
Abstract
Abstract
Objectives:
To report our preliminary experience and to assess the learning curve for laparoendoscopic single-site retroperitoneal pyeloplasty (LESS-RP) for ureteropelvic junction obstruction (UPJO).
Patients and Methods:
From July 2010 to February 2012, LESS-RP was performed in 27 patients affected with UPJO by a single surgeon. A homemade single-access platform and both conventional and prebent instruments were applied. Patient characteristics and perioperative outcomes were analyzed. The cumulative sum (CUSUM) method was used to evaluate the learning curve.
Results:
The LESS-RP was successfully accomplished in all 27 patients. The mean operative time (OT) was 175.9±22.5 minutes, and the mean estimated blood loss was 83.3±27.1 mL. We used the OT as a proxy to assess the learning curve. The CUSUM learning curve can be divided into two distinct phases: the initial 12 cases and the last 15 cases. There were significant differences in the mean OT (195.6 minutes versus 159.1 minutes, P<.001) and mean estimated blood loss (97.2 mL versus 72.2 mL, P=.014) between the two phases. The two phases did not differ in other parameters.
Conclusions:
LESS-RP is a safe and feasible procedure. The learning curve of a single surgeon suggests that the initial learning phase for LESS-RP can be completed after approximately 12 cases.
Introduction
For a new technique to be widely adopted, it is important to document the reproducibility of the technique and associated learning curve. The cumulative sum (CUSUM) can transform raw data into running total data deviations from their group means, which allows investigators to continuously monitor and rapidly detect the changes in performance and to judge whether the performance is acceptable or unacceptable. 11 Since it was first introduced to investigate the learning curve for human surgical procedures in the 1970s, 12 the CUSUM method has been applied to various operations.13,14
In this study, we reported our initial experience on LESS-RP and quantitatively assessed the learning curve faced by an experienced laparoscopic surgeon but an early adopter of the LESS-RP using the CUSUM technique.
Patients and Methods
We obtained approval for this study from the ethics committee at Central South University (Changsha, China). Also, we obtained informed consent from all participants in our study. The informed consent was written and specified in the operative consent. Between July 2010 and February 2012, 27 consecutive patients received LESS-RP performed by a single experienced laparoscopic surgeon at Xiangya Hospital. The surgeon already had experience in advanced laparoscopic procedures. However, he was a beginner in LESS surgery and had no experience with LESS-RP. All patients were subject to a preoperative evaluation, including renal ultrasonography, diuretic renography, intravenous urography, or computed tomography. The indications for surgery included an increasing degree of hydronephrosis, an obstructive pattern on diuretic renal scan, impaired renal function, and symptoms such as recurrent urinary tract infection and flank pain. No patient in this study had received renal surgery previously. The clinical data of the patients included were prospectively recorded.
Surgical procedures
The patient was placed in the lateral decubitus position after induction with general endotracheal anesthesia. A 2.5–3-cm transverse skin incision was made along the lower margin of the 12th rib in the midaxillary line. A hemostatic forceps was then used to divide the fascia lumbodorsalis, and a finger was inserted to separate the retroperitoneal fat and the retroperitoneal space. The creation of a working space was performed by placing a homemade balloon dilator with 600 mL of air infused for 5 minutes in the retroperitoneum. A size 7 powder-free surgical glove and an F14 silicone tube were used to construct the homemade single-port device. The wrist of the surgical glove was fixed to the ring made by the silicone tube with the silk suture. The fingers of the surgical glove were cut, and two 10-mm trocars, one 5-mm trocar, an intake pipe, and an exhaust pipe were inserted, one per finger. The ring was inserted into the retroperitoneal incision site (Fig. 1). Then a CO2 insufflation was performed at a pressure of 12–14 mm Hg. A 30° rigid laparoscope was inserted through the 10-mm trocar. The conventional and prebent instruments were inserted through the other two trocars. The prebent instruments (e.g., prebent laparoscopic forceps, prebent suction tube) and conventional straight ultrasonic scalpel and bipolar forceps were used to perform the procedure. The retroperitoneal fat tissue was dissected to reveal Gerota's fascia, which was then incised longitudinally close to the psoas magnum muscle. The lower pole of the kidney was identified. Surrounding fatty and connective tissue was bluntly dissected from the pelvis and upper ureter using the tip of the suction tube. The location of the UPJO could be identified after the dilated renal pelvis and the upper ureter were mobilized, and the cause of UPJO was evaluated.

