
Abstract
Abstract
Objective and Study Design:
To assess the feasibility of robotic-assisted skull base surgery, a preclincal cadaver study was conducted.
Materials and Methods:
The feasibility study was subdivided into three phases: Phase 1 (surgical corridor) entailed a review of the surgical access, Phase 2 (instrument configuration) entailed arrangements of the robotic instrument (da Vinci® Surgical System; Intuitive Surgical, Sunnyvale, CA) in relation to the surgical corridor and applied to a skull model, and Phase 3 was robotic-assisted skull base cadaver dissection.
Results:
Regarding the surgical corridor, the infratemporal area was accessed through a maxillary window, whereas the anterior skull base region was accessed through a combined single maxillary window and nasal corridor. Regarding instrument configuration, the camera was positioned above the two instrument arms, with both instrument arms angled at 30° to the camera axis with a flexed distal tip for the infratemporal skull base. For the anterior skull base, one of the robotic arms was inserted through the unilateral maxillary window, whereas the three-dimensional camera and the second arm were inserted through the nasal corridor. Regarding the robotic-assisted skull base cadaver dissection, we define the robotic set-up time in this study as the time required to move the robot into position, obtain adequate operative exposure, and place the robotic arms prior to the start of robotic dissection. The robotic set-up time for the anterior skull base dissection averaged 95 minutes, and that for pituitary resection was 61 minutes. The robotic set-up time for infratemporal dissection averaged 23 minutes. Operative time was 63.5 minutes. Robotic and endoscopic techniques can be combined during surgery.
Conclusions:
Robotic-assisted skull base surgery is feasible. The da Vinci instrument needs to be redesigned to be smaller and preferably with distal articulating tips, prior to clinical application of robotics to skull base surgery.
Introduction
In spite of the advances and tremendous advantages, current manual endoscopic surgical approaches to the skull base have several limitations such as the lack of depth perception, two-dimensional imaging, and rigid instrumentation that exaggerate fine movements. The classic open approach to the skull base remains the technique of choice in complex tumors because of the wide exposure and offering a close approach to the target lesions for delicate dissection. The morbidity associated with classic open approaches to the infratemporal fossa and midline anterior cranial base, which require wide disarticulation and disruption of normal tissue, makes them less ideal. Robotic systems address some of the limitations of the traditional open and manual endoscopic skull base approaches by offering three-dimensional (3-D) viewing, tremor filtration, and articulating distal arms that mimic natural hand and wrist movements. In this study, we studied the feasibility of robotic-assisted skull base surgery of the infratemporal fossa and anterior cranial base that combines the advantages of open and endoscopic skull base techniques.
Materials and Methods
Phase 1: surgical corridor
The transnasal and transmaxillary surgical corridors for open and endoscopic approaches to the anterior skull base and infratemporal fossa were reviewed to determine which surgical access could be adapted to accommodate the different arms and 3-D endoscopic camera of the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) for dissection to target lesions.
Phase 2: instrument configuration
A skull model was used to study access and instrument configuration to the infratemporal and anterior skull base areas.
To access target lesions in the infratemporal fossa, we studied different instrument configurations to determine which arrangement could be inserted and easily manipulated through a maxillary osteoplastic windows.
The da Vinci 3-D camera was positioned 2–3 cm from the maxillary osteoplastic window with full magnification setting. For the robotic infratemporal fossa surgery, the 3-D camera and instrument configurations were examined. The first instrument configuration (C1) has both instrument arms on each side of the 3-D camera. The second instrument configuration (C2) has the camera on top of both instrument arms with the distal articulating tips unflexed. In the third instrument configuration (C3), the camera was positioned above the two instrument arms, with both instrument arms angled at 30° to the camera axis and a flexed distal articulating tip (Figs. 1 and 2).
