
Abstract
Abstract
Background:
Laparoscopic intracorporeal suturing and knot tying for anastomosis are considered the most difficult laparoscopic skills to master. The aim of this study was to establish the safety and efficacy of barbed suture for intestinal sutures to close the gastrojejunal anastomosis in obese patients undergoing gastric bypass.
Study Design:
All consecutive patients undergoing gastric bypass were screened for enrollment in our study. Patients were randomly allocated to undergo knotless anastomosis with barbed suture (V-Loc™ 180; Covidien, Mansfield, MA) (case group) or knot-tying anastomosis with 3/0 polyglactin sutures (Polysorb®; Covidien) (control group). The primary outcome was the time needed for the gastrojejunal anastomosis and the operative time. The secondary outcomes were the incidence of leak, bleeding, and stenosis and the evaluation of the cost of the different procedures evaluated.
Results:
Among the 60 consecutive patients enrolled in our study, 30 underwent knot-tying anastomosis, and 30 underwent knotless anastomosis. The time needed for the anastomosis was significantly less (P<.001) in the knotless group, whereas no significant differences were found between the two groups for operative time (P=.151). We recorded one leak in the control group and one leak in the case group (P=1.000). One bleeding in the case group (P=1.000) and no stenosis in either group was recorded. Finally, in our experience, the knotless anastomosis was cheaper than the knot-tying anastomosis (P<.001).
Conclusions:
Our study appears to be encouraging to suggest the use of barbed suture for gastrointestinal anastomosis.
Introduction
Barbed sutures have recently been proposed to facilitate laparoscopic suturing. One of these novel sutures, the V-Loc™ 180 (Covidien, Mansfield, MA), consists of a barbed absorbable thread, armed with a surgical needle at one end and a loop at the other end, which is used to secure the suture. The barb and loop-end make it possible to approximate the tissues without the need to tie surgical knots. To date, the efficacy of this new method has been evaluated in different types of surgery,5–14 but few studies about general surgery are available.2,3 The aim of this study was to establish the safety and efficacy of barbed suture for intestinal sutures to close the gastrojejunal anastomosis in obese patients undergoing gastric bypass.
Patients and Methods
After local ethical committee approval and written informed consent signature, all consecutive obese (body mass index >40 kg/m2) adult patients undergoing gastric bypass were screened for enrollment in our study between September 2010 and June 2012. Only age younger than 18 years and inability to consent to the study were considered as exclusion criteria.
All surgical procedures were performed by the same surgeon, experienced in laparoscopic surgery (more than 500 laparoscopic surgical procedures) using the mini-gastric bypass technique.
The gastrointestinal anastomosis (GIA™; Covidien) stapler divides the stomach at the junction of the body and antrum, at a location where the jejunal loop can be brought up comfortably. An Ewald tube, roughly the diameter of the esophagus, is passed by the anesthetist and held against the lesser curvature. The division of the stomach against the tube is completed, with six lines of staples that seal the gastric pouch. The division of the stomach is parallel to the lesser curvature and up to the angle of His. No short gastric vessels are divided. The bypassed stomach lies on the patient's left, and the narrow lesser-curvature gastric pouch lies on the patient's midline to the right of the bypassed stomach. A point is selected on the small bowel about 200 cm distal to the ligament of Treitz. The jejunal loop is brought up antecolic, and the Endo-GIA stapler is used to anatomose the stomach and the small bowel at this point. The distal end of the gastric tube is anastomosed to the side of the small bowel (Fig. 1). Finally, laterolateral gastrojejunal anastomosis using a linear stapler requires closure of the enterotomies.