Our homemade single-access device.
A standard Anderson–Hynes dismembered pyeloplasty was performed. The stenotic segment of the UPJO was cut down, and the dilated renal pelvis was trimmed to a trumpet shape. The proximal ureter was spatulated with a 1.0-cm longitudinal incision on its lateral aspect. The posterior pelvis–ureter anastomosis was performed with 4-0 absorbable monofilament using a running suture. Before a similar suture was performed on the anterior wall of the anastomosis, a double-J stent was inserted in an antegrade fashion, and the proximal end of the stent was placed in the renal pelvis. After the anastomosis was completed, a suction drain was placed through the incision. The Foley catheter was removed on postoperative Day 2. The drain was subsequently removed when the drainage was <10 mL/24 hours after Foley catheter removal. The double-J stent was removed 4 weeks postoperatively by a cystoscope.
The demographic data, operative time (OT), estimated blood loss, length of stay, rate of conversion, degree of postoperative pain, and complications were recorded. The OT was calculated as the time from the first skin incision to the final closure of the skin incision. The visual analog pain scale (VAPS) score at 24 hours after the operation and at discharge was used to assess the degree of postoperative pain. The VAPS score ranged from 1 to 10 points (where 1=minimal pain to 10=worst pain). The dose of analgesic requirement from recovery room through to discharge was converted to morphine equivalents. Patients were followed up for at least 6 months. Success was defined as improvement or stabilization in function and adequate renal excretion (t½<20 minutes) on diuretic renal scan, along with the complete resolution of presenting symptoms.
CUSUM analysis
We quantitatively assessed the learning curve using the CUSUM technique as reported in the literature. 11 The CUSUM can be performed recursively because CUSUM is the running total of differences between the individual data points and the mean of all data points. The CUSUM technique was applied to assess the OT for all the 27 cases.
The cases were chronologically ranked. The CUSUM of the first case was defined as the difference between the OT of the first case and the mean OT of all the 27 cases. The second case's CUSUM was the CUSUM of the first case added to the difference between the OT of the second case and the mean OT of all the case. Similarly, the CUSUM values of the remaining cases were calculated continuously.
Statistical analyses
Statistical analysis was performed with the independent-samples t test, Mann–Whitney U test, or Pearson's chi-squared test, where appropriate. A difference was considered significant at P<.05 in all tests. Statistical analyses were performed with SPSS version 19.0 software (SPSS Inc., Chicago, IL).
Results
All patients underwent successful LESS-RP for UPJO. Patient demographics and perioperative outcomes are summarized in Table 1. Mean age of the patients was 36.8±13.4 years, and of the 11 women and 16 men, 17 presented with UPJO on the left side versus 10 on the right side. The mean body mass index was 24.1±3.4 kg/m2. The mean OT was 175.9±22.5 minutes, and the mean estimated blood loss during operation was 83.3±27.1 mL. No intraoperative complications or blood transfusions occurred in the 27 procedures. The mean postoperative hospital stay was 3.7±0.9 days. The mean VAPS scores were 4.3±1.7 and 1.6±1.4 at 24 hours after the operation and at discharge, respectively. The mean morphine equivalent requirement was 8.8±6.2 mg. Three minor postoperative complications (Clavien-Dindo classification for surgical complications) were identified in 3 cases. 15 Gross hematuria occurred in 1 patient (Case 19) and was resolved conservatively, but 2 more days were needed for the hospital stay. Two patients (Case 9 and Case 23) developed a urine leakage, which was managed successfully through extending the drainage time to 7 and 9 days, respectively. No major postoperative complications were observed.
VAPS, visual analog pain scale.
At the first time of follow-up, all preoperatively symptomatic patients reported a complete resolution of symptoms. There was only one small single scar left on the waist (Fig. 2). Average follow-up was 12 months (range, 6–24 months). Two patients (Case 3 and Case 17) were regarded as having failed procedures at follow up. They presented recurrent symptoms with t½ >20 minutes on the diuretic renal scan within 6 months. These patients were both managed successfully by open pyeloplasty. The overall success rate was 92.6%.

