoscopic radical nephrectomy for transitional cell carcinoma located in the lower one-third of the ureter with different methods (laparoscopic en bloc resection of ureter with a cuff of bladder, open surgical excision, and endoscopic incision) of dealing with the lower end were compared in their short-term surgical and oncological outcomes. The primary outcome was recurrence at 12 months of follow-up. The secondary outcomes were hospital stay, positive surgical margins, and duration of catheterization.
Results:
Analysis of perioperative and postoperative outcomes revealed laparoscopic en bloc resection of the lower end of the ureter with a cuff of bladder is a safe and feasible approach with the advantages of the laparoscopic approach such as less hospital stay compared with the open approach. The analysis of oncological outcomes in this feasibility study showed a higher rate of recurrences in the endoscopic approach.
Conclusions:
Laparoscopic en bloc resection of the lower end of the ureter with a cuff of bladder during nephroureterectomy for tumors located in the lower one-third of ureters is safe and feasible in terms of perioperative outcomes and early oncological results. We acknowledge that the small sample size and the nonrandomized design are a limit of the study. Thus, prospective randomized controlled trials are recommended to prove the superiority of one approach over the others.
Introduction
Laparoscopic resection of upper tract transitional cell carcinoma is an established surgical procedure with well-known perioperative advantages compared with open surgical excision. 5 Various techniques are used during the procedure to remove the distal ureter 6 : most commonly endoscopic resection or cold knife incision or alternatively by an open surgical approach. Often studies7,8 exclude patients with tumors in the distal third of the ureter from having minimally invasive or laparoscopic approaches; thus the benefits of ever-expanding laparoscopic techniques remain unknown in this group. 9
We describe a technique of laparoscopic en bloc resection of the lower ureter with a cuff of bladder without placement of any additional ports during nephroureterectomy. The aim of this report was to assess the feasibility, safety, and early oncological outcomes of the new technique compared with open surgical excision or the endoscopic approach.
Patients and Methods
