
Abstract
Abstract
Background:
The most efficient approach to diagnosis of acute appendicitis (AA) continues to be a challenge. We sought to determine diagnostic accuracy, sensitivity, and specificity of computed tomography (CT), ultrasonography, and laparoscopy and compared benefits and advantages in patients with suspected AA.
Patients and Methods:
A retrospective review of all patients who had laparoscopic surgery between January 2000 and December 2009 was conducted. Preoperative information, surgery results, and outcomes were compared.
Results:
Of 887 laparoscopic procedures performed for suspected AA, 254 (29%) patients had preoperative imaging: 171 CT scans and 83 ultrasound (US) scans. Overall, 754 patients underwent laparoscopic appendectomy (LA), and 133 underwent diagnostic laparoscopy (DL). DL was negative in 23 patients. The sensitivity of LA was higher than that of CT (98% versus 94%), whereas the specificity of LA was higher than that of CT and US in complicated appendicitis and in women. Complicated AA was significantly less common in patients who underwent laparoscopic surgery compared with patients evaluated by preoperative CT. Comparing the kappa value between the preoperative diagnosis by imaging and DL, a weak agreement was found (κ=0.234±0.057).
Conclusions:
Laparoscopy achieves early and accurate diagnosis of AA and can reduce the incidence of perforated appendicitis. Abdominal CT remains a valuable diagnostic tool. DL is useful in the early stages of the diagnostic work-up and avoids unnecessary exposure to radiation of the abdomen and pelvis in young women.
Introduction
A
Computer-aided diagnostic questionnaires, clinical scoring system (Alvarado), active observation, abdominal ultrasound (US), abdominal computed tomography (CT), and early laparoscopy have all been described as potential methods for improving diagnosis. The diagnostic accuracy of a US scan has been reported to range from 71% to 97%, whereas that of a CT scan has been reported to range from 83% to 98%.3,4 However, controversy still exists as to the role and benefit of imaging in the work-up for AA and as to clear indications for using these modalities. Diagnostic studies may cause additional delay in definitive management and increase operative risk.4,5 On the other hand, diagnostic laparoscopy (DL) in the acute abdomen offers rapid and accurate diagnosis and subsequent treatment of intraabdominal pathology. Nevertheless, DL and therapeutic laparoscopy are invasive procedures, and there is still controversy about whether this technique should be applied to all patients or reserved for patients in which any doubt still remains for the diagnosis of AA. 6
The purpose of this study was to evaluate benefits and clinical outcome and to compare the sensitivity, specificity, and diagnostic accuracy of US, CT, and laparoscopy in AA.
Patients and Methods
We reviewed the medical records of patients who underwent laparoscopic appendectomy (LA) for AA in our department at Soroka University Medical Center, Beer-Sheva, Israel, between January 2000 and December 2009. After we received the permission of the ethics committee, a list of patients was gathered from the operating room database. Data obtained included demographics, duration of disease before admission, time to surgery, body temperature, laboratory tests, imaging utilization prior to surgery, operative findings, pathology results, and surgery outcomes.
Patients were assessed initially by the on-call surgical team. In our service we do not use any scoring systems for diagnosis of AA. Preoperative laboratory tests were used as a part of routine investigation of abdominal pain in the emergency room (ER). All women who suffered from lower abdominal pain underwent a routine gynecological examination to exclude acute gynecological pathology. Patients with obvious clinical diagnosis of AA (local tenderness, guarding, fever, and leukocytosis) and high suspicion for AA (local tenderness, guarding, and no fever or leukocytosis) were considered for urgent laparoscopy. A flowchart of patients with right lower quadrant (RLQ) abdominal pain is presented in Figure 1. LA was performed in patients with AA found during surgery. Laparoscopy was considered diagnostic only when AA was not found and appendectomy was not done.