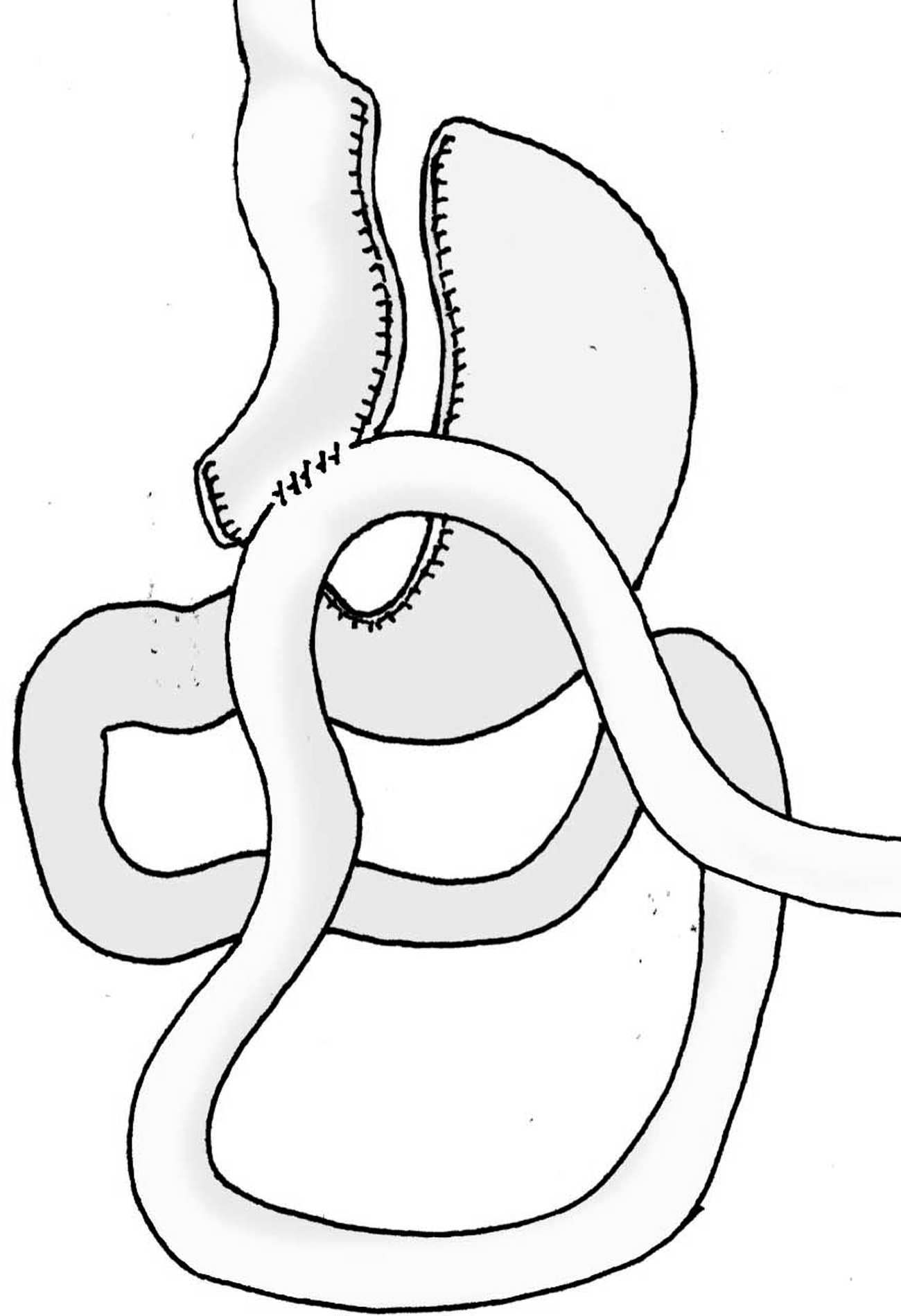
Diagram of mini-gastric bypass.
Patients were randomly allocated by sealed envelopes, according to a computer-generated sequence of random numbers, to undergo knotless anastomosis with barbed suture (V-Loc 180) (case group) or knot-tying anastomosis with 3/0 polyglactin sutures (Polysorb®; Covidien) (control group). The study was designed to obtain a 1:1 case:control ratio.
For the case group, the closure was started by passing the needle through a small loop at the end of the suture that was positioned intraluminally (no knot was tied) and was finished by taking two additional bites beyond the end of the enterotomy incision. The suture was cut flush to the bowel without a knot (Fig. 2). A barbed suture of 23 cm has been used to assure the complete closure of the enterotomy with a single suture. The control incisions were closed routinely by securing the running suture with three square knots at both ends. The number and spacing of bites were left to the surgeon's discretion. To facilitate handling of the surgical knot, one suture was used for each knot (all sutures were cut with a length of 12 cm).

Diagram of gastrojejunal anastomosis with barbed suture:
After the intervention, each subject was re-evaluated every 15 days with an overall follow-up of 6 months. Those patients with missing follow-up visits were excluded from the study.
The primary outcome was the time needed for the gastrojejunal anastomosis and the operative time. The secondary outcomes were the incidence of leak, bleeding, and stenosis and the evaluation of the cost of the different procedures evaluated.
Statistical analysis was performed with SPSS version 15.0 software (SPSS, Inc., Chicago, IL). The Yates's corrected chi-squared test was used as a means of evaluating differences in categorical variables, and the independent t test was used for continuous variables. To adjust for covariates and to make predictions, linear and logistic regression models were used. Statistical significance was accepted for P values <.05.