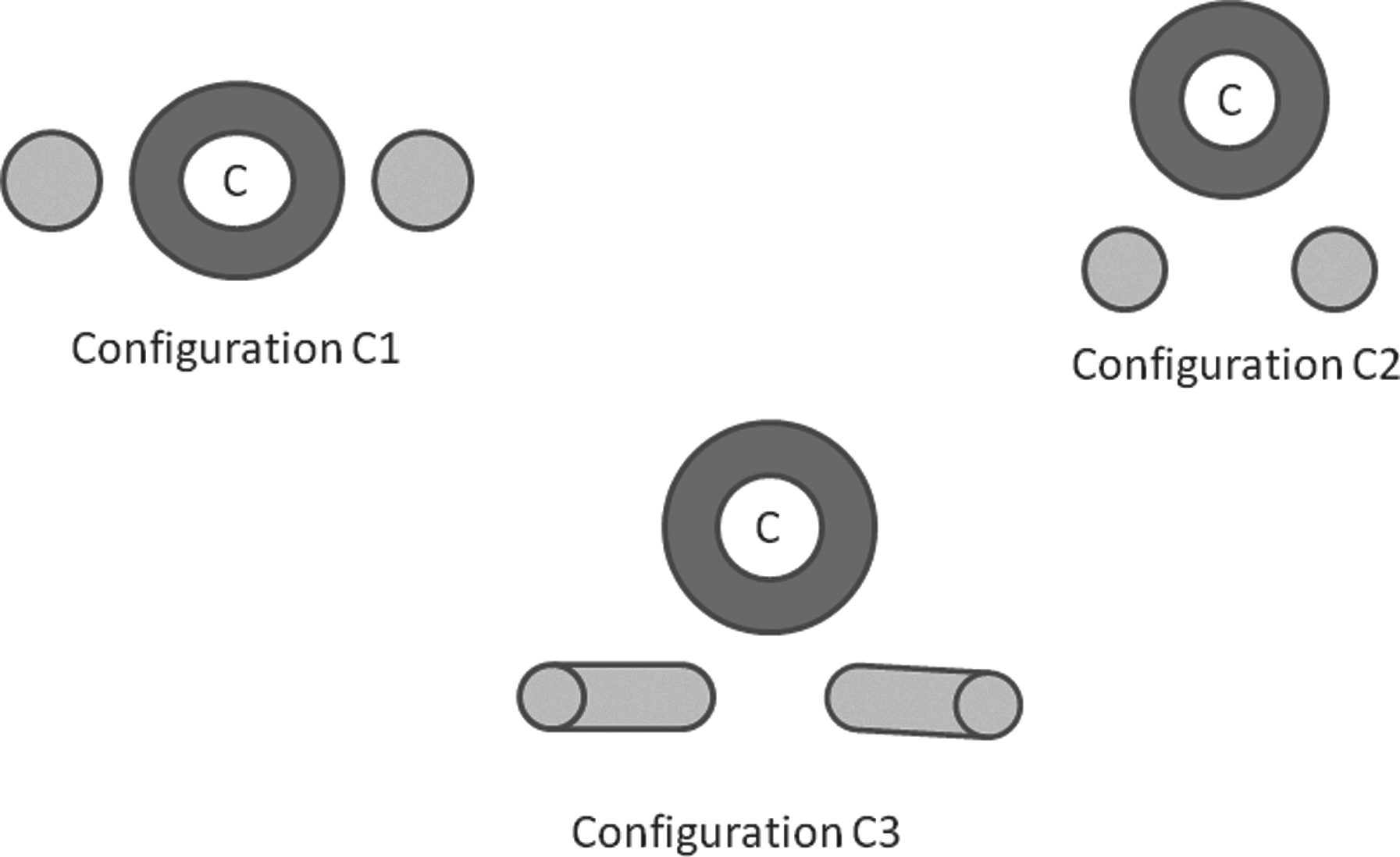
Instrument configuration for robotic infratemporal surgery through the maxillary osteoplastic opening. Robotic instruments are shown in yellow. c, camera.

Robotic arm configuration:
To access targets along the anterior skull base region, one of the robotic arms was inserted through the maxillary osteoplastic window, whereas the 3-D camera and the second arm were inserted through the nasal corridor via the nostril (Fig. 2).