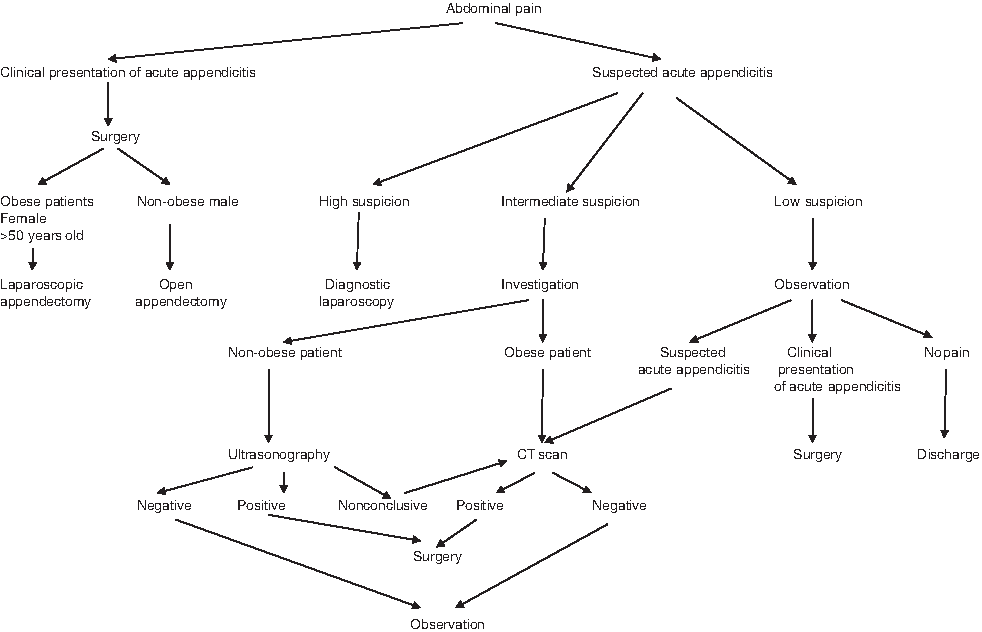
Flowchart of patients with abdominal pain. CT, computed tomography.
The decision for additional preoperative evaluation was made by the surgeon on call or senior surgeon in cases of insufficient clinical diagnosis at admission or during morning rounds. US was considered in nonobese patients in whom AA was suspected. CT scan was indicated in all other patients and in cases of inconclusive US. CT scan was performed using 1500 mL of oral contrast medium (2% diatrizoate meglumine [Gastrografin®; Bristol-Myers Squibb, Wallington, CT]) for bowel opacification 90–120 minutes prior to scanning. The scan was performed with the patient in the supine position, following an intravenous injection of 90 mL of iodinated contrast medium at a rate of 3 mL/second and a scan delay of approximately 50 seconds. Results of CT scans and ultrasonography were interpreted by a staff radiologist. Diagnosis of AA was made when a thickened appendiceal wall or pericecal or periappendicular inflammation with or without intraabdominal fluid was found. Patients with a nonvisualized appendix by CT scan were diagnosed as having no evidence of AA. An appendectomy was performed in all patients with a US or CT scan positive for AA. Patients who had persistent abdominal pain during a 24-hour observation were maintained in the ward on nothing peroral status without using antibiotics. In this group negative imaging for AA was an indication for DL. DL group included patients, in whom appendectomy was not performed.
Time to surgery was counted from admission to ER and surgery start. All patients were administered a single dose of intravenous metronidazole 500 mg and cefuroxime 750 mg preoperatively. In cases of perforated appendicitis antibiotics were continued for 3 or 5 days.
All procedures were performed by or under the guidance of the attending surgeon or chief resident. LA was performed via three ports. An infra- or supra-umbilical 11-mm port was inserted by either the closed (Veress needle) or open (Hasson) technique, and a 45° laparoscope was inserted to examine the abdomen. Two additional ports were inserted under direct vision in the right iliac fossa and either the left iliac fossa or above the pubis. The standard LA technique using bipolar coagulation for mobilization of mesoappendix and endoloop was used for closure of the appendiceal stump. The specimen was extracted inside the 10-mm trocar in the case of a thin appendix or through the one of the ports using a retrieval bag.
A diagnosis of AA was based solely on the pathological findings of the appendix. Complicated appendicitis was defined by the finding of a gangrenous or perforated appendix, as well as the presence of an intraabdominal abscess. Patients with a histologically normal appendix or patients with intraoperative findings of other intraabdominal pathologies were classified as “negative” appendectomy.