Six men with lower ureteric tumors (defined as location of the tumor lower than the pelvic brim on computed tomography urograms) with a mean age of 73.4 years (standard deviation 6.4 years) were recruited into the study (Table 1). Patients with a body mass index of more than 40 kg/m2, previous bladder tumors, multifocal disease, bilateral tumors, and previous pelvic radiotherapy or surgery were excluded from the study. All the participants had flexible cystoscopy to rule out the presence of bladder tumors.
F, female; M, male.
Surgical technique
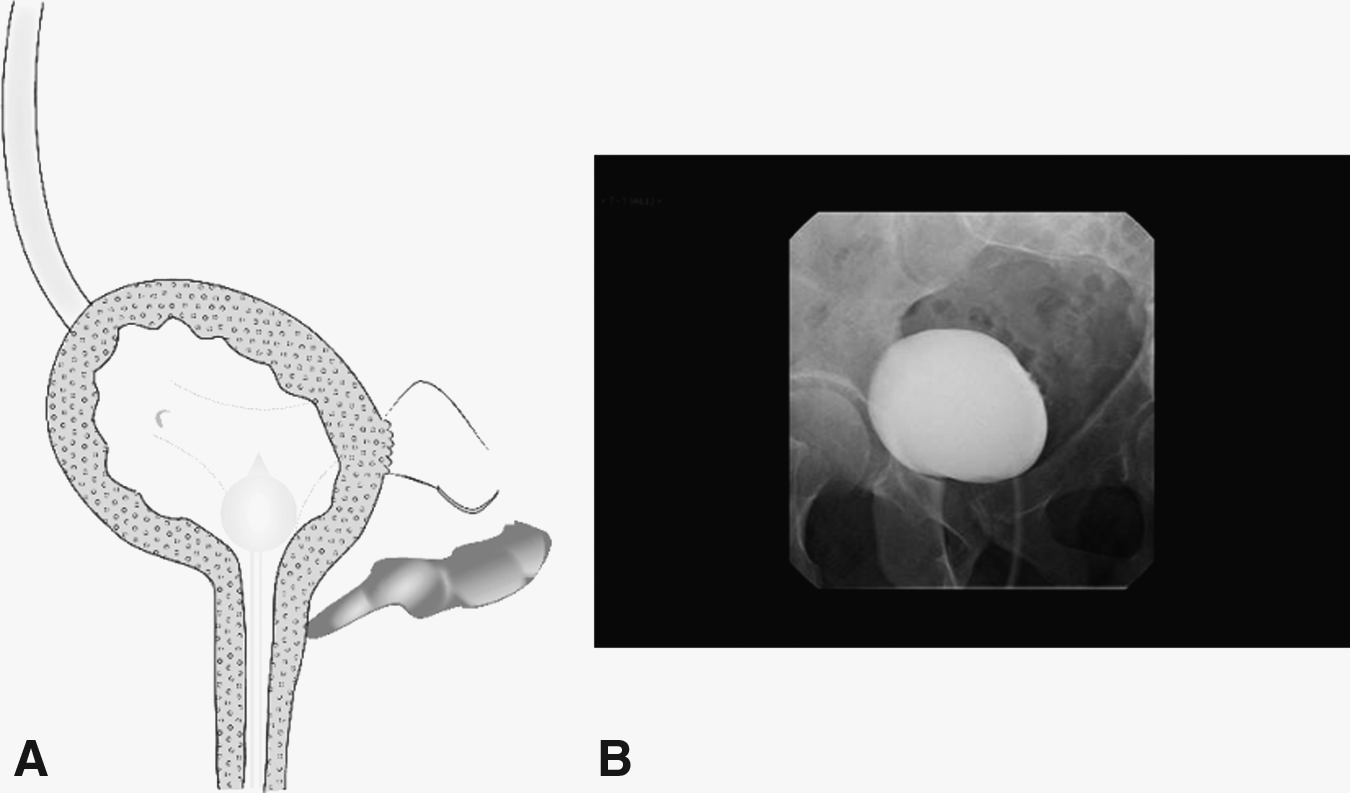
Instrumentation and preparation are exactly the same as requirements for transperitoneal laparoscopic nephroureterectomy. The patient is positioned in the usual nephrectomy position under general anesthesia with 20–30° side tilt to expose space among the ipsilateral external iliac spine, umbilicus, and symphysis pubis. The specific surgical instruments required are shown in Table 2. Laparoscopic radical nephrectomy is commenced with a transperitoneal approach with ports positioned as shown in Figure 1. Note the distance and the angle between the lower lateral and main endoscopic ports. The angle between the two lower ports should not be more than 20° as a higher angle causes difficulty in intracorporeal urinary bladder suturing. Laparoscopic removal of the kidney is carried out in a standard stepwise approach. 5 After the kidney is excised, the ureter is traced toward the pelvis, the position of the optics is changed, and the optics are used through the upper port. The ureter is traced to the iliac vessels and toward the pelvis in a plane as shown in Figure 2. A clip is placed just distal to the visible bulge in the ureter to prevent any spillage of cancer cells into the urinary bladder during manipulation of the ureter. The ipsilateral vas deferens is identified and traced to the seminal vesicles, which act as a landmark for the lower limit of the ureteric opening into the bladder (Fig. 3). The urinary bladder is filled with 300–350 mL of normal saline at this stage. A cuff of bladder is excised; note the tip of the vesicle in vision. The defect left (Fig. 4) is sutured using two layers of interrupted sutures. The nephroureterectomy specimen along with the cuff of bladder is removed through the 12-mm port in an endocatch bag. The catheter is left for 10–14 days and removed after a satisfactory cystogram (Fig. 5). None of the patients received any adjuvant intravesical treatment.
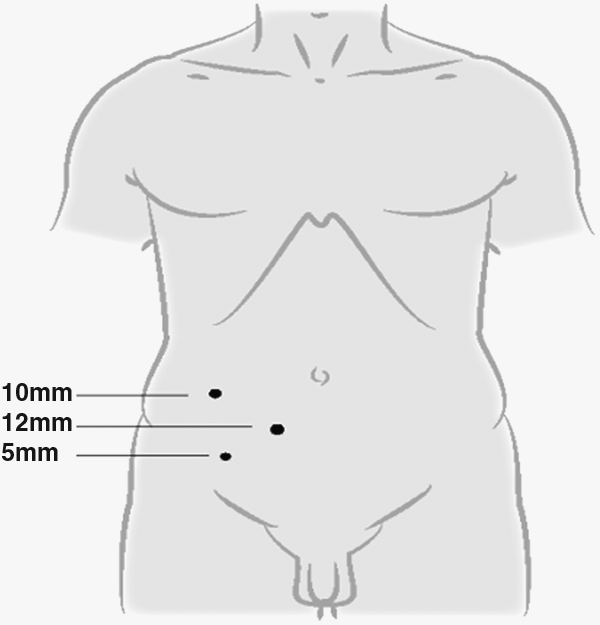
Position of trocar placement. Note the angle between the lower two trocars. This angle makes it easier to carry out subsequent intracorporeal suturing.