These configurations were first applied to a skull model and were tested at tremor filtration of 1.5:1 (1.5 cm of hand movement results in 1 cm of movement of the arms), 2:1, and 3:1.
Phase 3: robotic-assisted skull base cadaver dissection
The findings from Phases 1 and 2 were then applied to cadaver specimens. Two cadaver heads with intact arterial and venous systems were obtained with institutional review board and institutional approval. The arterial and venous systems were injected with colored latex (red, artery; blue, vein) to visualize the arterial and venous systems. Both the right and left skull base regions of the cadaver were dissected. One cadaver head had one side dissected for the anterior skull base and the opposite side for the infratemporal area via the maxillary osteplastic window. A computed tomography scan of the cadaver heads was obtained prior to the robotic surgery and used for surgical navigation. We marked the end of the infratemporal fossa dissection when the following structures were identified and dissected: maxillary artery, middle meningeal artery, maxillary V2 and V3, lateral pterygoid, foramen rotundum, and foramen ovale.1,2 The end of the anterior skull base dissection was marked when the structures around the pituitary gland were identified and pituitary resection was complete.
Robotic set-up time, operative time, ability to transition from robotic-assisted to manual endoscopic surgical techniques, exposure problems, technical problems, and ability to expose the lateral and anterior skull base regions were reviewed. We define the robotic set-up time in this study as the time required to move the robot into position, obtain adequate operative exposure, and place the robotic arms prior to the start of the robotic dissection. Observations with regard to robotic-assisted endoscopic suturing were noted.
Results
Phase 1: surgical corridor
On review of the different open and endoscopic approaches and preclinical robotic studies, we found that the midface degloving approach with the transmaxillary window could fulfill the surgical access for the infratemporal area,1–3 whereas the modified traditional nasal corridor with one transmaxillary window could be used to access the central skull base region. 4
Phase 2: instrument configuration
All three instrument configurations for the infratemporal dissection were able to provide adequate visualization within the infratemporal region. There were more instrument collisions with the C1 and C2 configurations compared with the C3 configuration. The maxillary osteoplastic window provided an adequate corridor for positioning and manipulation of the 3-D camera and the two instruments for the infratemporal fossa dissection. The C3 instrument configuration was more facile and produced fewer collisions compared with the other instrument set-ups in the infratemporal region.
Access to the anterior skull base was achieved using the nasal corridor and a unilateral osteoplastic window with the instrument configuration of one robotic arm through the osteoplastic window, whereas the other robotic arm and the 3-D camera were passed through the nasal corridor.
There were gross instrument collisions if the da Vinci motion scaling was at 1.5:1. This was more prevalent in the anterior skull base area. Motion scaling at 2:1 was generally ideal, and 3:1 motion scaling was even better for fine and slow movements. Proper positioning of the skull model facilitated a direct trajectory to the target area and lessened the instrument collisions in a given configuration.
Phase 3: robotic-assisted skull base cadaver dissection
Figures 3 and 4 show the operating room set-up for the robotic-assisted skull base surgery. The da Vinci unit was positioned above the patient's head. The Medtronic (Minneapolis, MN) AxIEM™ emitter was positioned in the superior lateral side of the head (Fig. 3). Accurate sterotactic navigation points were obtained. The Medtronic navigational unit was interfaced with the Tilpro of the da Vinci Si, thus giving the surgeon the ability to verify his or her surgical position when the second assistant places the probe.

Operating room set-up. S1, surgeon; S2, assisting surgeon; A, anesthesiologist.

Robotic skull base surgery on
Transmaxillary corridor
To expose the anterior maxillary wall, a sublabial incision was performed extending from the central incisor to the third molar tooth. The soft tissue of the cheek was then elevated up to the inferior orbital rim, preserving the infraorbital nerve. An osteoplastic window was created, removing a bone flap that was replaced at the end of the case. Once the bony aspect of the procedure was completed, the arms of the robot were docked using the different instrument configurations.