Postoperative complications were determined as infectious when postoperative fever, intraabdominal abscess or phlegmon, wound infection, or urinary tract infection was present after surgery.
Data were coded, stored in a Microsoft® (Redmond, WA) Office Excel file, and analyzed with SPSS version 17.0 software (SPSS, Inc., Chicago, IL). Data were first analyzed with descriptive statistics (distribution characteristics). Comparison of the groups was done with a Pearson chi-squared test and calculation of kappa for qualitative data and with a Fisher's exact test for dichotomic variables. Comparison of quantitative data was examined with parametric tests: t test and nonparametric (Mann–Whitney) test. Significance was set at a P value of <.05. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated in comparison with the pathological report (gold standard).
Results
During the study period, 887 laparoscopies for suspected AA were done: 133 DL and 754 LA; 254 (29%) patients underwent further preoperative imaging. Following sonographic diagnosis of AA in 83 patients, 20 DL and 63 LA procedures were performed. Twelve patients underwent CT after an inconclusive US and were included into the CT group. Twenty-five DLs and 146 LAs were performed according to positive CT scan. During the study period, there was an increase in preoperative imaging: from 15% in 2000 to 48% in 2009 (Fig. 2).
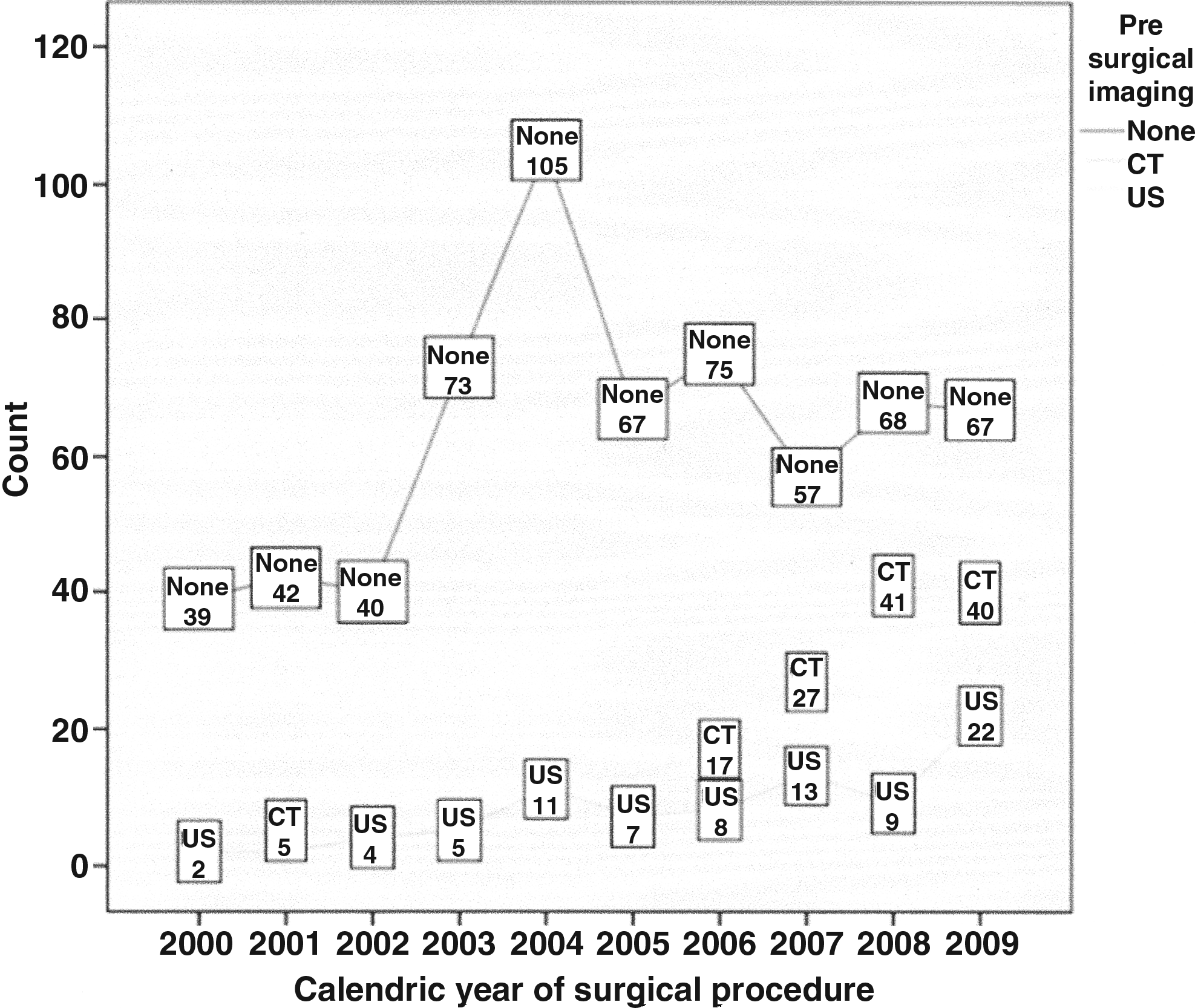
Use of additional imaging for diagnosis of acute appendicitis during the study period. CT, computed tomography; US, ultrasound.