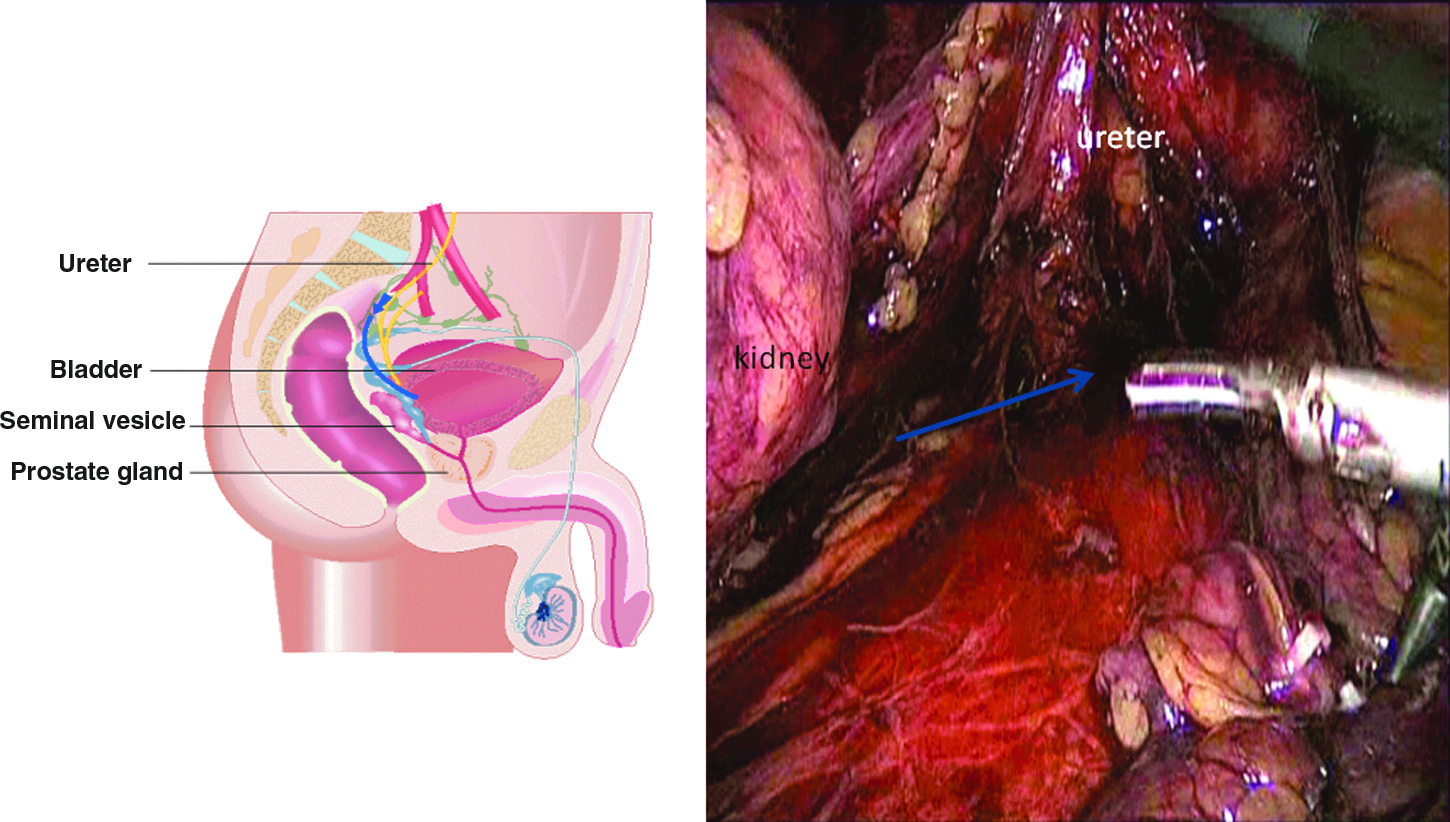
After removal of the kidney, the ureter is traced back to the opening into the urinary bladder. Note the plane of dissection (blue line and arrow) between the ureter and the seminal vesicles.