Infratemporal skull base dissection
The infratemporal dissection was performed through the maxillary osteoplastic window. The posterior and medial maxillary walls were removed to provide simultaneous exposure and access to the nasal cavity, nasopharynx, and pterygomaxillary and masticator spaces. The da Vinci Surgical System was then docked with the camera and instrument configurations described above. In the infratemporal skull base dissection, we did not encounter exposure problems, and with the use of the 3-D da Vinci camera, the operating surgeon in the console had a 3-D panoramic view of the operative site. The assisting surgeon had a two-dimensional panoramic view on a standard endoscopic monitor. The surgical assistant had access and could manipulate using standard endoscopic instruments for suctioning, retraction, and complementary tissue dissection.
Soft tissue dissection was done using the 5-mm robotic arms and assisted by standard endoscopic sinus instruments (Fig. 5). The 5-mm Maryland dissector, an important tool in transoral robotic surgery, had limited applicability in the skull base dissection because of its size and limited area of the operative field. We found the 5-mm needle holder much more useful in tissue manipulation. We were able to place four instruments in the operative site without problems of visualization. We also observed that rotating the cadaver's head facilitated a direct trajectory to the target area and lessened the instrument collisions. The nasal passages also gave us access for additional endoscopic instruments for the assistant during the transmaxillary dissections. The neurovascular structure was visualized and dissected without difficulty, and we marked the end of the infratemporal fossa dissection when the following structures were identified and dissected the maxillary artery, middle meningeal artery, maxillary V2 and V3, lateral pterygoid, foramen rotundum, and foramen ovale.
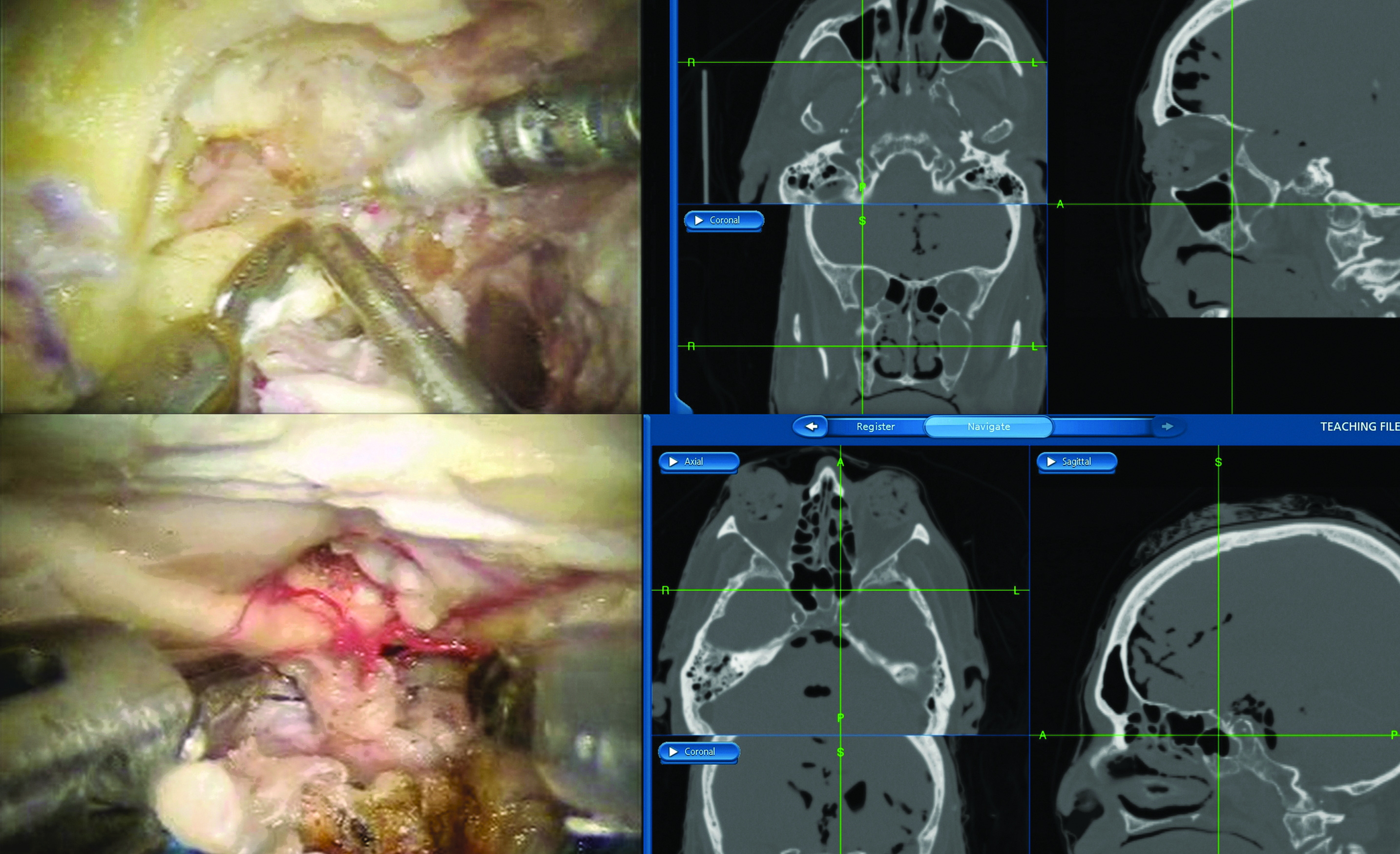
Robotic skull base surgery in the infratemporal area and anterior skull base with surgical navigation.
Transnasal corridor
The 8-mm 3-D camera was able to pass through the nasal corridor after adequate lubrication. We found, however, that the nostril of our cadaver had a tight access for the instrument and 3-D camera. To widen access into the nasal cavity, a rhinoplasty-type transcolumellar incision was made through which the medial crural foot plates were released from the membranous septum. 