
Abstract
Abstract
Introduction:
The aim of this study is to present a preliminary series of six children affected by an anterior mediastinal mass, resulting in a thymoma. We treated this pediatric population by a video-assisted thoracoscopic thymectomy.
Patients and Methods:
We performed a retrospective study from January 2000 to January 2012 of all children affected by an anterior mediastinal mass, resulting in a thymoma. Data included sex, age at surgery, clinical and radiological features, surgical procedure, follow-up, and complications.
Results:
Video-assisted thoracoscopic thymectomy was performed in six children (five boys and one girl). Four patients presented with dyspnea and/or thoracic pain treated with analgesic and corticosteroid therapy without any benefits. Two patients were asymptomatic. Preoperatively, exams included radiological imaging, blood, and immunological test. All 6 patients were treated with a thoracoscopic approach; of these patients, 5 were treated with a thoracoscopic right-side thymectomy and 1 with a left-side approach. Patients were treated by a three-trocar technique, and thymectomy was performed using Valleylab (now Covidien) (Boulder, CO) LigaSure™. The mean operative time was 120 minutes. The mean hospital stay was 5 days. In all cases histological findings revealed no malignancy. The mean follow-up was 38 months.
Discussion:
Thoracoscopic thymectomy facilitated the goal of early thymectomy. The right-side approach is preferred because it gains a good visualization of the venous anatomy for dissection. The left side allows a good extended resection of both the thymus and perithymic fat. Thoracoscopic thymectomy should be consider a valid, less invasive alternative to the most radical open approach.
Introduction
Patients and Methods
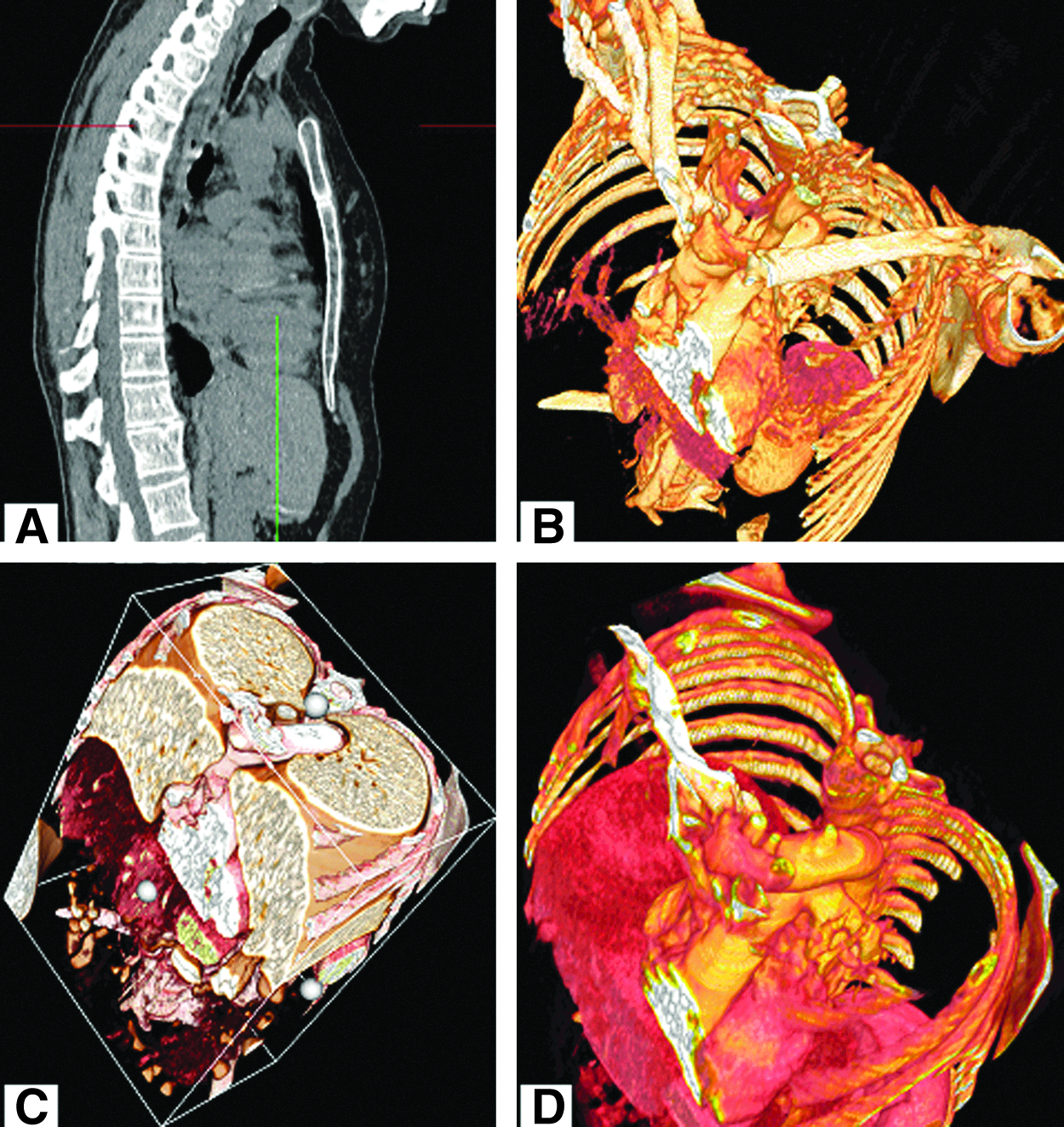