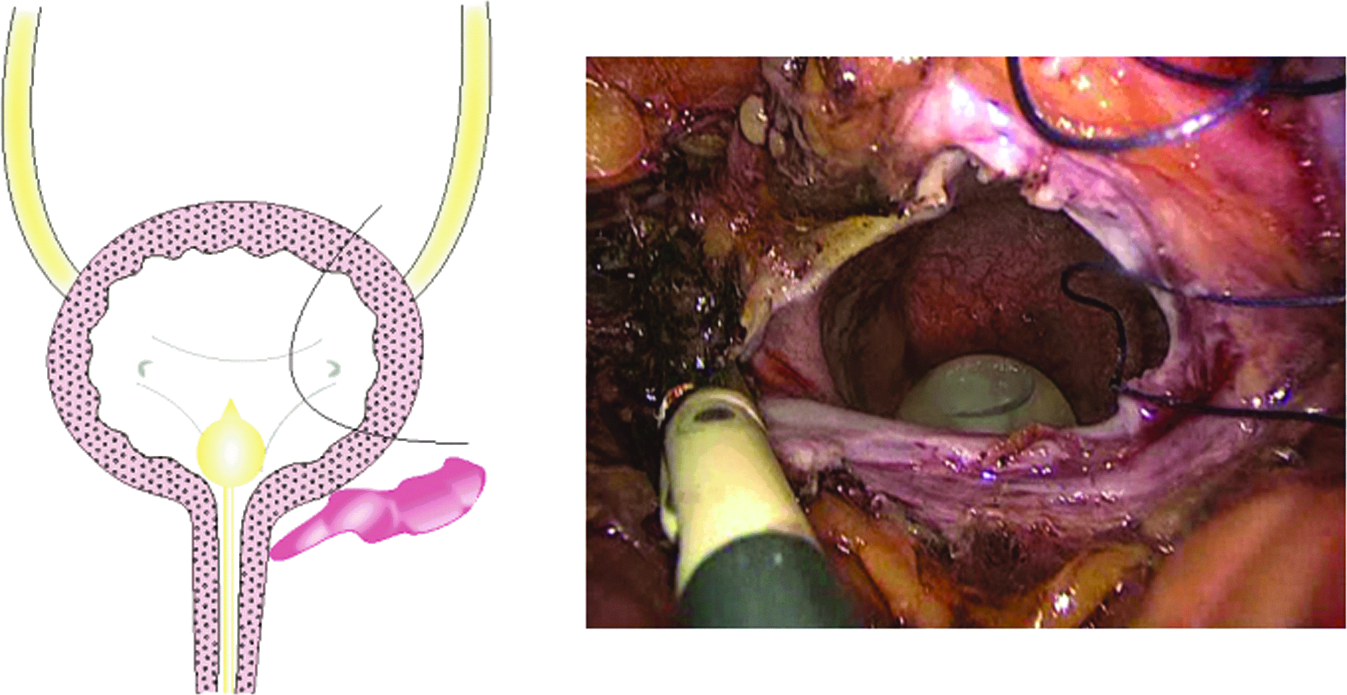
A cuff of bladder along with the ipsilateral ureteric orifice is being removed. It should be ensured that the other ureteric orifice is visualized while making an incision into the trigonal area.