Preoperative patient data are presented in Table 1. Laparoscopic surgery was more often used than CT in younger patients. US and DL were more common in women compared with men. Patients with prolonged abdominal symptoms and unknown diagnosis of abdominal pain were referred for additional imaging as opposed to those referred for laparoscopy. In addition, patients referred for laparoscopy had a shorter time before surgery. There was a significant difference between the neutrophil percentage at admission among all groups.
ASA, American Society of Anesthesiologists; CT, computed tomography; NR, no relevance; NS, not significant; SD, standard deviation; US, ultrasound; WBC, white blood cell.
Laparoscopy showed abdominal pathology in 864 (97.4%) patients. Overall, laparoscopy was “negative” for AA in 133 (15%) patients: 84 (63.2%) were gynecological, 26 (19.5%) had nongynecological pathology (mesenteric torsion, diverticulitis, mesenteric lymphadenitis, etc.), and 23 (17.3%) were without abdominal pathology. There were 87% females in the DL group.
Eighty-eight of 133 patients underwent DL without preoperative imaging; 20 had US and 25 had CT prior to surgery. In the US group 11 (55%) were considered to have normal imaging, 4 (20%) had AA, and 5 (25%) were suspected of having other nonappendiceal pathology. There were no intraabdominal findings on DL in 6 (55%) of 11 patients with normal US, whereas gynecological pathology was found in 5 (45%). Four patients with sonographically shown AA had gynecological problems on surgery. DL was normal in 1 patient and revealed gynecological pathology in 4 patients with US suspicion for other pathology.
In the CT group, 9 (36%) were considered normal imaging, 9 (36%) had other, nonappendiceal pathology, 6 (24%) were suspected of having AA owing to the enlarged diameter of the appendix between 8 and 10 mm, and 1 (4%) was suspected of having a parasitic infection inside the appendix. On DL, 5 of 6 (83.3%) patients with suspected AA on CT scan were found to suffer from gynecological and 1 (16.7%) from other nonappendiceal pathology. DL was normal in 5 (55.5%) of 9 patients with normal CT scan. Gynecological and nonappendiceal pathology was found during surgery in 3 (33.3%) and 1 (11.1%) patient, respectively. DL in 9 patients with nonappendiceal pathology showed gynecological problems in 4 (44.4%) and nonappendiceal pathology in 3 (33.3%) and was normal in 2 patients. There were no findings during surgery in the patient with suspected parasitic infection on CT scan.
There were 597 women (67%) in the current study with mean age of 36.3±15.8 years. Of these, 451 (75.5%) were in the fertile age group and underwent laparoscopic surgery: 89 (19.8%) DL and 362 (80.2%) LA. Intraabdominal pathology was found on laparoscopy in 404 patients: AA in 265 (65.6%) and gynecological and other pathology in 129 (31.9%) and 10 (2.5%), respectively. There were no findings during surgery in 47 (10.2%) of the patients. Pathology results of the specimen reported AA in 249 and other (carcinoid, parasites, etc.) in 7 patients. There was no acute inflammation of the appendix in 16 (6.0%) fertile-age women on pathology. Complicated appendicitis was diagnosed in 29 (11.6%) of all women suffering from AA in this group.