Postoperative appearance at 3 months following laparoendoscopic single-site retroperitoneal pyeloplasty.
The original OTs for the 27 cases are shown in Figure 3. The CUSUM learning curve is demonstrated in Figure 4 and was best fitted and defined as a cubic polynomial with the following equation: CUSUM OT (in minutes)=−40.16+(51.05×case number)−(2.87×case number2)+(0.04×case number3), with an R value of 0.95. The curve can be divided to two different phases: phase 1 (Case 1–Case 12) and phase 2 (Case 13–Case 27). Patient characteristics and perioperative results were compared between the two phases. There was no significant difference in any of the determinants between the two phases. The OT significantly differed between phase 1 and phase 2 (195.6 versus 159.1 minutes, P<.001). There was a significant difference between the two phases in terms of estimated blood loss (97.2 mL versus 72.7 mL, P=.014). However, mean postoperative hospital stay, mean VAPS score, mean dose of analgesic requirement, intraoperative and postoperative complication rates, and success rate were also comparable and were almost identical between the two phases (Table 1).

Operative time versus case number.
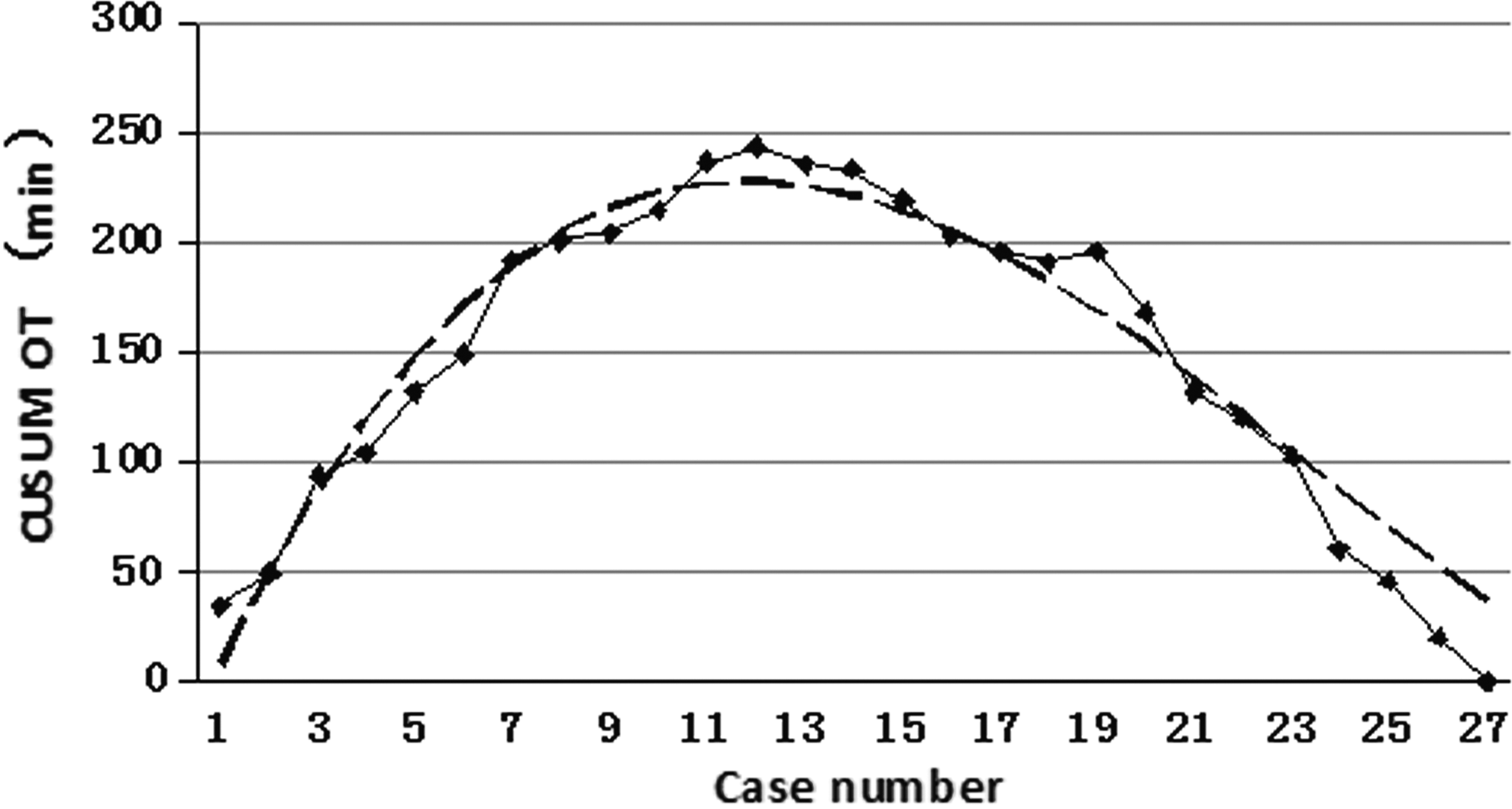
Cumulative sum for operative time (CUSUM OT) plotted against case number (solid line). The dashed line represents the curve of best fit for the plot, a cubic polynomial with the equation CUSUM OT=−40.159+(51.050×n)−(2.874×n2)+(0.040×n3) (where n is the case number), R=0.951.
