
Abstract
Abstract
Introduction:
Transumbilical laparoendoscopic single-site (U-LESS) pyeloplasty may provide improved cosmesis compared with conventional laparoscopic pyeloplasty. However, U-LESS pyeloplasty can be challenging because of the need for extensive suturing. The wristed instrumentation of robot-assisted laparoendoscopic single-site (R-LESS) pyeloplasty provides improved dexterity to facilitate intracorporeal suturing. We therefore present our technique and experience with R-LESS pyeloplasty for ureteropelvic junction obstruction (UPJO).
Subjects and Methods:
The da Vinci® S or Si Surgical System (Intuitive Surgical, Sunnyvale, CA) was used in all cases. Ureteral stents were placed cystoscopically at the start of each case. A 3-cm skin incision was made adjacent to the umbilicus. Three ports (12 mm, 8 mm, and 5 mm) were placed either through separate fascial incisions or into a GelPort® (Applied Medical, Rancho Santa Margarita, CA). Key techniques included port staggering, a “chopstick” arrangement of the instruments, and use of a 30° lens in an upward configuration. Traditional dismembered pyeloplasty procedures were performed in all cases. Patients less than 45 years of age with no prior abdominal surgery were offered this approach.
Results:
Eight patients (4 female; 5 right-sided; median age, 22 years) underwent R-LESS pyeloplasty without the need for additional ports. All patients were discharged by the third postoperative day, and 5 were discharged on Day 1. One patient experienced urine leakage, which was managed with a temporary nephrostomy tube. Length of follow-up ranged from 29 to 46 months. No patients have developed symptoms or radiographic evidence of recurrent UPJO.
Conclusions:
R-LESS pyeloplasty can be safely performed for selected patients with currently available robotic equipment. Careful patient selection and case setup are key to successfully performing these procedures.
Introduction
The da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) provides three-dimensional visualization, increased magnification, and wristed instrumentation, which facilitate fine dissection and suturing in restricted areas. Since its initial description in 2009, robot-assisted laparoendoscopic single-site surgery (R-LESS) has been applied to a variety of procedures across multiple surgical disciplines.6,7 Because of the extensive suturing necessary to complete the anastomosis, pyeloplasty is a procedure that would seem well suited to utilize the assistance of the robot. R-LESS pyeloplasty has recently been described, and there may be technologic advancements in the near future that can facilitate the procedure and increase its utilization. 8 As this procedure is in its infancy, data regarding technique and perioperative outcomes are scarce—although this is a procedure that can be accomplished with existing technology. Therefore, we present our experience with R-LESS pyeloplasty and describe our technique for successful completion of this procedure.
Subjects and Methods
Patient demographics
From December 2008 to April 2010, selected patients with UPJO were offered an R-LESS pyeloplasty. Patients were generally offered this approach if they were younger than 45 years old, had no history of prior abdominal surgery, and placed a high value on the cosmetic result of the procedure. Patients with UPJO who did not meet the above criteria were offered standard multiport robot-assisted pyeloplasty and are not included in this report. Preoperative imaging to confirm the UPJO included an abdominal computed tomography scan, diuretic renography, and/or retrograde pyelogram. All procedures were performed by a single surgeon (G.W.). Patient demographic details are listed in Table 1. Clinical data were collected prospectively for quality assurance purposes and retrospectively reviewed with Institutional Review Board approval.
BMI, body mass index; CV, crossing vessels; EBL, estimated blood loss; F, female; M, male; OR, operating room.
