
Abstract
Abstract
Background:
Although laparoscopic splenectomy (Lap-Spleen) has become the standard surgical approach for normal-sized spleens, open splenectomy (Open-Spleen) is still recommended by many in the setting of splenomegaly. We set out to compare the impact of spleen size on Lap-Spleen and Open-Spleen outcomes using a national database.
Study Design:
We reviewed the American College of Surgeons' National Surgical Quality Improvement Program database to identify patients who had undergone non-emergency splenectomy during 2005–2010. To evaluate the impact of spleen size on outcomes, we considered patients with diagnoses of splenomegaly and hypersplenism as those having large spleens (Large-Sp group) and those with diagnoses of primary thrombocytopenia and immune thrombocytopenic purpura as having normal spleens (Normal-Sp group). Patients were also categorized based on surgical approach into Lap-Spleen and Open-Spleen groups.
Results:
We identified 639 patients in the Large-Sp group and 879 patients in the Normal-Sp group. During 2005–2010 laparoscopy was used in 84.2% of cases in the Normal-Sp group (annual range, 77.8%–90.8%). However, the rate of laparoscopy in the Large-Sp group remained consistently below 50% with an average of 41.8% (annual range, 20%–47%). In the Lap-Spleen group, those with Large-Sp had longer operative time and length of stay and higher blood transfusion and morbidity compared with the Normal-Sp group. However, when looking specifically at the Large-Sp group, patients with Open-Spleen had more transfusion requirements, longer length of stay, and higher morbidity, compared with those with Lap-Spleen.
Conclusions:
Lap-Spleen leads to significant improvement in outcomes. These advantages were believed to be limited to normal-sized spleens, but this study demonstrates that laparoscopy can still be advantageous in patients with splenomegaly. We hope such data encourages wider utilization of laparoscopy in the setting of splenomegaly, especially among surgeons who are experienced with the technique.
Introduction
Splenomegaly introduces many challenges to the laparoscopic approach, including difficulty in manipulating the organ and dissection, limited working space, and issues with retrieval of the large spleen. Splenomegaly was therefore considered a relative contraindication for laparoscopy. Although some studies have indicated the feasibility and safety of the laparoscopic approach in patients with splenomegaly,4–6 other studies have shown worsened outcomes in this patient group,7,8 with the laparoscopic approach leading to higher morbidity (especially bleeding) and longer operative times. These authors have therefore advocated for open splenectomy (Open-Spleen) in patients with splenomegaly.
Much of the controversy in the field rises from the inherent scarcity of elective splenectomy, especially in the setting of splenomegaly, which leads to studies with limited number of cases mostly from single institutions. As expected, such studies demonstrate different results based on patient, surgeon, and institution characteristics. Also, most of these case series span over a decade and might not fully reflect the increased laparoscopic experience of the surgeons or recent improvements in techniques and devices. We therefore set out to review a large cohort of patients from a multi-institutional national database that accurately and extensively tracks postoperative complications, to compare Lap-Spleen and Open-Spleen outcomes in patients with splenomegaly.
Subjects and Methods
We reviewed the American College of Surgeons' (ACS) National Surgical Quality Improvement Program (NSQIP) database. ACS-NSQIP is a multi-institutional database prospectively collected at each institution by trained nurse reviewers in a standardized fashion. The participant institutions go through a periodic review process to ensure data accuracy, and studies have demonstrated quality and reliability of the collected data. 9 For this study, we considered other large available clinical databases, including the National Inpatient Survey; however, we chose the ACS-NSQIP as it accurately tracked 30-day morbidity and mortality, which is of great importance for surgical decision making.
Patients
Over 1.3 million procedures were recorded in the ACS-NSQIP during 2005–2010. We included patients who were 16 or more years old, had undergone elective splenectomy, had procedures with CPT codes 38100 or 38120, and had a postoperative diagnosis with International Statistical Classification of Diseases, 9th revision (ICD-9) codes of 789.2 (splenomegaly) or 289.4 (hypersplenism), 287.3 (primary thrombocytopenia), or 287.31 (immune thrombocytopenic purpura [ITP]).