Between January 2000 and January 2012, 18 patients presented with anterior mediastinal mass; 6 of these patients (5 boys and 1 girl), with a median age of 8 years (range, 6–11 years), underwent complete thoracoscopic thymectomy for diagnosis of Masaoka stage I and II thymoma without myasthenia gravis (Table 1). All patients were subjected to diagnostic procedures that included chest radiograph, thoracic computed tomography, or magnetic resonance imaging with a virtual reconstruction by virtual rendering (Fig. 1), assessment of pulmonary function, and complete neurologic workup. In each case, the anterior mediastinal mass demonstrated features highly suggestive of thymoma without signs of invasion to the surrounding structures and diameter <5 cm. Two patients were asymptomatic, whereas in 4 cases there were respiratory symptoms (dyspnea, chronic coughing, thoracic pain, fatigue, and weight loss). Surgical resection was performed in all these cases by a thoracoscopic access.
CT, computed tomography; MRI, magnetic resonance imaging; WHO, World Health Organization.
Surgical technique
The technique was performed in five children from the right side with the patient in the 30° left lateral decubitis position under single right lung ventilation; in the remaining child, in whom preoperative magnetic resonance imaging showed enlargement of the thymic gland to the left side, a left-sided approach was chosen. Three trocars of 5 mm were placed at the fifth intercostal space of the left anterior axillary line for introduction of a 30° telescope and at the third and seventh intercostal space of the midaxillary for instruments. After general exploration, the dissection by LigaSure™ (Valleylab [now Coviden], Boulder, CO) was begun caudally along the capsule of the thymus gland with progressive exposure of the lower pole. Lateral dissection included pericardial tissue and perithymic fat, preserving the phrenic nerve and proceeding toward the innominate vein. The thymic horn was dissected to the point where it ends above the brachiocephalic vein, before one or two thymic veins were closed. At the end of dissection, we removed a 5-mm trocar and inserted a 10-mm trocar, and then the thymic gland was brought into an endobag positioned through the 10-mm trocar. After control of hemostasis, a drainage tube was placed in the seventh intercostal space, in order to promptly remove the pneumoperitoneum after the surgical procedure.