Discussion
With the development of the technology over the past few decades, laparoscopic surgery has been widely applied to treat various surgical disorders with comparable efficacy and reduced morbidity relative to their open surgical counterparts. In order to continually improve on the morbidity, convalescence, and cosmetic results of laparoscopic surgery, more and more surgeons have attempted to pursue LESS surgery.6,7
Many urologic LESS procedures, including nephrectomy, ureterolithotomy, adrenalectomy, and pyeloplasty, have been proved to be feasible and safe. Because of the lack of an extraction incision, limited dissection, and improvement of cosmesis, pyeloplasty seems ideally suited for LESS surgery. 8 Since the first clinical experience of dismembered pyeloplasty with LESS was reported by Desai et al. 9 in 2008, there have been several series in the published literature demonstrating the feasibility and efficacy of LESS pyeloplasty in both children and adults.6,7,16 LESS pyeloplasty can be performed through a transperitoneal or retroperitoneal approach. Best et al. 17 suggested that a skilled laparoscopic surgeon could make the transition from conventional laparoscopic pyeloplasty to LESS pyeloplasty and achieve a similar complication rate relatively quickly. Tugcu et al. 18 completed 14 LESS pyeloplasties and predicted this technique would take the place of the standard laparoscopic pyeloplasty. Recently, Chen et al. 19 demonstrated that LESS-RP was a feasible and safe alternative for correcting UPJO in experienced hands.
According to conventional laparoscopic pyeloplasty experience, the transperitoneal approach provides better working space and better cosmetic effect but may need considerable mobilization and retraction of the bowel to reach the ureteropelvic junction, which increases the risk of bowel injuries and postoperative ileus. 20 Conversely, retroperitoneoscopy has a limited working space that may increase the difficulty of reconstruction but offers a shorter and more direct access to the UPJO, and there is no violation of the peritoneal cavity. We prefer LESS-RP because we have performed numerous cases of retroperitoneal laparoscopic surgery and have accumulated extensive experience with the surgical technique.
To our knowledge, this is the first report to demonstrate the learning curve of LESS-RP. The learning curve for surgery is represented as the number of cases required for a surgeon to perform a specific procedure to achieve a steady state in terms of OT and outcomes. OT can be used to assess the learning curve when the baseline characteristics were similar.21,22 Previous studies usually performed their analysis based on chronological cases split into predefined segments to investigate the learning curve for a specific procedure. Relatively speaking, CUSUM is considered to be more sensitive and objective to show the change in surgical performance with a binary outcome. 11 We adopted the CUSUM method to demonstrate the learning curve for LESS-RP performed by a single surgeon experienced in advanced conventional retroperitoneal laparoscopic surgeries but not in LESS-RP. When the initial 12 cases were compared with the last 15 cases, no statistical differences were observed in terms of clinical characteristics or outcomes except for the OT and estimated blood loss. When we used OT as a proxy for technical facility, we were able to delineate a learning curve of approximately 12 cases because the mean OT for the first 12 cases was 195.6 minutes, but it fell to 159.1 minutes in the next phase. The initial 12 cases constituted the initial phase of the learning curve in which OT decreased obviously. During this phase the surgeon could adapt to new instruments and spatial perception, gradually grasping the essentials of the new technique. This first phase of the learning curve seemed short and steep, which correlated with rapid learning and could be attributed to the surgeon's abundant experience of conventional retroperitoneal laparoscopic surgeries. The last 15 cases constituted the mastery phase of the learning curve, with a significant reduction in OT. This phase might indicate that a sophisticated operation skill had been developed.