We divided patients based on CPT codes: 38100 to the Open-Spleen group and 38120 to the Lap-Spleen group. Because neither spleen sizes nor weights are recorded in the ACS-NSQIP database, we used the postoperative diagnosis as a surrogate for spleen size. We considered patients with diagnoses of splenomegaly and hypersplenism (ICD-9 codes 789.2 and 289.4, respectively) as those having large spleens (Large-Sp group) and patients with postoperative diagnoses of primary thrombocytopenia and ITP (ICD-9 codes 287.3 and 287.31, respectively) as those having normal spleens (Normal-Sp group). We also performed an internal validation of this assumption using our institutional NSQIP database. For this purpose we received Institutional Review Board approval. We included the patients who met our primary inclusion criteria. Medical records, pathology reports, operation notes, and radiological images from these patients were reviewed. We defined a normal spleen as one that weighed <300 mg or was <13 cm in length. Splenomegaly was defined as a spleen that was >500 mg or >15 cm in length.
To validate the assumption that those with a postoperative diagnosis of splenomegaly and hypersplenism (ICD-9 codes 789.2 and 289.4, respectively) indeed had large spleens (Large-Sp group) and those with postoperative diagnoses of primary thrombocytopenia and ITP (ICD-9 codes 287.3 and 287.31, respectively) had normal-sized spleens (Normal-Sp group), we reviewed our own institutional NSQIP database and identified 101 patients with a splenectomy. Of these, 28 met our inclusion criteria.
Using our study definitions, all 6 patients who were categorized in the Normal-Sp group had in fact a normal-sized spleen that weighed less than 250 g. Twenty-two patients were categorized in the Large-Sp group, 18 of whom had spleens weighing over 500 g. From the remaining 4 patients, 3 had a radiologic study consistent with splenomegaly with maximum splenic length of over 15 cm. This study provided confirmation that postoperative codes in the ACS-NSQIP database can provide reliable insight to the size of the spleen.
Variables
Race was dichotomized into white and minorities. American Society of Anesthesiologists (ASA) physical classification was dichotomized as ≥3 (severe) or below 3. To be consistent with the literature we considered the surgical length of stay (LOS) for LOS. All 23 adverse events recorded in the ACS-NSQIP database were summed up, and any patient with at least one complication after the surgery was categorized as having morbidity. The occurrences of superficial surgical site infection (SSI), deep incisional SSI, and organ space SSI were summed as SSI. Mortality was considered as death that occurred within 30 days after surgery.
Statistical analysis
Statistical analysis was carried out in two stages; in the first stage patients in the Large-Sp group who had a Lap-Spleen were compared with patients in the Normal-Sp group who also had a Lap-Spleen. In the second stage these patients were compared with those in the Large-Sp group who had undergone Open-Spleen.
Statistical analysis was performed using SPSS version 16 software (SPSS Inc., Chicago, IL). Continuous variables are reported as median with interquartile range (except for mean blood transfusion, which is reported as mean with 95% confidence intervals) and were compared using the Mann–Whitney test. Comparison of categorical outcomes was carried out using the chi-squared test and Fisher's exact test (when appropriate). Multiple linear and logistic regressions were performed to control for differences in preoperative variables, including age, gender, body mass index (BMI), and ASA level, that have shown to have impact on splenectomy outcomes.10,11 P values <.05 were considered significant.
Results
We identified 639 patients in the Large-Sp group and 879 patients in the Normal-Sp groups. Throughout the study period (2005–2010), in the Normal-Sp group the laparoscopic approach was used in 77.8%, 90.8%, 83.0%, 82.8%, 86.3%, and 81.1% of patients in 2005, 2006, 2007, 2008, 2009, and 2010, respectively (weighted mean, 84.2%). However, the rate of utilization of the laparoscopic approach in the Large-Sp group was consistently lower (20.0%, 46.1%, 32.8%, 42.3%, 45.2%, and 46.5% in 2005, 2006, 2007, 2008, 2009, and 2010, respectively). Although the rate of laparoscopic approach increased in this subgroup from 20% in 2005 to 47% in 2010 (P=.02), it remained below 50% (weighted mean, 41.8%) throughout the study period (Fig. 1).