Analysis using imaging in this group showed that 344 (76.3%) patients underwent surgery without imaging prior to surgery. Of these, 284 (82.6%) patients underwent LA, and 60 (17.4%) underwent DL. Intraabdominal findings during surgery included AA in 204 (59.5%), gynecological problems in 100 (29.2%), and other pathology in 6 (1.7%) patients. Laparoscopy was normal in 33 (9.6%) women. Pathological investigation approved AA in 198 (97%) cases. Complicated appendicitis was found in 25 (12.2%) of the patients without imaging.
One hundred seven fertile-age women underwent imaging before surgery: 57 (53%) abdominal US scans and 50 CT scans (10 patients had both because of an inconclusive US). Sonographic diagnosis of AA was done in 28 women. Of these, 21 (75%) had AA, 5 had gynecological pathology, 1 had other pathology, and 1 had normal laparoscopy. Twenty-nine women had normal US before surgery; however, laparoscopy found AA in 10, gynecological problems in 11, and no findings in 8 (27.5%). AA was considered on CT scan in 29 women. Surgery showed AA in 24 (82.7%) women, gynecological pathology in 9 women, and no findings in 1 woman. During surgery of 21 patients with normal CT scan, 6 had AA, 9 had gynecological pathology, and 2 had other pathology. Only 4 (19%) women of this subgroup had a true-negative CT scan.
Sensitivity, specificity, PPV, and NPV of US, CT, and LA are presented in Table 2. The sensitivity of LA was found to be higher than that of a CT scan (98% versus 94%). It was higher in younger patients (<60 years old) compared with CT and US (98% versus 87% and 64%, respectively). In older patients (>60 years old), a high sensitivity was found (98%–100%) in all methods, with no difference among the groups.
CT, computed tomography; NPV, negative predictive value; PPV, positive predictive value; US, ultrasound; NR, no relevance.
The specificity of LA was higher than that of CT or US in complicated appendicitis (100% versus 13% and 37%, respectively) and in women (95% versus 72% and 63%, respectively). It should be noted that specificity and sensitivity were identical for the DL and regular laparoscopy groups.
The NPV of patients who underwent LA was higher in all subgroups except that of uncomplicated appendicitis. The PPV for LA was 100%, as opposed to 25% for CT and 23% for US.
Surgical outcomes are presented in Table 3. Incidence of complicated appendicitis was significantly less in patients who underwent laparoscopy, compared with those who had preoperative CT. So it is not surprising that operation time, antibiotics duration, and length of hospitalization were significantly shorter in patients who underwent laparoscopy than in those who underwent CT.
CT, computed tomography; SD, standard deviation; US, ultrasound.
Kappa values for the test reliability were calculated for the laparoscopic versus imaging groups. Kappa was 0.325±0.071 (low–medium agreement) when a comparison was made between the surgeon's preoperative assessment and the preoperative diagnosis according to imaging results in the laparoscopic group. In the DL group, the kappa value was 0.282±0.109 (weak agreement). Laparoscopic surgical diagnosis versus preoperative diagnosis for the imaging results found a kappa value of 0.234±0.057 (weak agreement) between tests.
Discussion
Prompt and accurate diagnosis reduces the morbidity and mortality of AA. About 33% of patients with AA have atypical presentation. 2 During the past decade, dramatic changes in the diagnosis and management of AA have occurred.
Appropriateness criteria of the American College of Radiology–recommended ultrasonography as a screening test for most patients with suspected AA. 7 US is noninvasive, safe for use in children and pregnant patients, and able to make a particular contribution in gynecological problems. In our study we found the lowest sensitivity of US to be 74% and specificity to be 39% in diagnosing AA with lowest NPV. The sensitivity was lower than CT and clinical presentation, and specificity was nearly the same as clinical judgment. Despite reports of high accuracy, up to 93% with an experienced US operator, the high rate of false-negative results is not a clear indication for releasing a patient when the clinical picture is unclear. 8 Jones 9 recommended using US as a preliminary test, especially in females of reproductive age, when the rest of the tests are nonconclusive, and there is reasonable suspicion for other intrapelvic pathologies (non-AA). This study found a high NPV in women (66%) and young patients (60%), but this value is not high enough to recommend releasing a patient. Davies 10 found that diagnosing AA with US is no better than a clinical diagnosis by the surgeon. In addition, one must take into account the limitations of US in obese patients, where the penetrance of the US of the abdominal wall is low. Otherwise, atypical positioning of the appendix may cause a false-negative result on sonography. On the other hand, incorrect identification of the terminal ileum as an enlarged appendix may cause overdiagnosis of AA when US is used.
