
Abstract
Abstract
Laparoscopic surgery has become common in the treatment of gastric cancer because of improvements of both surgical techniques and devices. The aim of this study was to compare totally laparoscopic distal gastrectomy (TLDG) with laparoscopically assisted distal gastrectomy (LADG) implemented by experienced laparoscopic surgeons. Studies and relevant literature regarding LADG versus TLDG were searched for in the PubMed and Embase databases. Operative time, volume of bleeding, number of retrieved lymph nodes, time to first flatus, duration of postoperative hospitalization, and postoperative complications in LADG and TLDG were pooled and compared by meta-analysis. Odds ratios (ORs) and weighted mean differences (WMDs) were calculated with 95% confidence intervals (CIs) to evaluate the effect of TLDG. Six recent studies of 1644 patients were included in the meta-analysis. Compared with LADG, TLDG had advantages of less bleeding (WMD −17.79, 95% CI −32.57 to −3.02, P=.02), shorter time to first flatus (WMD −0.14, 95% CI −0.23 to −0.06, P=.001), and shorter postoperative hospitalization (WMD −0.32, 95% CI −0.53 to −0.12, P=.002). Operative time, mean number of lymph nodes retrieved, and postoperative complication rate were not statistically different (P>.05). Compared with LADG, TLDG significantly reduced bleeding, time to first flatus, and postoperative hospital stay and can be considered a useful technique for patients with gastric cancer.
Introduction
The first laparoscopically assisted distal gastrectomy (LADG) was reported by Kitano et al. 1 Compared with classical open gastrectomy, it was acknowledged as having advantages such as reduced blood loss and intraoperative pain and shortened postoperative hospital stay.2,3 These advantages are ascribed to the lower invasiveness of laparoscopic surgery. During LADG, lymph node dissection and stomach ablation are performed laparoscopically. However, a minilaparotomy is performed on the epigastrium, through which the anastomosis is performed under direct vision. The narrow and restricted space in which to operate is a key limiting factor, particularly in obese patients with a thick abdominal wall. When all processes are accomplished laparoscopically, the procedure is termed totally laparoscopic distal gastrectomy (TLDG). Digestive tract reconstruction is conducted intracorporeally using laparoscopic stapling devices without any wound on the epigastrium; as a result, TLDG is considered less invasive than LADG.4–6 However, there have been few prospective studies of differences in the clinical results of TLDG and LADG. To clarify the safety and feasibility of TLDG, we compared the surgical outcome of patients treated with TLDG with that of patients treated with LADG.
Materials and Methods
Publication search
Two bibliographic databases (PubMed and Embase) were searched for all related literature in English, including articles referenced in the publications. The medical subject headings and key words searched for individually and in combination were as follows: “totally laparoscopic distal gastrectomy,” “laparoscopically assisted distal gastrectomy,”and “gastrectomy.” The last search was conducted on December 20, 2012.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) histologically proven that the tumor was located in the lower or middle third of the stomach; (2) no evidence of a T4 tumor; (3) body mass index less than 40 kg/m2; and (4) the patient's basic condition was good enough for him or her to undergo surgery. The exclusion criteria were as follows: (1) T4 cancer or huge tumor; (2) operative cardiovascular or pulmonary risk or hepatic or renal dysfunction; (3) high body mass index; and (4) immunocompromise.
Statistical analysis
For statistical analysis, we used Review Manager (RevMan) software version 4.2.09 (Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). Odds ratio (OR) and weighted mean difference (WMD) with 95% confidence intervals (CIs) were used to assess the outcomes of the studies. Heterogeneity was assessed using the chi-squared test with significance set at P<.10. If heterogeneity was limited according to forest plotting, we used the Mantel–Haenszel fixed effect model; if not, the Mantel–Haenszel random effect model was used. The significance of the OR was determined by the Z test and considered to be statistically significant at P<.05. Publication bias was evaluated by funnel plotting with Egger's linear regression test. Funnel plot asymmetry on the natural logarithm scale of the WMD was measured by a linear regression approach.