Operative technique
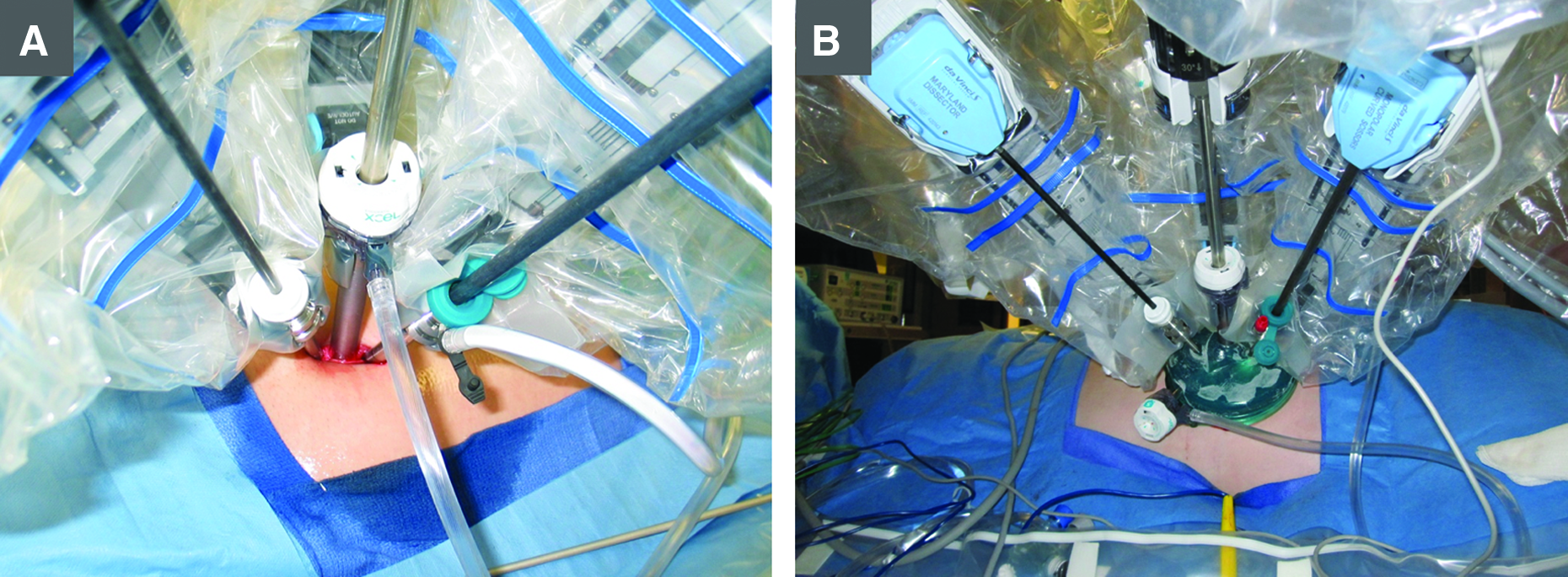
The da Vinci Surgical System S or Si model was used for all procedures. A 6-French ureteral stent was placed with a cystoscope at the beginning of each case. Patients were then positioned in a modified lateral decubitus position. The differences in port and equipment setup between a multiport robotic pyeloplasty and the R-LESS approach are illustrated in Figure 1. A 3-cm skin incision was made along the crease of the umbilicus. After Veress needle insertion, the abdomen was insufflated to 15 mm Hg. A 150-mm-long, 12-mm-wide ENDOPATH® Xcel® trocar (Ethicon, Cincinnati, OH) was inserted in the middle of the incision as the camera port. Two robotic arm ports (5 mm and 8 mm with outlet) were also placed through separate fascial incisions on either side of the camera port (Fig. 2A). Alternatively, a GelPort® (Applied Medical, Rancho Santa Margarita, CA) was placed through a single fascial incision, and then the three ports as well as insufflation tubing were placed through the GelPort (Fig. 2B).