The use of CT in this clinical decision-making process has been proved to lower the rate of negative appendectomy—an appendectomy of a macroscopically normal appendix.11,12 CT is a more precise and accurate tool than US in diagnosing AA. 13 The helical CT has high sensitivity, specificity, and diagnostic accuracy (87%–100%, 83%–99%, and 94%–98%, respectively).3,14,15 Comparison of studies under experimental clinical protocols and studies in the community showed that studies under clinical protocols had higher sensitivity (98%) 3 compared with community studies, which had a lower sensitivity (as low as 83%).4,16 Our study found a sensitivity of 87%–98% in all subgroups; this strengthens existing data about the diagnostic value of CT in experimental protocols.
In our study CT was done in cases where the diagnosis was unclear. In the majority of patients who underwent CT, the length of disease before hospitalization was significantly longer, which can be explained by the atypical presentation of AA. There are investigators who recommend CT as part of the routine process in a patient with RLQ abdominal pain and suspected AA, in order to improve treatment and efficiently use hospital resources. On the other hand, routine use of CT in assessing patients with suspected AA exposes them to unnecessary radiation and contrast material, which may endanger the patient, and delays surgery (definitive therapy), as well as adding to health expenditure. In a review by Terasawa et al., 17 CT was shown to be preferable to US in patients with an atypical clinical presentation that still indicates AA. Other recent studies have shown the advantages of a selective approach to use of CT in suspected AA patients.3,18
Some researchers have postulated that CT is more effective in diagnosing AA in women of reproductive age. This subgroup has a higher negative appendectomy rate, up to 40%. 19 This can probably be attributed to the high rate of pelvic gynecological pathologies, which often mimic the symptoms of AA. This study examined the advantages of laparoscopy over CT and US in women, by analyzing specificity and NPV. In the women's group there was higher sensitivity in the laparoscopy group compared with CT and US (95% versus 72% and 63%, respectively) and NPV of 84% compared with 74% and 66%, respectively. It can be concluded that CT is not reliable enough and is less efficient than laparoscopy in women. In most cases, the final diagnosis was of another intrapelvic pathology.
The optimal protocol of CT for the diagnosis of AA is still debated. Lane et al. 20 recommended the use of helical CT, without contrast, as the first choice. Rao et al. 3 and Hershko et al. 21 reported notable results with appendiceal CT and rectal contrast. The use of rectal contrast alone (compared with triple contrast) led to decreased delay until definitive surgery, decrease in perforations, and contrast use morbidity, without undermining diagnosis.3,21,22 However, intravenous and oral contrast allows evaluation of other intraabdominal pathologies and can spare later assessment. Soroka Medical Center uses oral and intravenous contrast material, with good results using the above criteria.
Erroneous interpretation of CT can lead to unnecessary surgery or delay in definitive therapy (such as in AA). Most CT scans in the study were interpreted by an on-call radiologist (during the night shift) and were revised by a senior radiologist the next morning. Only in 1 case (1%) did the senior radiologist change the diagnosis on revision. Imprecision in diagnosis may occur when inexperienced staff members do the preliminary interpretation.12,23 However, Ruchman et al. 24 described a discordance of 2.6% when interpretations of on-call residents and seniors were compared. Ceydeli et al. 23 argued that in order to decrease disparity, CT scans interpreted by on-call physicians and deemed negative should be reexamined by a senior radiologist. Using new computing systems, a senior radiologist can interpret CT scans from home and so increase the diagnostic value, sensitivity, and specificity. Good teamwork between the on-call surgeon and resident will improve the value of the CT because clinical data can improve understanding and interpretation of the test.