Results
Study characteristics
Six studies were included in this meta-analysis.7–12 All were published after 2008, and they comprised 1644 patients in total, 656 of whom underwent TLDG and 988 of whom underwent LADG. The sample size of the trials ranged from 40 to 567. Some other studies13–17 reported TLDG but did not report information regarding LADG, so they were excluded from the present meta-analysis. Table 1 lists the main characteristics of the six studies included in the analysis.
BMI, body mass index; LADG, laparoscopically assisted distal gastrectomy; TLDG, totally laparoscopic distal gastrectomy.
Meta-analysis results
Operative time
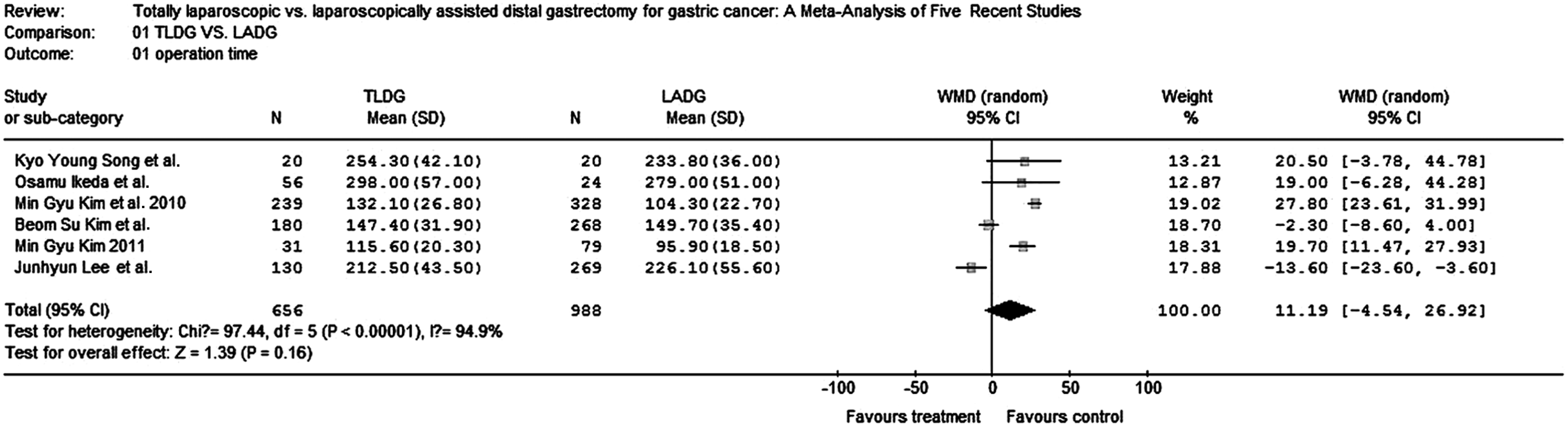
All six studies (1644 patients) provided data on operative time. Pooling the results for LADG and TLDG revealed no significant difference in operative time (WMD 11.19, 95% CI −4.54−26.92, P=.16; chi-squared=97.44, P<.00001) (Fig. 1).