Results
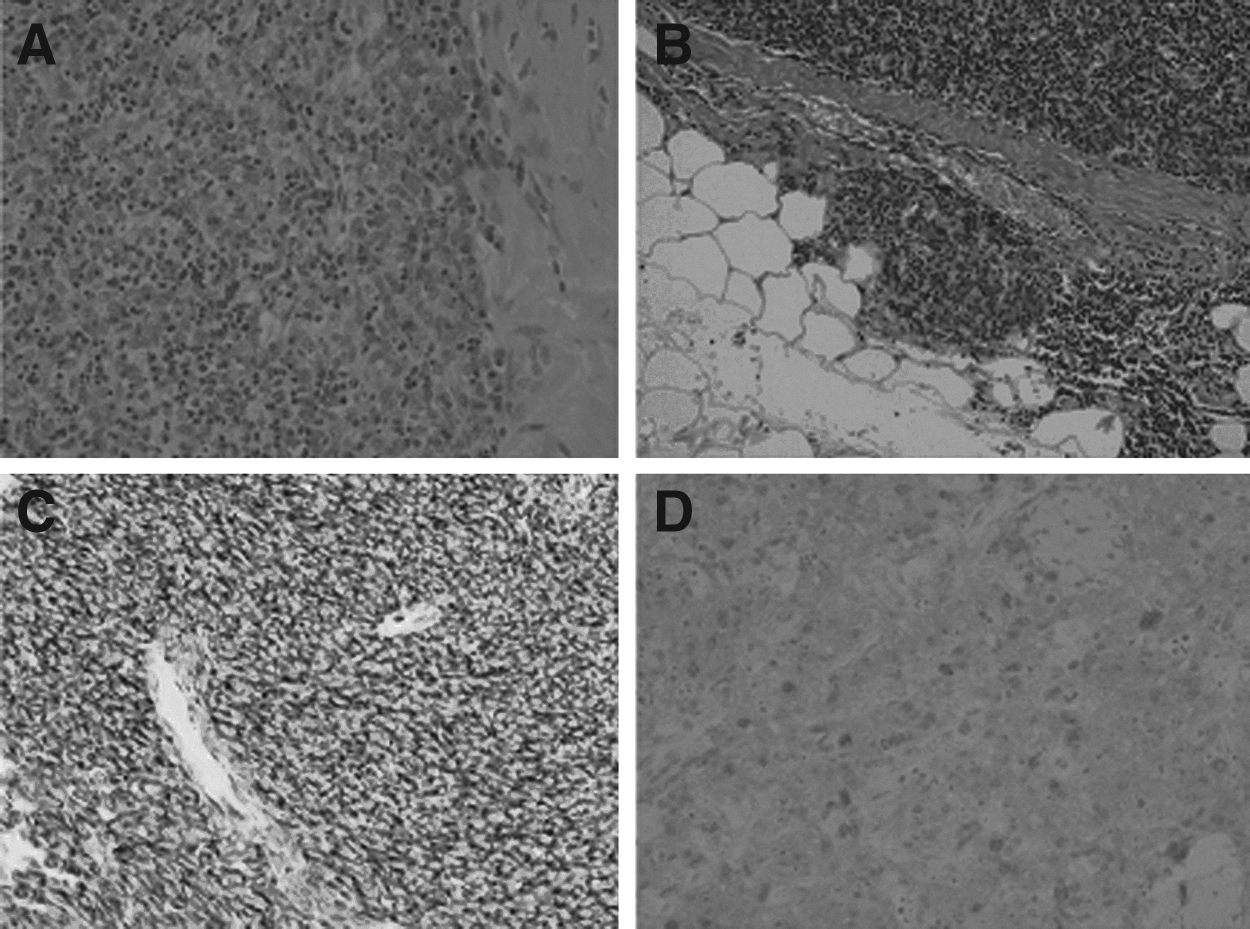
The procedure was well tolerated, with a mean operation time of 120 minutes and without complication, except for minimal bleeding that promptly solved. Oral feeding was restored on the first postoperative day, and the drainage tube was removed in the second postoperative day. The patients made an excellent recovery, with a median time of 5 days, and were discharged after a negative radiological control. Histopathological examination showed in all cases the presence of a well-differentiated thymoma; two cases were classified as World Health Organization AB thymoma, and four were classified as A thymoma (Fig. 2). Only 1 patient presented dysphagia and gastric pain, 10 months after surgery, that resolved after a short treatment with antacids. The mean follow-up was 38 months, and the patients were totally asymptomatic during daily activities with a good cosmetic result.