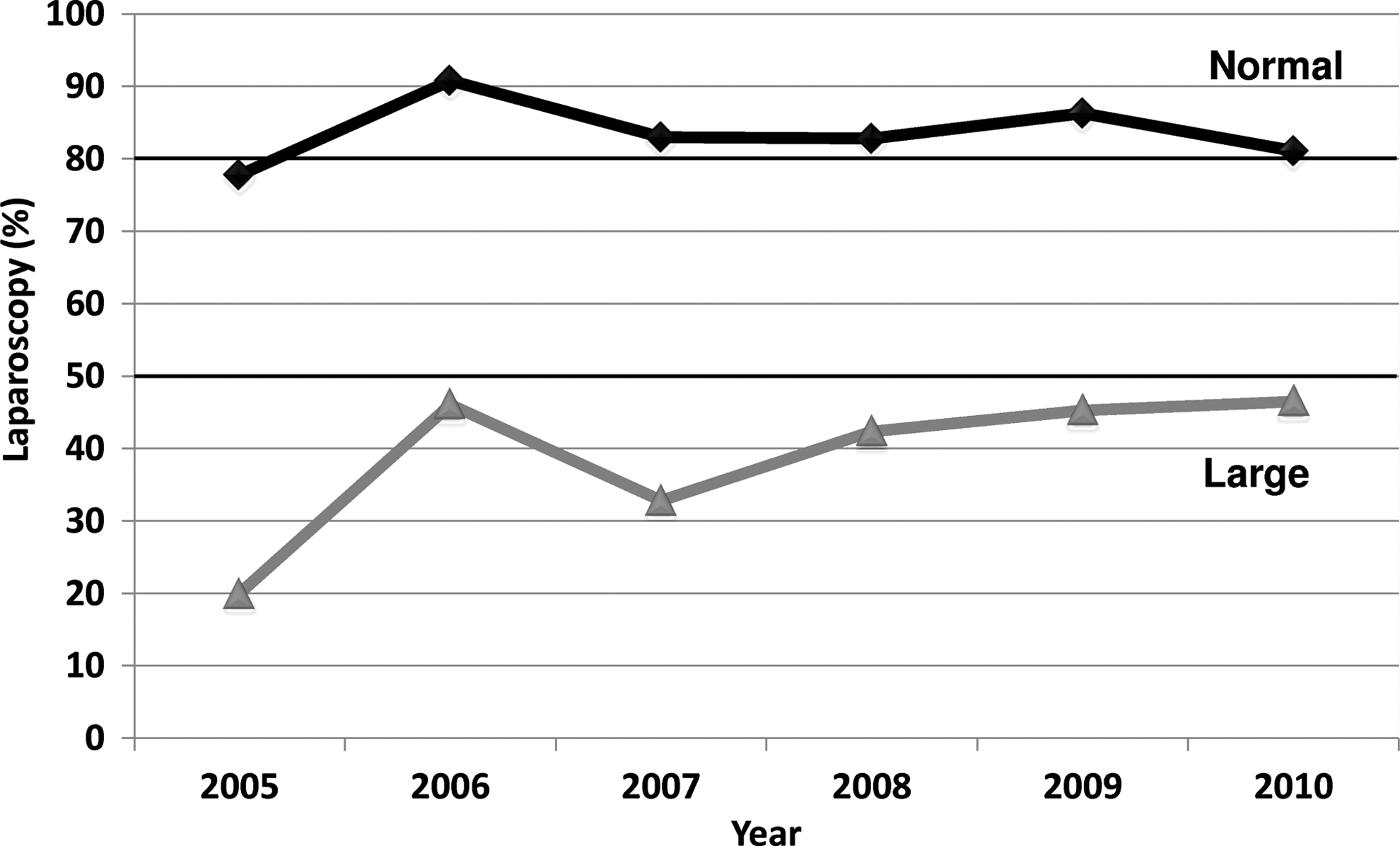
Prevalence of laparoscopic splenectomy during 2005–2010.
In the first set of analyses, we identified 1007 patients who had undergone Lap-Spleen, with 740 (73%) in the Normal-Sp group and 267 (27%) in the Large-Sp group. Patients in the Large-Sp group were older (median age, 55 versus 48 years) and proportionally more male (52% versus 37%) (Table 1). There were no statistically significant differences among patients with regard to BMI (27 kg/m2 versus 28 kg/m2), race (86% versus 81% white), or patients with ASA level 3 and higher (62% versus 55%) (Table 1).
Interquartile range is reported in parentheses for continuous variables (95% confidence interval of the mean is reported for mean blood transfusion).
ASA, American Society of Anesthesiologists; BMI, body mass index; LOS, surgical length of stay; NS, not significant.
In terms of outcomes, those in the Large-Sp group undergoing Lap-Spleen required more blood transfusion (mean, 0.4 packs versus 0.2 packs; P<.001) and had a longer operative time (median, 142 minutes versus 107 minutes; P<.001) and longer LOS (median, 3 versus 2 days; P<.001) compared with Normal-Sp group patients undergoing laparoscopic resection. They also had a significantly higher rate of morbidity (18% versus 11%; P=.009). No significant difference was found regarding the mortality rates between the two groups (Table 1).