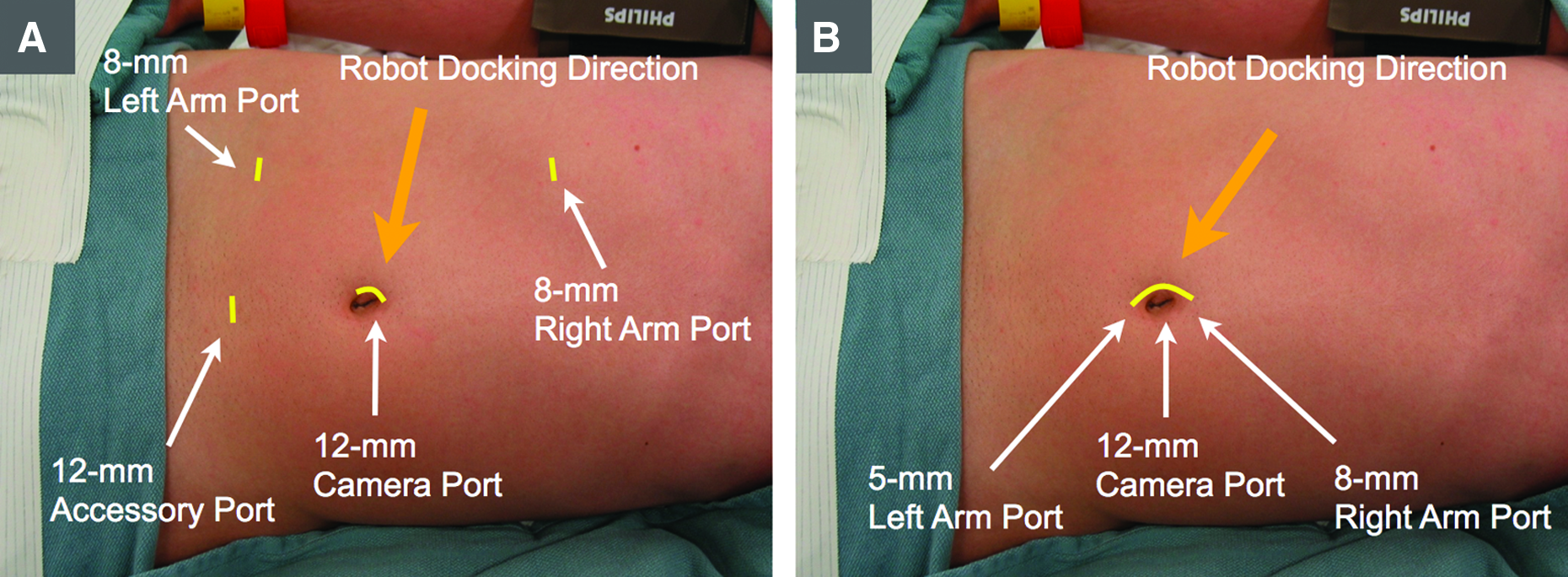
The differences in port and equipment setup between
Port configuration for robot-assisted laparoendoscopic single-site pyeloplasty.
The robotic instruments used in these procedures included an 8-mm monopolar curved scissors (in the left port), a 5-mm Maryland dissector (in the right port), and two 5-mm needle drivers. The robotic instruments were inserted in a “chopstick” configuration, whereby the instruments cross internally at the level of the abdominal wall such that the right-hand controls the left instrument, and vice versa. 9 The two robotic arm ports were staggered caudal to the camera port, which facilitated the docking of the robotic camera-holding arm and two instrument arms in a tight space (Fig. 2). Before docking, a small sponge was inserted into the abdomen to absorb minor bleeding during the surgery. The robot was docked from the posterior side of the patient and from a more cephalad direction compared with traditional robotic pyeloplasty (Fig. 1). A 30° robotic laparoscope was inserted with the lens facing upward to minimize interference between the scope and instruments. Image zooming was primarily done digitally to keep the camera away from the working arms and reduce interference.