Because the operative rules and visualization of the surgical field are not different between our LESS-RP and conventional laparoscopic retroperitoneal pyeloplasty (CL-RP), the learning curve of LESS-RP largely represents the process of understanding the spatial restriction caused by the close proximity of the instruments and the camera. The parallel insertion of conventional instruments results in the lack of triangulation. At the beginning, it is common that instruments clash against each other and the laparoscope. Intracorporeal suturing is the most difficult part of laparoscopic pyeloplasty. This task becomes even more challenging in LESS-RP because of the parallel insertion of instruments. We completed knot-tying using a prebent laparoscopic forceps to reduce the difficulty after suturing with the conventional laparoscopic needle holder. In addition, the performance of LESS requires ambidexterity of the surgeon because of the frequent crossing of the instruments' shafts at the entry point of the multiport. The adoption of prebent instruments, which have an angled and rigid shaft, may provide triangulation and decrease the instrument crossing. The surgeon holds the conventional instruments in the right hand and the prebent instruments in the left hand. In this way, the surgeon not only can create triangulation, but also can adapt to the LESS platform as soon as possible because the surgeon is right-handed and depends mainly on the right hand to complete specific procedures. Thus, to perform LESS-RP proficiently, the surgeon has to adapt to the lack of triangulation, the crossing of instruments, and the crowding of instruments outside the port and in the operative field. According to our experience, it is not very difficult to overcome these challenges for an experienced urological laparoscopic surgeon. In our present study, all patients underwent successful LESS-RP, and no intraoperative complications occurred in the 27 procedures. The postoperative complication rate was 11.1%, which was similar to the complication rates for standard laparoscopic pyeloplasty, which range from 12.9% to 22.5% as cited in the literature.23–25 After a mean follow-up period of 12 months, our success rate was 92.6%, whereas dismembered pyeloplasty is typically associated with a 90%–96% success rate.20,26,27 These data illustrate that, for a surgeon proficient with CL-RP, the LESS-RP is a safe and easily reproducible procedure even at the beginning stage, and the learning curve begins near proficiency. After performing only about 12 cases, the surgeon can achieve a stable phase with acceptable outcomes.
Calvert et al. 28 suggested 30 cases were required to complete the learning curve during the transition from open pyeloplasty to standard laparoscopic pyeloplasty. Our study seems to demonstrate that the transition from CL-RP to LESS-RP is easier than that from open to standard laparoscopic pyeloplasty. Similarly, some previous articles speculated on a short learning curve for the transition from standard laparoscopic surgery to LESS. Park et al. 22 reported a case series of 19 patients who underwent LESS radical nephrectomy. They found that the OT was reduced with experience and reached statistical significance within the initial 13 cases and suggested this might be reflective of the learning curve. Best et al. 17 adopted the complication rate to assess their learning curve of LESS pyeloplasty. They noted the frequency of complications decreased significantly over time and resembled that of conventional laparoscopic pyeloplasty after 10 cases.
The main limitation of this study is that the learning curve described is specific to only one surgeon proficient with CL-RP, with a relatively small sample size of 27 patients, limiting the generalizability of the results. It is expected that any individual surgeon's learning curve will vary depending on initial training and previous experience with different laparoscopic procedures. The learning curve might be longer for surgeons who are not experienced in CL-RP or do not possess skills in advanced laparoscopic surgeries.
Moreover, no comparison was performed between LESS-RP and CL-RP. Further studies are expected to better define the benefits of LESS-RP over CL-RP.
LESS-RP is technically demanding. However, for a surgeon proficient with conventional laparoscopic retroperitoneal procedures, LESS-RP is a safe and feasible procedure. The present study, using CUSUM analysis, suggests that the initial learning phase for LESS-RP can be completed after approximately 12 cases.
Footnotes
Disclosure Statement
No competing financial interests exist.