As for the sample size evaluation, planning a study of independent cases and controls with one control per each case, with an expected difference in the time needed for the gastrojejunal anastomosis of >5 minutes, an α error of <5%, and a power of >90%, we would need to enroll at least 24 experimental subjects and 24 control subjects.
Results
Of the 72 subjects screened for enrollment in this study, 12 patients were excluded because of the exclusion criteria. In particular, 3 were ≤18 years old, and 9 denied their consent to the study.
Among the 60 consecutive patients enrolled in our study, 30 underwent knot-tying anastomosis (control group), and 30 underwent knotless anastomosis (case group). Baseline clinical and demographic characteristics were similar between the two groups (Table 1).
ASA, American Society of Anesthesiologists; BMI, body mass index.
Whereas for the knotless anastomosis a single barbed suture has been used, for the knot-tying anastomosis up to seven polyglactin sutures have been used (Table 2). The time needed for the anastomosis was significantly less (P<.001) in the knotless group, whereas no significant differences were found between the two groups for operative time (P=.151) (Table 2 and Fig. 3). We recorded one leak in the control group and one leak in the case group (P=1.000). One bleeding in the case group (P=1.000) and no stenosis in either groups were recorded. In particular, the two leaks were located along the enterotomy closure. All leaks were treated by drainage and fasting. No surgical interventions were needed. Finally, in our experience, the knotless anastomosis was cheaper than the knot-tying anastomosis (P<.001) (Table 2).

Time needed for knotless and knot-tying anastomosis. Each point represents a single procedure.
A multivariate logistic regression analysis showed that, after adjusting for all the other clinical and demographic parameters, a shorter time needed for the anastomosis was significantly predicted by the use of knotless anastomosis (β=−0.949, P<.001). Separate regression models showed that none of the evaluated variables was a predictor of bleeding, stenosis, or leak development.
Discussion
This is the first prospective randomized controlled study evaluating the efficacy of V-Loc suture on gastrojejunal anastomosis in human subjects undergoing gastric bypass.
Obesity is associated with numerous comorbidities affecting virtually every organ system, including hypertension, type 2 diabetes mellitus, coronary artery disease, dyslipidemia, infertility, certain cancers, and, in the end, increased mortality.15–18 Since 1991, the National Institutes of Health Consensus Panel has recommended the use of surgery to manage the growing problem of obesity. 19 The mini-gastric bypass is safe, results in major weight loss, has a short operating time, and has a short hospital stay. 20
One of the most challenging steps during this procedure is the construction of the gastrojejunal anastomosis. Laparoscopic intracorporeal suturing and knot tying for anastomosis are considered the most difficult laparoscopic skills to master.1–4
The V-Loc 180 closure device is a unidirectional barbed variant of the absorbable copolymer polyglyconate. Tissue-closing strength is approximately 50% at 30 days, with complete absorption in 180 days. Although etching the barbs reduces the core diameter of these sutures, they have been sized according to their postetching diameter, and 3-0 V-Loc suture has the same tensile strength as 3-0 Maxon™ (Covidien). A loop at the end of the suture can be used for knotless suturing, and the first 2 cm of the suture is without barbs to allow throws to be readjusted before the barbs are engaged.
Separated and running sutures are both suitable for closing intestinal openings. Running suture is usually faster than separated ones, but its downside is the loss of tension on the suture line. The aim of this study was to prove the safety of barbed suture, as it seems to associated with the advantages of both sutures, in terms of operative time and tension.
To date, the efficacy and suitability of barbed sutures have been reported in gynecologic,5–7 plastic,8,9 urology,10–13 and orthopedic surgery, 14 but no large study in general surgery has been published. Although usage has been previously described with animal subjects,1,4 the first report of barbed sutures in gastric or bowel anastomosis on human subjects included a very small number of patients, and a more recent report compared retrospectively two consecutive groups without randomization.2,3
Our results showed that the knotless, unidirectional barbed suture reduced the time required to close the anastomosis, compared with a conventional suture with intracorporeal knots, without impact on surgical complications. Moreover, we have shown the knotless anastomosis with barbed suture was cheaper than the conventional knot-tying anastomosis.
The relatively small sample size makes it unlikely to define conclusive results. Further studies are needed to address the safety and efficacy of barbed suture for intestinal sutures. On the other hand, our study appears to be an encouraging proof-of-concept suggesting the use of barbed suture for intestinal anastomosis.
Footnotes
Disclosure Statement
No competing financial interests exist.