For the next set of analyses, we focused on the cohort of patients in the Large-Sp group and compared those that had a laparoscopic versus an open resection. Those undergoing Lap-Spleen were younger (55 versus 59 years) with a slightly higher BMI (27 kg/m2 versus 26 kg/m2) (Table 2). No significant difference was observed in terms of gender (48% versus 46% female), race (86% versus 86% white), and ASA level (62% severe versus 68% severe) for Lap-Spleen versus Open-Spleen, respectively.
Interquartile range is reported in parentheses for continuous variables (95% confidence interval of the mean is reported for mean blood transfusion).
ASA, American Society of Anesthesiologists; BMI, body mass index; Lap-Spleen, laparoscopic splenectomy; LOS, surgical length of stay; NS, not significant; Open-Spleen, open splenectomy.
Regarding the outcomes, of patients in the Large-Sp group, those who underwent Lap-Spleen required less blood transfusion (mean, 0.4 packs versus 1.0 packs; P<.001) and had a lower incidence of postoperative bleeding (6% versus 12%; P=.007) and SSI (2% versus 7%; P=.009). The Lap-Spleen group also had a shorter LOS (3 days versus 5 days; P<.001) and overall morbidity rate (18% versus 32%; P<.001) compared with the Open-Spleen group. The mortality rate was not significantly different between the two groups (1.5% versus 4%). Lap-Sp cases, however, took longer to perform (142 versus 108 minutes; P<.001).
Among patients in the Large-Sp group, by linear multiple regression analysis controlling for age (β=0.02, P not significant), gender (β=0.08, P not significant), BMI (β=–0.04, P not significant), and ASA (β=0.14, P=.003), the open approach was a significant predictor of LOS (β=0.18, P<.001). Logistic regression analysis confirmed that patients undergoing Open-Spleen have a higher risk of having a morbidity (odds ratio=2.2; P<.001) adjusted for age, gender, BMI, and ASA (Table 3).
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; NS, not significant.
Discussion
Lap-Spleen offers many advantages over Open-Spleen and has become the standard approach in the majority of patients undergoing splenectomy. Early experience with the laparoscopic approach in patients with splenomegaly demonstrated the feasibility of this technique in this subgroup. Although these results were encouraging, other reports of higher morbidity and inherent difficulties of the laparoscopic approach in the setting of splenomegaly have led many surgeons to shy away from Lap-Spleen in such patients, as evidenced by significantly lower usage of laparoscopy in our multi-institutional cohort of patients undergoing splenectomy (Fig. 1). Although the usage of laparoscopy in patients with splenomegaly has been increasing in recent years, the rate has remained below 50% throughout the 2005–2010 period.
We initially looked at all patients undergoing Lap-Spleen and, using postoperative diagnosis as a surrogate for spleen size, divided them to two groups: Normal-Sp and Large-Sp groups. The Normal-Sp group was younger and proportionally more female in comparison with the Large-Sp group, reflecting the demographics of the underlying diseases. In line with findings of Heniford et al. 12 and Terrosu et al., 13 we found that patients with splenomegaly undergoing Lap-Spleen had a higher rate of blood transfusion, as well as a longer operative time and LOS. The morbidity rate (17.6%) was also significantly higher than that observed in patients with a normal-size spleen (11.4%), consistent with reports from Patel et al. 8
These data clearly showed that in patients undergoing Lap-Spleen, a large spleen is associated with increased operative time and morbidity. Although some have used such data to argue against the use of the laparoscopic approach in the setting of splenomegaly, we felt that before reaching such conclusion we should consider the comparison of outcomes of Lap-Spleen versus Open-Spleen in the patient population with a large spleen, thus providing a novel angle to the study.
When looking at patients with a large-size spleen, patient characteristics of those who underwent a laparoscopic resection were comparable to those who underwent an open resection as they shared the same postoperative diagnoses and had similar gender and race distribution. Also, noticeably, the percentage of patients with ASA levels of 3 and higher was comparable (62% versus 68% in the Lap-Spleen group versus Open-Spleen group, respectively). Although there were slight differences in terms of age (median of 55 years for the Lap-Spleen group in comparison with 59 years for the Open-Spleen group) and BMI (which was higher in the Lap-Spleen group), these differences were small and unlikely of clinical significance. Furthermore, neither age nor BMI demonstrated any significant impact on outcomes in multivariate analysis.