The Soroka Medical Center ER is divided into surgical and internal medicine departments. Most patients with an acute abdominal pain are referred to the surgical ER. This allows quick identification and evaluation of patients with suspected AA and reduces unnecessary tests when the clinical picture clearly fits AA. However, surgical staff inexperience may cause overuse of imaging. Another physical exam by a chief resident or senior surgeon can reduce the number of unnecessary imaging tests. Terasawa et al. 17 recommended immediate intraoperative evaluation of patients with typical presentation of AA. Morris et al. 25 additionally recommended evaluation by experienced surgical staff before ordering CT exams for suspected AA and reducing superfluous CT scans. This study did not gather data on senior surgeon exams before CT, so we cannot improve knowledge about the value of this exam in these cases.
Diagnosing AA in the first stages is difficult when the appendix is retrocecal, confined, or perforated. Diagnosis of complicated AA is relatively simple when the patient has peritonitis, high fever, or significant leukocytosis, but patients without these severe signs may only be diagnosed intraoperatively. CT findings such as free air, periappendicular collection, and severe periappendicular inflammation are important in predicting complicated AA. Study results show that patients with extended disease before admission have a higher prevalence of complicated AA. Presurgical imaging and preparation for the test delayed surgery in the study cases. Theoretically, surgery delay increases the risk of a perforated appendix. Temple et al. 26 concluded that most perforated appendix cases developed because of late presentation. Eldar et al. 27 found that the minority of perforations occurred in-hospital and that a perforated appendix can be recognized clinically. Musunuru et al. 14 found that CT scans have a negative effect in delaying surgery and have the potential for a high perforation rate. On the other hand, Frei et al. 28 concluded that the increasing use of CT decreases delays in therapy and the complication rate.
In addition, the study found an increase in complicated AA and longer hospitalization because of intravenous antibiotic use. Despite the high rate of complicated AA cases in patients who underwent CT, there was no difference in morbidity in this group.
Recently, small numbers of studies have been published evaluating the efficacy of laparoscopy and imaging in the diagnosis of AA. 29 Despite this, it is difficult to establish a precise diagnosis of AA without invasive techniques. In comparison with preoperative imaging or the watchful waiting approach, laparoscopy can give a precise diagnosis in more patients. It seems that laparoscopy to evaluate the acute abdomen is safe, for whatever organ is afflicted, adhesions, or severity of the peritonitis. Recent studies have shown that DL for suspected AA can reduce the rate of unnecessary laparotomies. 30 in't Hof et al. 15 concluded that laparoscopy is the gold standard for diagnosis of patients with suspected AA. AA can be diagnosed laparoscopically in early stages of the disease and so lower the threshold for appendectomy in AA. 31 Another advantage of laparoscopy is the ability to recognize situations such as cecal carcinoma, cecal or sigmoidal diverticulitis, Meckel's diverticulitis, or inflamed duodenal ulcer, which can present similarly to AA; these conditions can be diagnosed and treated in the same procedure. Early diagnosis and therapy with laparoscopy save money and resources such as imaging, as well as excess morbidity in more advanced disease. On the other hand, regular use of laparoscopy in suspected AA patients can increase the cost of hospitalization and the rate of unnecessary appendectomies. Our study found a PPV for laparoscopy of 85%–100% in different subsets of populations, where older adults had the lowest predictive value. In light of these data, the rate of unnecessary appendectomies is relatively negligible.
This study examined data of DL. Preoperative data show that the procedure was mostly carried out in women, younger patients, and patients with a lengthy course before admission. It can be concluded based on this that the decision for laparoscopy was based on atypical clinical presentation and nondiagnostic imaging, but with a high suspicion of intraabdominal or intrapelvic pathology. In addition, one can see that the time elapsed until entering surgery (DL) was long, similar to the CT and US groups, which highlights the need for a highly accurate diagnostic test for an unclear clinical picture. In light of the difficulty in differentiating intrapelvic pathologies and AA in women, one can claim that in the subset of women of reproductive age, this test is valuable. This study did find that out of 110 pathological results in DL, 84 were gynecological pathologies. Garbarino and Shimi 32 found that routine use of DL in women of this age significantly reduced the negative appendectomy rate to 5%, compared with selective use of DL in this group of patients (with typical presentation of RLQ), which reduced the negative appendectomy rate to 31% (insignificant). Lim et al. 33 found that use of DL in women of reproductive age, with clinical presentation similar to that of this study group, changed the therapeutic course in 31% of cases (following a non-AA pathology) and that the diagnostic accuracy of this method, compared with other gynecological imaging methods, was higher. The women's group had a particularly high specificity (95%) for laparoscopy compared with imaging groups (72% for CT, 63% for US), so the method's ability to find “healthy” patients (without AA) is high, which shows itself in the NPV in this group. Another corroborator for this claim is the kappa value for DL, which shows that preoperative diagnosis and intraoperative diagnosis have a weak agreement between groups, and in light of specificity data it seems that DL is the superior of the two in women.