For right-sided cases, the ascending colon was mobilized along the hepatic flexure. For left-sided cases, the descending colon was not mobilized, and a transmesenteric approach was used. The previously stented ureter was then identified and mobilized to the renal pelvis. When encountered, lower pole crossing vessels were preserved. Dismembered pyeloplasty with reduction of redundant renal pelvis was then performed in all cases (Fig. 3). Poliglecaprone 25 (Monocryl™; Ethicon) sutures (3-0 and 4-0 on RB-1 needles) were delivered through the 8-mm port for reconstruction of the renal pelvis and ureteropelvic anastomosis, respectively. The fascial incisions were closed with interrupted 0 Vicryl™ (Ethicon) sutures. Approximately 20 mL of 0.5% plain bupivacaine (Marcaine®; Hospira, Lake Forest, IL) was infused into the subcutaneous space around the umbilicus to provide postoperative analgesia. The skin incision was closed with a running subcuticular 4-0 Monocryl suture and covered with Dermabond™ (Ethicon). One patient had four small kidney stones (4–5 mm) that were removed by inserting a 16-French flexible cytoscope with a Zero Tip™ stone basket (Boston Scientific, Natick, MA) through one of the robotic arm ports (Fig. 4). A watertight ureteropelvic anastomosis was confirmed by intravenous injection of methylene blue, with observation of blue dye in the Foley catheter but none leaking from the anastomotic site.
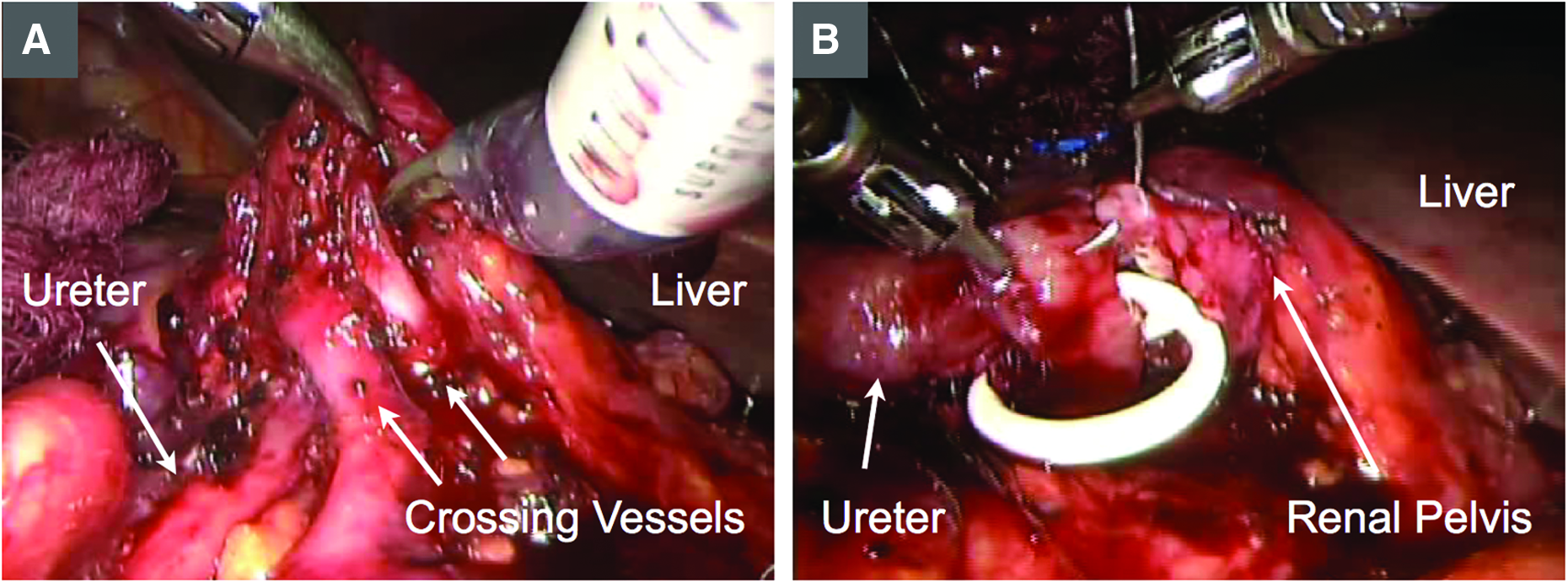
Intraoperative views of a right-sided robot-assisted laparoendoscopic single-site pyeloplasty.