Amount of bleeding
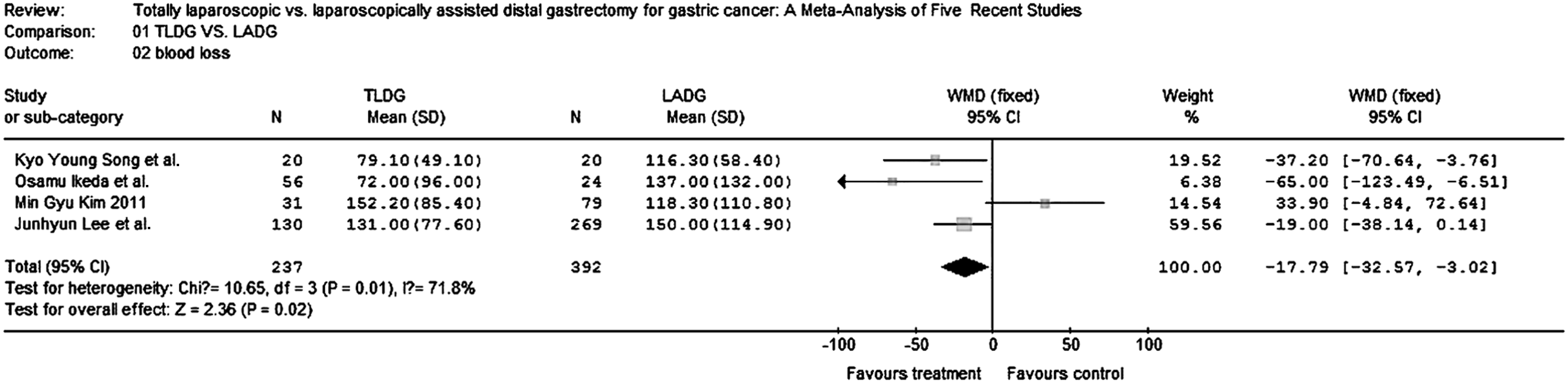
Four studies (629 patients) provided data on amount of bleeding. Intraoperative bleeding was significantly reduced in the TLDG group (WMD −17.79, 95% CI −32.57 to −3.02, p=0.02; chi-squared=10.65, P=.010) (Fig. 2).
Number of retrieved lymph nodes
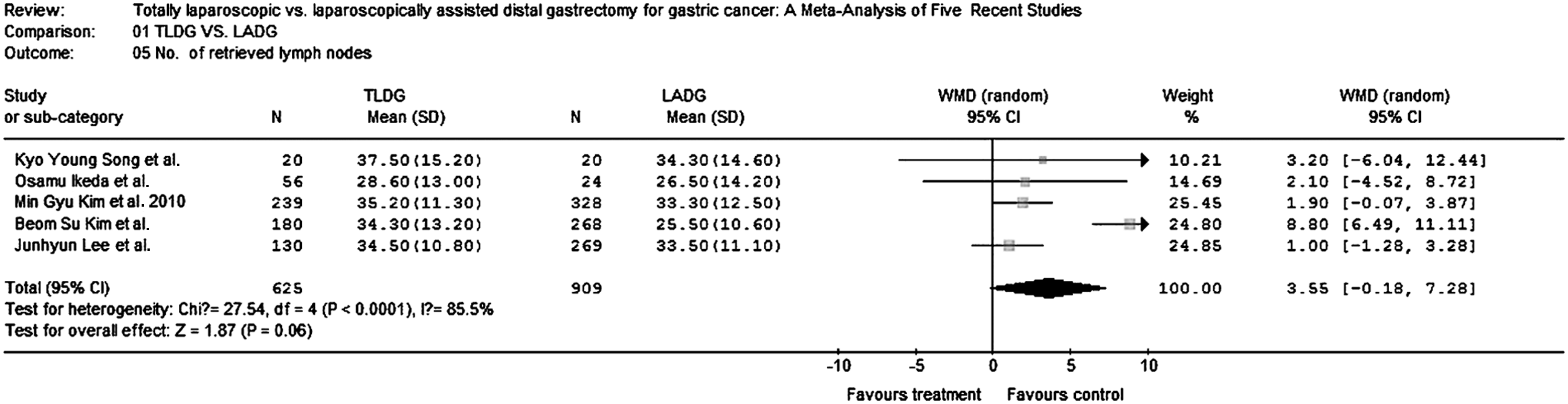
The number of retrieved lymph nodes in LADG and TLDG was measured in five studies (1534 patients). The numbers were similar in the two groups (WMD 3.55, 95% CI −0.18 to −7.28, P=.06; chi-squared=27.54, P<.0001) (Fig. 3).