These data strengthen our argument in preferring laparoscopy of women of reproductive age. The diagnostic difficulty in this group (atypical presentation and similar gynecological pathologies), the time spent in evaluation before definitive therapy, and the ability to give a precise diagnosis and efficient therapy, whether the final diagnosis is AA or a gynecological pathology, require a gynecological surgeon for continued treatment.
Study Limitations
One limitation in the present study is that it is retrospective, which makes it difficult to evaluate the rationale behind deciding on one imaging technique or another, and the real-time interpretation and diagnosis of the radiology team in examining the imaging results. For example, there are no data of patients with CT evidence of AA who were released without surgical intervention because of changes in their clinical presentation, although it is known that there were such patients during the study period. Although prospective studies are significant in evidence-based medicine, their realization in practice is difficult. In considering a prospective study, one must remember that not every patient with RLQ abdominal pain and negative imaging will agree to undergo appendectomy just to prove a clinical argument, a problem we contended with in this study as well, retrospectively examining these patients.
Overlap between the study groups was another limitation, which results from the clinical nature of the study, and the wish to give the patients optimal care. One group was the imaging group, and the second group was a laparoscopy group, which added a diagnostic value to the therapeutic value. This fact hampers a direct comparison between the groups, without overlap. For example, a patient who underwent US imaging without conclusive evidence and then underwent CT would be placed in the CT group. This same patient, if a CT confirmed AA, may have undergone LA and would then appear in the laparoscopy study group. It should be emphasized that overlap is necessary for data in this study; because of this, patients did not undergo appendectomy. The study groups' size was the main tool in dealing with this limitation, so that comparison significance could be achieved, despite the overlap.
A third limitation was the inability to compare against the gold standard in DL. Because the gold standard is the pathological tissue exam, in addition to “diagnostic” laparoscopy being, by definition, without tissue excision, sensitivity, specificity, NPV, and PPV could not be calculated for this group. This limitation prevented us from truly discussing the diagnostic accuracy of the test. One way to contend with this limitation is to argue that the first stages of the LA are essentially equivalent to DL, and so the data for the laparoscopy group can be projected on the DL group in specificity and NPV. To strengthen this argument, we calculated a kappa value between different study groups for diagnosis agreement. The value expresses the probability that agreement between different methods is not incidental, so that a kappa value smaller than 0.4 expresses weak agreement. Use of the kappa value for preoperative and intraoperative diagnosis strengthened this study's hypothesis concerning the disagreement between groups (tests), and their incorporation with values of the diagnostic accuracy for the LA led us to our conclusions. A third option for analysis was to examine whether “healthy” patients on DL were readmitted the following month, assuming that a missed appendicitis would present severely not long following release from hospital. Data on readmission in the 30 days were collected but, owing to the small number of patients and limited statistical strength, was not analyzed.
Conclusions
Use of laparoscopy allows early precise diagnosis of AA resulting by decreasing the rate of appendical perforations. Clinical judgment and proper use and timing of imaging still have an important role in AA diagnosis. Use of abdominal CT is efficient in diagnosing AA in most cases (except complicated AA), but it delays surgery and elevates the rate of complicated AA. Early referral of patients to CT in the ER can prevent AA complications and reduce hospitalization length. These data strengthen the routine use of early DL in the diagnostic process and the avoidance of abdominal and pelvic radiation in young women.
Footnotes
Disclosure Statement
No competing financial interests exist.