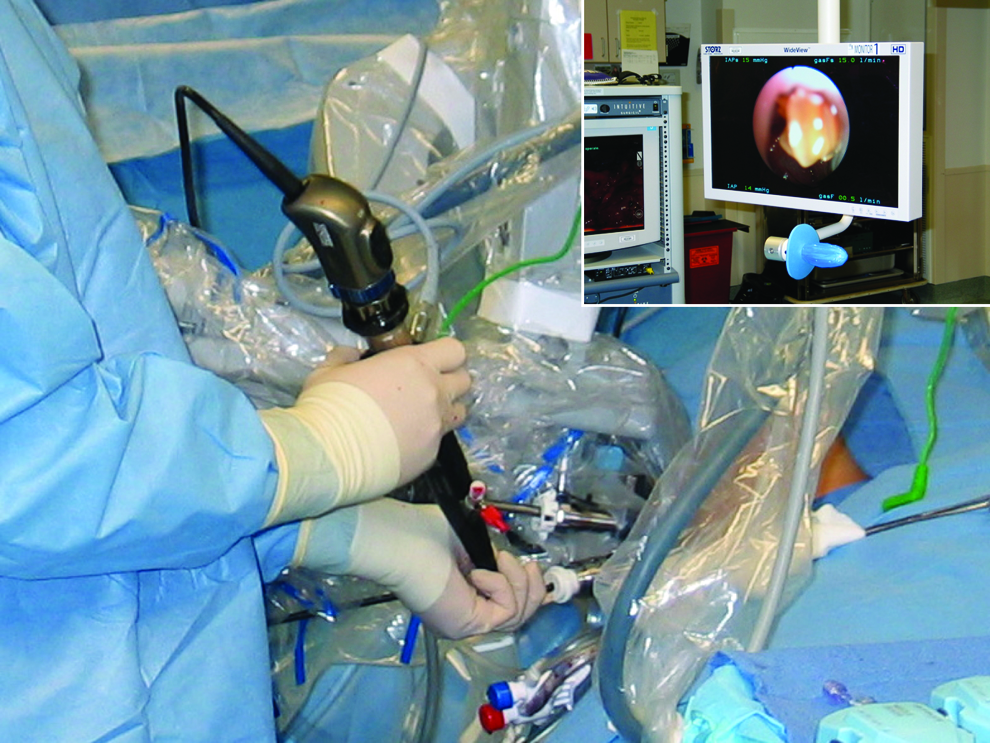
Pyelolithotomy. In 1 patient a flexible cystoscope was inserted through one of the robotic arm ports. A basket was used to remove four small stones from the collecting system prior to ureteropelvic anastomosis.
Results
All 8 cases were completed uneventfully in an R-LESS fashion without the need for additional ports or needle-scopic instruments, and no drains were placed. Primary operative outcomes are listed in Table 1. There were no major differences in operative technique for pediatric versus adult patients. Trocar placement through separate fascial incisions was used in the first 5 patients, and thereafter the GelPort was used. One patient had renal stones associated with his UPJO, and these were removed by pyelolithotomy during the operation. Operative time ranged from 139 to 245 minutes with a mean of 181 minutes. Estimated blood loss was ≤25 mL. Hospital stay ranged from 1 to 3 days, with 5 patients discharged on postoperative Day 1.