Postoperative complications
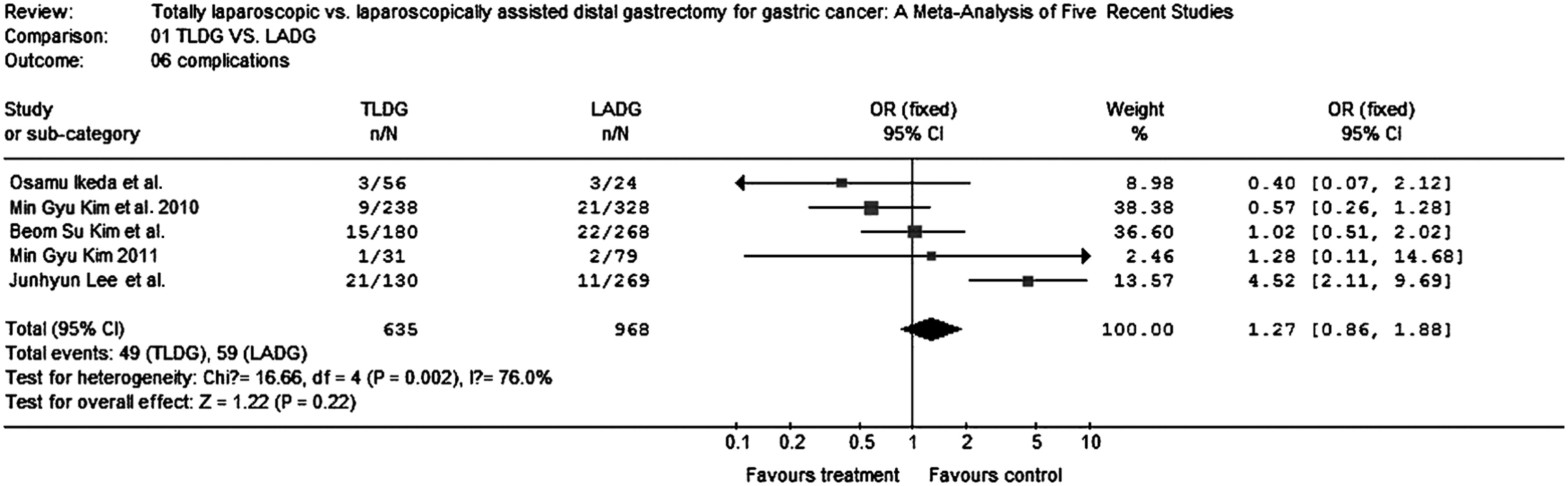
Five studies (1603 patients) compared complications between TLDG and LADG. There was no statistically significant difference between the two groups (OR 1.27, 95% CI 0.86–1.88, P=.22; chi-squared=16.55, P=.002) (Fig. 4).
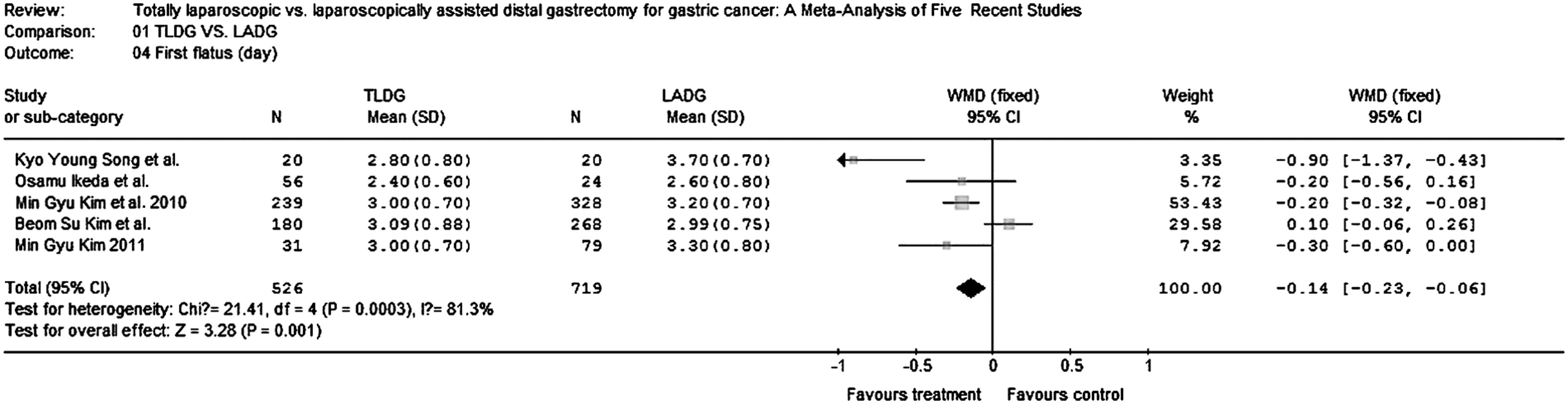
Time to first flatus
Five studies (1245 patients) provided data on the time to first flatus. This was significantly shorter after TLDG than after LADG (WMD −0.14, 95% CI −0.23 to −0.06, P=.001; chi-squared=213.41, P=.0003) (Fig. 5).