3 Using Lega's technique, the transnasal corridor was enlarged in a craniocaudal plane by making a marginal incisions along the anterior and posterior margins of the medial crural cartilage.3,5 With the releasing incision at the base of the medial crural foot plate, the skin below the transcolumellar incision was freed from the medial crural cartilages. 3 Releasing the medial crural cartilages allowed the nostrils to open and the nasal tip to reflect superiorly. These maneuvers increased the range of the endoscope in a craniocaudal plane as well as increased the size of the nostrils for placement of the 8-mm endoscope. Structures limiting the 3-D camera in the horizontal plane were the inferior turbinate, septum, and piriform aperture. To widen the nasal corridor in the horizontal plane, the inferior turbinates were out-fractured. Additional width in the horizontal plane was achieved by creating an inferior nasoseptal mucoperichondial tunnel through which the inferior aspect of the nasal septum was disarticulated from the maxillary crest, allowing the septum to be lateralized off the midline.
Anterior skull base dissection
The 3-D camera and one of the instrument arms were passed into the traditional nasal corridor through the expanded nasal corridor. The bone dissection was done as in the conventional endoscopic technique using minimal angle drills and dissectors. The da Vinci arms were used in the soft tissue component of the surgery. The end of the anterior skull base dissection was marked when the structures around the pituitary gland were identified and pituitary resection was complete. A pedicle septal flap was mobilized and sutured to close the anterior skull base resection. Endonasal suturing of the pedicle septal flap to the anterior skull base was feasible. Visual cueing, like tissue tension and tissue deformity, was required to secure the knots and prevent ripping of the tissue being sutured (Fig. 6).

Pedicled septal flap being sutured in place.
During cadaver dissection, without removing the da Vinci endoscopic 3-D camera, we were able to quickly transition from robotic to manual endoscopic dissection, and vice versa, without compromising access and operative site visualization. We also noted the camera from the robotic da Vinci Surgical System gave us a panoramic view of the surgical field.
For the two cadavers, the robotic set-up times for the anterior skull base dissection were 31 and 64 minutes (average, 47.5 minutes), and those for pituitary resection were 55 minutes and 67 minutes (average, 61 minutes). The robotic set-up times for infratemporal dissection were 14 minutes and 9 minutes (average, 23 minutes). Operative times were 65 minutes and 62 minutes (average, 63.5 minutes).