One patient developed the sudden onset of severe left flank pain on postoperative Day 6. Rupture of the left renal pelvis was identified on an abdominal computed tomography scan. A nephrostomy tube was placed and removed 12 days later, and the patient had no further sequelae. The exact etiology of this event is unclear, although passage of a blood clot may have temporarily obstructed the ureter and stent. All ureteral stents were removed approximately 5 weeks after surgery. Length of follow-up ranged from 29 to 46 months. No patient has developed symptoms or signs of recurrent UPJO based on diuretic renal scan and either computed tomography scan or renal ultrasound. All umbilical wounds have healed well, without any hernias, with minimal scarring, and with high subjective patient satisfaction in the cosmetic results, although this was not scored (Fig. 5).
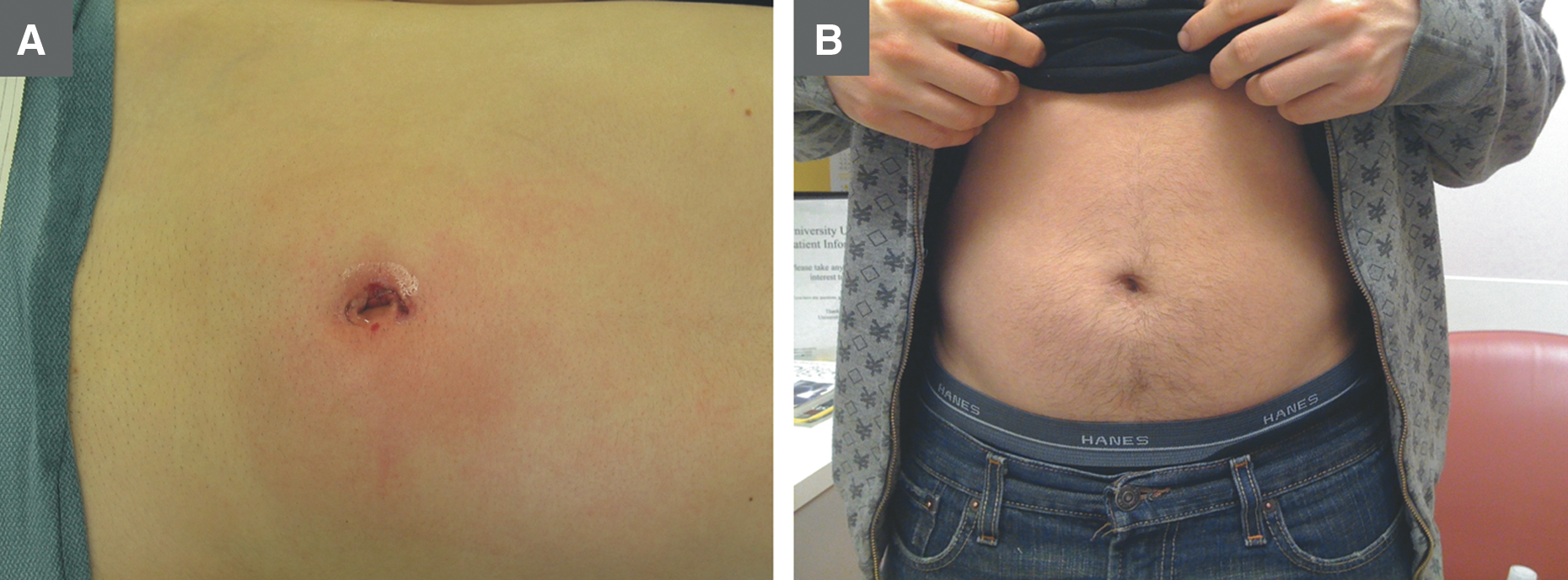
Representative postoperative photographs of robot-assisted laparoendoscopic single-site pyeloplasty cosmetic outcomes:
Discussion
Although the da Vinci Surgical System was not originally designed for this purpose, successful R-LESS surgeries can be performed through strategic port placement and instrument configuration. Just as the robotic approach has allowed more surgeons to complete laparoscopic procedures, the addition of robotic assistance to single-site surgeries may provide an attractive entry point to such procedures for surgeons who are less comfortable with traditional laparoscopy. However, careful planning is necessary to reduce robotic arm collisions and maximize dexterity.