We found that in patients with splenomegaly, the laparoscopic approach was associated with lower transfusion requirements, shorter LOS, and lower morbidity rate. Regression analysis verified that, controlling for age, sex, BMI, and ASA, the open approach continued to be a significant predictor of LOS and morbidity. Although the laparoscopic approach led to these improvements in outcomes, the operative times were longer by approximately 30 minutes. These findings were consistent with findings of Targarona et al., 6 Owera et al., 14 and Feldman 15 and a recent meta-analysis by Bai et al., 16 who demonstrated shorter LOS for Lap-Spleen in the setting of splenomegaly. Similar to our observations, Watanabe et al. 17 reported significant lower transfusion requirement with laparoscopy in their cohort of 43 patients with hypersplenism. We observed a 17.6% morbidity rate in Lap-Spleen patients with splenomegaly, which was significantly lower than the 31.5% observed in the Open-Spleen patients. These rates are consistent with other smaller case series published in the literature and the meta-analysis by Bai et al. 16 Zhou et al. 18 studied 62 patients with splenomegaly and also reported a significantly higher morbidity rate in their Open-Spleen group (34.5% versus 9.1% for the laparoscopic group). Cai et al. 19 have also reported a higher complication rate for their open group (41.7%) in comparison with their laparoscopy group (12.5%) in patients with hypersplenism. Our observed mortality rate of 1.5% in Lap-Spleen patients with splenomegaly is similar to the findings of Bourgeois et al. 11 The 4.0% mortality rate in the Open-Spleen group is also within the range of 0.2%–4.2% mortality rate for splenectomy in previous studies.
Considering the overall patient cohort as well as those with splenomegaly, the only outcome that was not in favor of the laparoscopic approach was operative time, a finding that has been reported and confirmed by others.7,12,14,20,21 Although the increased operating room time leads to increased operative costs, it has been shown that increased operative costs can be offset by shorter LOS. 22 In our study, regression analysis confirmed that the open procedure is a significant factor that impacts LOS after adjusting for other patient characteristics (age, gender, BMI, and ASA). We therefore believe that despite the increased operating room time, the laparoscopic approach is likely to be a cost-effective approach that also provides many advantages to the patient.
There are some limitations to our study, mostly related to the limitations of the database. We used postoperative diagnosis as a surrogate for spleen size as the spleen length and weight were not recorded in the database. We addressed this limitation by performing an internal validation of the reliability of postoperative diagnosis, using our own institutional NSQIP database. If we consider splenomegaly as a spleen weighing over 500 g or over 15 cm in length, we had only 1 case (3.6%) where the postoperative code did not truly reflect the spleen size. We believe this is an acceptable error rate for such a large study, and the data showed a distinct size difference between normal size and large size in our NSQIP dataset. We acknowledge that spleen size distribution in the Large-Sp group is not homologous and includes patients with splenomegaly (>500 g or >15 cm) as the majority of patients with massive spleens (>1000 g or >20 cm). Unfortunately, we do not have the data to provide a more detailed analysis of spleens weighing >500 mg, which are grouped together in this study. In our own institutional review, we did, however, have spleens weighing >1800 g that underwent a successful laparoscopic splenectomy, confirming that the laparoscopic approach is feasible even in the setting of massive splenomegaly. We also did not have data on conversion rates. There might be other considerations for an open procedure that were not captured in the databases such as previous multiple abdominal surgeries precluding a laparoscopic approach. Such limitations are inherent to most databases; however, without using such a large database we will not have been able to gather an appropriately large enough cohort to answer this important clinical question. We also cannot rule out potential selection bias; in fact, our intuitional review demonstrated that the majority of laparoscopic cases in the setting of splenomegaly are performed by a few surgeons, whereas others preferred the open approach. We hope that our findings would change such a pattern and lead to surgical decision making based on evidence rather than personal preferences, especially in those familiar with the laparoscopic techniques.
In conclusion, this study demonstrates that although Lap-Spleen patients with a large spleen have less favorable outcomes in comparison with Normal-Sp patients, laparoscopy can still be advantageous in patients with splenomegaly in comparison with the open approach, albeit with a modest increase in operative time. We hope this evidence encourages wider utilization of laparoscopy (including hand-assisted laparoscopic surgery) in the setting of splenomegaly, which is presently used in less than 50% of cases.
Footnotes
Acknowledgments
The American College of Surgeons' National Surgical Quality Improvement Program and the hospitals participating in this program are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors. The manuscript has been read and approved by the authors.
Disclosure Statement
No competing financial interests exist.