Discussion
Robotic application in skull base surgery is a potential progression in the evolution of endoscopic cranial base surgery. Robotic surgery provides a 3-D view of the surgical field, tremor-free tissue manipulation, and distal articulating arm movement in multiple degrees of freedom not achievable by manual endoscopic instruments. The compact anatomy and limited natural corridors to targets in the skull base have challenged the broad clinical implementation of robotic techniques in cranial base surgery. In this study we evaluated the application of the robotic da Vinci Surgical System in skull base surgery using available instrument arms and modified entry ports.
To access the infratemporal fossa, we created a unilateral maxillary osteoplastic window by removing the anterior wall of the maxillary sinus as a single bone flap. The osteoplastic flap is replaced at the end of the case. The extent of the osteoplastic flap can be modified based on the extent of exposure needed and the location of the target lesion. The window spans the medial and lateral maxillary buttresses in width and starts below the infraorbital nerve to just above the maxillary tooth roots. The osteoplastic flap can be preplated prior to the osteotomy, making it easier to replate at the end of the case.
The skull base has been approached using a bilateral maxillary antrostomy in preclinical robotic studies. 5 The utility of the transmaxillary approach has also been reported by Couldwell et al. 6 and Doglitto et al. 7 for surgery within the cavernous sinus. Extensive lesions inferior and lateral to the sella, such as clival chordomas, could be approached through a partial anthrostomy. 3 Depending on the location of the skull base lesion, access can be through the transoral, transnasal, or transmaxillary approach or a combination of these. We found that a unilateral access point and a wider maxillary osteoplastic window adequately allowed the placement and manipulation of three to four instruments, including the 3-D camera, and eliminated the added morbidity of a bilateral midfacial dissection and antral windows.
The nostrils are a natural orifice for introducing the endoscope and instruments into the nasal cavity but are limited in the access they provide. To expand the nostril window, we released the medial crural cartilages from the caudal septum. Additional adjuvant intranasal techniques can also be used to further expand the nasal corridor for the introduction of the 5-mm robotic instrument if needed. To widen the nasal corridor, the nasal septum can be temporarily disinserted from the maxillary crest through an inferior septal mucoperichondrial tunnel, allowing the septum to swing laterally. In addition, out-fracturing the inferior turbinate provides more access.
Lega et al. 5 in their experience noted difficulty when the camera and the dissection arms were placed along a similar axis. We noted this problem in anterior robotic dissection; however, we did not encounter this problem in the infratemporal region.
We were able to place four instruments as needed through the maxillary window for the infratemporal dissection. The transnasal corridor, even when expanded, still offered a tight room for maneuvering the 3-D camera and instruments for anterior skull base dissection.
Endoscopic techniques further facilitated robotic dissection, and vice versa, making the transition from one technique without changing position and reorientation of the 3-D camera/endoscope. We were able to demonstrate in the present study that the four-handed technique can be achieved in skull base robotics with both the surgeon and first assistant.
In the study of Gonzales et al. 8 with regard to the angle of approach in pterional and orbitozygomatic extensions, they noted that increments in bony removal opened a wider angle in which to work more than they increased the actual amount of working area. This observation supports the use of an expanded maxillary osteoplastic flap over bilateral limited culdwell luc maxillary windows.