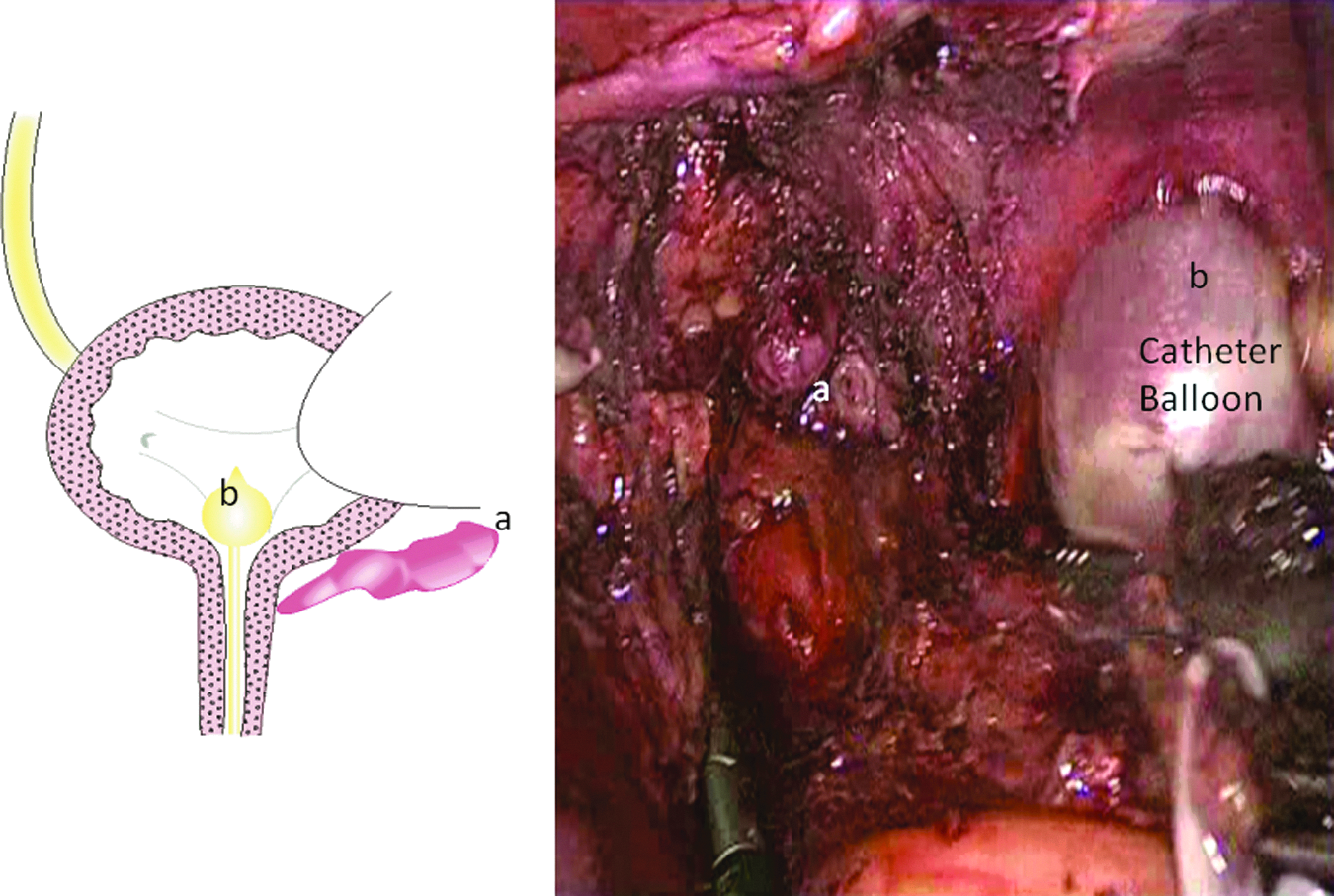
A large defect seen with a catheter balloon (b) in the bladder. Note the tip of the seminal vesicle (a).
The laparoscopic technique described here recreates the steps of open trans- and extravesical approaches in dealing with the distal ureter without in principle compromising the oncological safety, especially for lesions in the distal third of the ureter.
Our preliminary data from 6 patients suggested a good recovery and no postoperative complications. Drains were removed within 48–72 hours of the surgery, and cystograms at 10–14 days of procedures showed no leakage in any of the patients. Our observation suggested that this is a viable technique in the hands of experienced laparoscopic surgeons with good intracorporeal suturing skills.
Selection of comparative group
For each of the 6 men in the study, 2 control participants were chosen from a total of 128 nephroureterctomy procedures carried out at the same institute with open or endoscopic management of the distal ureter. The matching process was based on eight features: age, sex, body mass index, tumor location, no concurrent or previous bladder tumor, transperitoneal laparoscopic resection of kidney, and laparoscopic nephroureterectomy carried out within 5 years of the study. Complete follow-up was recorded.