There are several key strategies that are helpful to complete R-LESS pyeloplasty procedures. Placing the robotic arm and camera ports slightly staggered from one another, both in laterality and in depth, helps reduce interference from the ports themselves. We transitioned to use of the GelPort approach because of reduced gas leakage, greater flexibility in port positioning, and the ability to have a small bedside-assistant port. 10 Docking the robot from a more cephalad direction helps aim the camera directly at the ureteropelvic junction area and provides the best view of the operative field because camera mobility is limited compared with conventional robotic pyeloplasty. Placing the robotic instruments in a “chopstick” configuration, originally described by Joseph et al., 9 increases the range of motion of the robotic instruments internally. This also allows for greater separation of the robotic instruments externally, reducing the amount that the robotic arms interfere with one another. Using a 30° lens in the “up” position allows the camera to reside inferior to the working arms inside the patient, further maximizing instrument mobility. Many centers, including our own, have upgraded to the da Vinci Si Surgical System. The robotic arms of the Si system have a slimmer profile and greater mobility compared with the S system, which facilitates the R-LESS approach (our transition to the Si Surgical System occurred during this series). A flexible cystoscope or ureteroscope can also be inserted through one of the working arm ports to perform pyelolithotomy, as was necessary in one of our patients. Additional “needle-scopic” assistant instruments through separate abdominal wall stab incisions can also be used, although they were not necessary in this series.
Large case series of traditional robotic pyeloplasty procedures have been completed, confirming the safety and efficacy of this approach while obtaining the benefits of minimally invasive surgery.11–13 It therefore seems likely that patients undergoing the R-LESS approach would enjoy similar surgical outcomes with an enhanced cosmetic result. All patients in this series had minimal blood loss and a short length of stay and remain free of recurrent obstruction, although 1 patient did require temporary placement of a nephrostomy tube postoperatively to manage a urine leak. It should be noted that the patients in our series were young and healthy and did not have prior abdominal surgery. These criteria were chosen to facilitate learning this technique without potentially complicating factors such as significant intraabdominal adhesions and comorbid conditions. This would seem a prudent approach for other surgeons attempting to use this technique for the first time—most reports of R-LESS pyeloplasty have been limited to small case series in highly selected patients, although results appear promising.4,10 In the first comparative series, Olweny et al. 14 described 10 R-LESS and 15 conventional laparoendoscopic single-site pyeloplasty patients. Although the operative times were longer in the R-LESS group, no conversions were necessary, and only one postoperative complication was noted. This was in contrast to the conventional laparoendoscopic single-site group, of which 3 patients had complications, and all required an additional port to be placed to complete the anastomosis. Cestari et al. 15 recently described the use of a new da Vinci single-site platform that utilizes curved robotic trocars as well as technology to “reverse” the crossed configuration of the instruments (i.e., the surgeon's right hand controls the instrument on the right side of the screen, even though this is technically the left instrument at the bedside). Their median operative time of 160 minutes was shorter than in the present study, although the average length of stay was longer (median, 4 days). Other perioperative outcomes were similar, and the authors stated that the surgery is indeed facilitated with the new technology that is created specifically for single-site surgery.
Although not objectively graded in this series, the single-site approach likely provides greater cosmetic satisfaction than multiport robotic or laparoscopic pyeloplasty because of reduced abdominal skin incisions. Long-term follow-up with cumulating experience and outcomes from comparative case-control series of U-LESS and R-LESS pyeloplasty are necessary to further validate the R-LESS approach for pyeloplasty in terms of perioperative outcomes. We believe that surgeons who perform standard robot-assisted pyleoplasty should consider R-LESS pyeloplasty in healthy young patients who place a high value on cosmesis, as future generations of robotic equipment and accessories developed specifically for single-site surgery are being developed and will likely facilitate this technique.
Footnotes
Disclosure Statement
No competing financial interests exist.