We found the EndoWrist® (Intuitive Surgical) 5-mm needle driver more useful for tissue retraction and dissection than the 5-mm Maryland dissector because of its distal articulating tip and size of the tip. The 5-mm needle holder can hold and retract delicate structures for the EndoWrist monopolar tip for dissection. In considering future instruments for robotic skull base dissection, a 5-mm instrument with interchangeable distal articulating tips of varying sizes would be especially useful, and the EndoWrist component of the instrument should be reduced in size to accommodate the operative work space. Development of 5-mm bipolar cautery tips and clip appliers are also needed. Although it would be ideal to have bone instruments and burrs all incorporated in future robotic instruments, in this present study, we were able to use currently available minimal angled drills under the two-dimensional and 3-D panoramic views provided by the robotic camera
Image-guided navigation is an essential aspect of contempory skull base surgery. In the preclinical study by Bumm et al. 9 on the automated robotic approach with redundant navigation for minimally invasive extended transphenoidal skull base surgery, the safety features noted were continuous endoscopic visual control of the operating field, integrated robotic navigation software, and a redundant navigational control system. Their study noted that “the redundant navigation system detects offset between the patient and robot coordinates by supervising all tool movement and maneuvers.” 9 Xia et al. 10 demonstrated the importance of a cooperatively controlled robotic system, navigation system, and added virtual fixtures to enforcing and protecting critical neurovascular structures. In our study, the second assistant is the one placing the navigation probe to determine the anatomical position under instruction by the surgeon. Future robotic surgical design must incorporate a navigation device that can be controlled by the primary surgeon. Regardless of the use of navigation systems, the surgeon should monitor the drilling and dissection and provide the final degree of safety.
Comer et al. 11 reported that the room set-up of transnasal microscopic resection ranged from 76 to 160 minutes and that the interval for endoscopic resection ranged from 36 to 134 minutes. 11 The operative times for transnasal microscopic resection and endoscopic resection were in the range of 79–274 minutes and 31–215 minutes, respectively. 11 Khalifa and Ragab 12 have also reported their operative times in the endoscopic-assisted antral window approach and in endoscopic-assisted midface degloving to the infratemporal fossa as 128±14 minutes and 153±23 minutes, respectively. The operative time for McCool et al. 13 in their infratemporal cadaver dissection ranged from 21 to 72 minutes. In our study, our operative times are comparable to those in the above-mentioned studies.
In the present study the second assistant provided the primary surgeon with his or her haptic interpretation of the structures being manipulated. The primary surgeon also directly palpated structures at intervals during the case prior to proceeding with further dissection. Surgeons have estimated applied contact via visual haptics through tissue deformation and color change of the tissue during applied pressure. 14 Visually estimating applied pressure may also be influenced by the surgeon's surgical experience. Performing manual palpation of structures for confirmation is sometimes required.
Although Van der Meijden and Schijven 15 could not confirm consensus in their review of the value of haptic feedback in conventional and robotic-assisted minimally invasive surgery, they noted the importance of haptic feedback in the early acquisition of psychomotor skills and knot-tying. Wagner et al. 16 found that tissue damage increased by a factor of 3 and the magnitude of force increased by 50% without haptic feedback in blunt dissection experiments. The lack of important tactile feedback in robotic surgery needs to be addressed in the next generation of surgical robotic platforms, especially if robotic surgery is to be applied in skull base surgery.
Commenting on the evolution of endoscopic skull base surgery, Nogueria et al. 17 stated that “the potential current advantages of endoscopic skull base surgery are the lack of external incision, decreased trauma to normal soft tissue and bone, improved visualization, increased access, improved outcomes, fewer complications, rapid recovery, decreased hospitalization, and cost.” The addition of robotic surgery in the skull base region with its inherent advantages needs to be closely evaluated with the above-mentioned parameters.
Conclusions
We have shown that application of the robotic da Vinci Surgical System with currently available instrumentation in skull base surgery of the infratemporal area and anterior skull base is feasible. The infratemporal area can be accessed through a unilateral maxillary osteoplastic window. The anterior skull base region can be accessed through a combined transmaxillary and nasal corridor. Release of the nasal structure can improve passage of the 3-D camera if needed. Endoscopic and robotic techniques and instruments can be combined during surgery, and one can shift instruments or technique as indicated during the procedure. At present, the da Vinci 3-D camera needs to be smaller, and the instrument arms need to be redesigned and developed preferably with distal articulating tips to meet surgical operative needs. Further studies are required in the preclinical stage prior to clinical application.
Footnotes
Acknowledgments
This research was funded by the Milton J. Dance Jr. Endowment. We thank Steve Eliades, MD, PhD, Richard Hirata, MD, FACS, and James Scuibba, DMD, PhD.
Disclosure Statement
No competing financial interests exist.