All patients in the matched-paired analyses had laparoscopic nephroureterectomy procedure with different strategies for handling the lower end of the ureter. The open technique involved a midline or Pfannensteil incisions with transvesical excision of the lower end of the ureters and removal of the specimen. The endoscopic approach consisted of endoscopic incision of the lower end and then plucking of the ureter after completing the nephroureterectomy. The specimens were extracted intact by enlarging the lower port in a bag.
During matched-pair analysis, each pair was classified by the pattern of outcome events experienced within the pair. Pairs are classified as concordant if the events are same and as discordant if an event was experienced by one of the members in the pair.
Results
The matched characteristics of the three groups are summarized in Table 3. The patients were matched by sex, age, body mass index, and stage and grade of cancers. There are no significant differences in the demographics between the groups due to the inherent design of the study methodology.
SD, standard deviation.
In the endoscopic management group, 1 patient had positive surgical margins (ureteric), and 2 patients had bladder recurrence within 3 months as seen on white light cystoscopy. Compared with the other two techniques, 1 patient in the open surgical excision group had bladder recurrence identified by cystoscopy at 6 months post-surgery. With follow-up ranging from 12 months to 66 months, there was statistically significant concordance between the open and en bloc laparoscopic excisions, whereas three discordances were observed between the endoscopic and en bloc laparoscopic approaches. No statistical significance differences were seen between endoscopic and en bloc excision (relative risk 1.0497; 95% confidence interval 0.79–1.394; P=.738) in the risk of positive surgical margins. Similarly, no differences were seen at 12 months in cystoscopic recurrences between the groups (relative risk 1.1497; 95% confidence interval 0.82–1.608; P=.415).
None of the patients treated by the new technique had any postoperative complications or urinary leakage on cystograms carried out between postoperative Days 10 and 14. Hospital stay was significantly lower than that in the open surgical repair (almost 50% reduction). There were no significant differences in blood loss, operative time, and postoperative complications.
Discussion
The laparoscopic technique described here imitates open trans- and extravesical approaches in dealing with the distal ureter without compromising the early oncological safety. Our preliminary data in 6 patients suggest a good recovery and no postoperative complications. Our observations suggest that this is a viable technique in the hands of experienced laparoscopic surgeons with good intracorporeal suturing skills.
The aim of the present study was to assess feasibility and safety of the technique compared with the established surgical practice. Although this needs to be further assessed in a larger cohort of patients and including long-term oncological outcomes, our preliminary observation with 12 months of follow-up clearly points toward its viability as an alternative option.
Two previous studies have reported the feasibility of pure laparoscopic excision of the ureter in patients with upper tract transitional cell carcinoma; however, in one study, 7 distal tumors were excluded, and the other study had just 1 patient with a distal ureteric tumor. 8 Clearly, the reported literature suggests that distal ureteric tumors are not favored for the laparoscopic approach and hence underscores the importance of the technique described in this article.
A myriad of techniques have been described to deal with the distal ureter.3,7,10–13 Most of these techniques have reported the feasibility and safety of the procedures; however, long-term data reporting oncological outcomes are lacking. Endoscopic approaches ranging from resection to incisions sometimes combined with careful coagulation of the ureteric end, followed by “pluck” during laparoscopic radical nephroureterectomy, are popular with urologists during laparoscopic resection of upper tract transitional cell carcinoma. The seeding of tumor cells during laparoscopic mobilization of kidneys or ureters remains a concern. 14 Higher recurrences in the urinary bladder on follow-up cystoscopic surveillance were noted by many in the past. 4 This may be one of the main reasons few studies are not in favor of recommending endoscopic management in patients with tumors in the distal third of the ureter. 3 Similarly, the extravesical stapling technique carries a higher risk of recurrences.
The quality of the literature in this area remains poorly reported, retrospective in nature, and often limited to case series by a single surgeon. 4 Our feasibility study points toward safety of the procedure; however, long-term oncological safety needs to be tested for this procedure. Future protocol-driven prospective studies, preferably with randomized design, are needed to settle the question of the best surgical approach to the distal ureter during radical nephroureterectomy, specifically for tumors in the distal third of the ureter.
Footnotes
Disclosure Statement
No competing financial interests exist.