Duration of postoperative hospitalization
The number of days spent in hospital was compared in the six studies (1644 patients). Pooling the results, postoperative hospital stay was shorter after TLDG than after LADG (WMD −0.32, 95% CI −0.53 to −0.12, P=.002; chi-squared=22.48, P=.0004) (Fig. 6).

Publication bias
Funnel plotting and Egger's test were performed to assess the publication bias of the studies used. No significant publication bias (P<.05) was found (data not shown).
Discussion
The overall conclusion drawn from the included studies is that, compared with LADG, TLDG has several advantages, including less bleeding and a lower rate of postoperative complications. During LADG, 18 the surgeon usually pulls out and resects the stomach and performs the anastomosis through a small abdominal wall incision, which may cause injury to structures around the anastomosis due to his or her limited vision, especially in an obese patient. Moreover, the minilaparotomy itself may result in operative trauma, although of a degree less than that caused by conventional open surgery needing a large abdominal incision. By contrast, in a completely laparoscopic procedure, the entire intra-abdominal procedure and reconstruction are accomplished by laparoscopy only, with no minilaparotomy 19 ; that is, the entire procedure is observable by the surgeon, and unnecessary manipulations can be avoided. Furthermore, a common belief in this field is that the smallest incision is the least traumatic; thus, TLDG is considered less invasive than LADG. In the present study, we found that, compared with LADG, TLDG had a quicker postoperative recovery, with the time to first flatus being significantly shorter after the latter procedure.
We should regard these outcomes with caution, however, and interpret them critically for the following reasons. First, although no detectable publication bias was found on funnel plotting, the overall methodologic quality and reporting of the included studies were poor. Because of limitations in terms of medical ethics, not all of the studies were randomized controlled trials, and the sample size of some studies was rather low. Second, simply implementing a TLDG or LADG procedure will not ensure results similar to those found in this meta-analysis. Stringent adherence to protocol by all staff and continuous alertness for decreasing compliance also seem to be necessary, as many colleagues involved in TLDG or LADG have reported. The number of studies included in this meta-analysis was relatively low, and the aforementioned quality issues may have biased the results significantly. Thus, more large trials with better separation between TLDG and LADG for gastric cancer seem necessary.
In light of the current evidence, we feel that TLDG should not yet be considered the gold standard for distal gastrectomy. Long-term data on outcome and on other factors important for decision-making are also lacking. Five-year quality of life and physiologic performance have never been described, although these parameters could play an important part in recommending TLDG treatment for gastrectomy. Furthermore, none of the studies addressed long-term mortality and complications after TLDG or LADG, which are crucial in assessing the curative effects of these treatments. It remains the case that most surgeons prefer LADG. The reasons for their reluctance to use the totally laparoscopic technique are as follows. First, most have difficulty with intracorporeal anastomosis, not only regarding the operative technique but also because of deficiencies in laparoscopic devices. Second, many surgeons are concerned about the questionable intraoperative localization. In LADG, surgeons can easily localize the tumor via the minilaparotomy site; however, this is impossible in TLDG. Finally, the use of additional stapling devices 20 makes TLDG more expensive than LADG, a problem that remains to be solved.
In conclusion, this meta-analysis demonstrates that TLDG significantly reduces bleeding and complications compared with LADG but does not retrieve more lymph nodes. A large, randomized trial is needed to demonstrate the superiority of TLDG for gastric cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.