Discussion
Thymoma is rare in childhood, with only 40 cases reported in the literature. 5 In our study the median age was 8 years, with no child under 1 year of age. The literature reports only 40 cases of thymoma in infants. As others authors have reported, we detected a male predominance in our series (5 males and 1 female). This male predominance needs an explanation with further epidemiological experience. 6 Although most of the thymomas have been reported to be asymptomatic in the literature, 4 cases in our study were symptomatic, showing dyspnea with chronic coughing, a stabbing chest pain during exercise, and weight loss. A chest computed tomography scan and magnetic resonance imaging were performed preoperatively that showed signs of compression of the trachea and major vessels with irregular mass margins. There were no cystic components in the mass in any case. No case showed any clinical and radiological invasive features. In accordance with the Masaoka staging system, our cases have been considered to be a locoregional tumor corresponding to stages I and II; capsular invasion of the tumor with involvement of the surrounding fat tissue was evident in only 2 of our cases. So, excluding any invasion of adjacent organs and regional or distant metastasis, we did not use any adjuvant chemotherapy or radiotherapy in our series.
In the literature fundamental histological and immunohistochemical studies are considered not only for allowing the diagnosis of thymoma and its staging but also for excluding other epithelial or mesenchymal tumors of the mediastinum, head, and neck region. 7 In accordance with the World Health Organization criteria, two of our cases had a mixed population of cells classified as type AB, and in the remaining cases a monomorphous population of oval-spindle cells was classified as type A. In Masaoka stage I and II cases, the main treatment is surgery, and survival is almost 100% in totally resected cases. 8
Several surgical approaches to thymectomy exist. Total thymectomy by median sternotomy has been the preferred standard treatment for thymoma for a long time, but the operative procedure for thymoma should be reconsidered. The thoracoscopic approach was first reported by Sugarbaker 9 from Boston, MA, and also by the group from Belgium 10 in 1993. Since then, it has evolved with several variants, including video-assisted thoracic surgery of unilateral thymectomy through three ports, the bilateral thoracoscopic approach combined with a cervical incision for extended thymectomy, and more recently endoscopic robot-assisted thymectomy. Minimally invasive techniques have become popular because of their low procedural mortality and morbidity associated with minimal surgical trauma with the best cosmetic results. Ng et al. 11 first proposed a right-sided approach for video-assisted thoracic surgery thymectomy, justifying this for the greater maneuverability of instruments in the wider right pleural cavity and easier identification of the left innominate vein using the superior vena cava as a landmark. Mineo et al. 12 advocated a left-sided approach because the dissection maneuvers are safer for the position of the superior vena cava out of the surgical field with less risk of accidental injury. In addition, the resection of perithymic fatty tissue around the left pericardiophrenic angle and aortopulmonary window can be performed more readily from the left side.
In our follow-up (median time, 38 months) there was no recurrence of thymoma. No case was converted in open surgery, and no case required blood transfusion. In addition, we noted a short hospital stay (median time, 5 days).
There is no agreement on the appropriate size of the thymoma required to permit thoracoscopic surgery. Most authors restrict the indication of thoracoscopic surgery to lesions smaller than those in our series (size <5 cm). Our preliminary results in this series, even if the number of cases is limited, suggest that thoracoscopic thymectomy for low stages of thymoma is technically feasible and safe with an excellent prognosis. Video-assisted thoracoscopic thymectomy is a successful technique in experienced hands and represents an increasingly popular alternative approach to conventional open techniques because it allows achieving the goal of early thymectomy with the advantages of a less invasive procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.