
Abstract
Abstract
Objective:
To evaluate the feasibility of and indication for laparoscopic methods for neonates with congenital duodenal obstruction.
Patients and Methods:
From September 2009 to October 2012, 40 newborns with duodenal obstruction underwent exploratory laparoscopy. With a lower-pressure pneumoperitoneum of 6–8 mm Hg and a suspending suture for the right liver elevator, the procedure was performed using four trocars 3–5 mm in diameter. Under laparoscopic vision, the causes of duodenal obstruction were diagnosed, and then the operation methods were determined by the type of obstruction.
Results:
Of the 40 cases, 4 were duodenal atresia (type II), 8 were duodenal stenosis, 8 were annular pancreas, and 20 were congenital intestinal malrotation. For the cases with duodenal diaphragmatic stenosis a partial excision of the diaphragm was performed after longitudinal incision of the anterior part of the duodenum followed laparoscopically by a transverse suture. For the cases with duodenal atresia (type II) and annular pancreas, a duodenal diamond anastomosis was successfully carried out through a laparoscopic approach. Ladd's operational method was performed in the cases with congenital intestinal malrotation. Feedings were started on postoperative Day 3–7, without abdominal distention and vomiting, and discharge from the the hospital was on postoperative Day 9–14.
Conclusions:
Congenital duodenal obstruction is a common malformation in neonates. The laparoscopic procedure is an important method of diagnosing, and correct operational methods are the key to improve the therapeutic effect in the treatment of congenital duodenal obstruction. The laparoscope has the value of a small incision, microinvasion, and better recovery in diagnosis and treatment for congenital duodenal obstruction. The laparoscopic methods can be performed in neonates safely and are appropriate for a full-term newborn with tolerance to CO2 pneumoperitoneum.
Introduction
The aim of this report is to describe our initial experiences with the laparoscopic approach for correction of neonates with duodenal obstructions.
Patients and Methods
This study involved a retrospective review of 40 neonates with congenital duodenal obstruction managed by a laparoscope-assisted approach from September 2009 until October 2012 at our hospital. The 40 cases were explored laparoscopically and operated on by a laparoscope-assisted procedure.
Laparoscopic technique
After initial stabilization and investigation, the laparoscopic approaches were discussed with the patients' parents, and formal consent was obtained for laparoscopy-assisted surgery with the patient under general anesthesia. The patients were placed supine on the table, the display was placed on the side of the head, and a nasogastric tube and urethral catheter were inserted. A 5-mm port was placed at the umbilicus for a 30° laparoscope, and CO2 pneumoperitoneum with a pressure of 6–8 mm Hg and a flow of 4–6 L/minute was established. The second and third ports were inserted, respectively, at the right lower and upper site of the abdomen just lateral to the edge of the rectus abdominis muscle. An extra port could be placed in the left upper quadrant to help in the operation (Fig. 1). A percutaneous suture introduced just below the xiphoid process was used to snare the round ligaments and retract the liver to achieve adequate exposure.

Port placement demonstrated as for the minimally invasive surgery cases. Gray arrow, laparoscope; black arrow, working port; white arrow, port for assistance.
In cases with duodenal diaphragmatic stenosis, a partial excision of the diaphragm was performed after longitudinal incision of the anterior part of the duodenum followed laparoscopically by a transverse suture closure (Fig. 2).
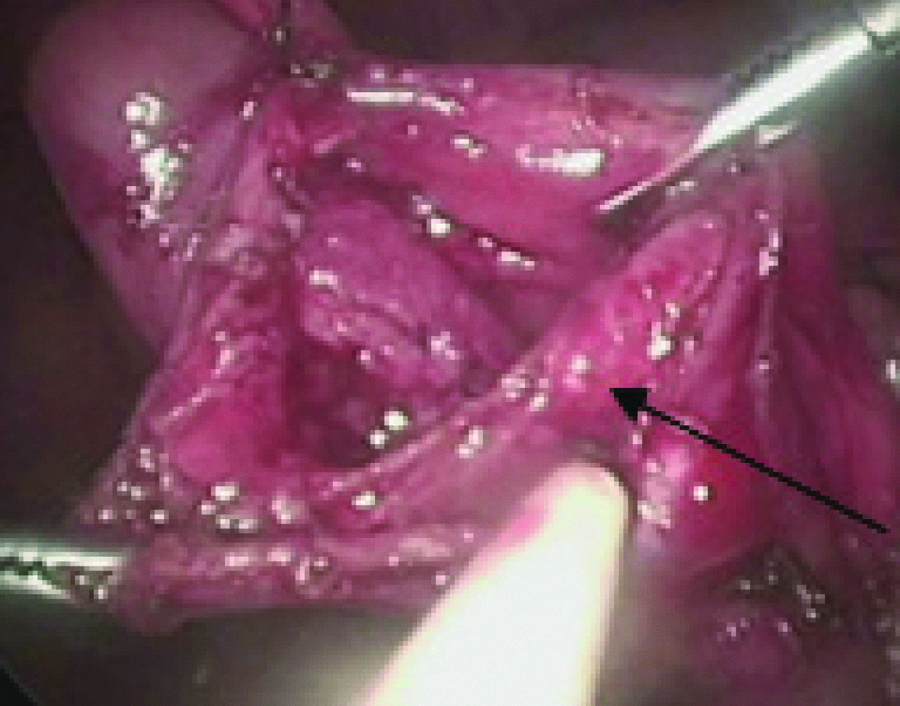
Duodenal diaphragm (arrow).
For cases with duodenal atresia (type II) and annular pancreas, diamond anastomosis of the duodenum was successfully accomplished through a laparoscopic approach (Fig. 3). The anastomosis was accomplished by 5-0 polydioxanone (PDS™; Ethicon, Cincinnati, OH) running sutures.
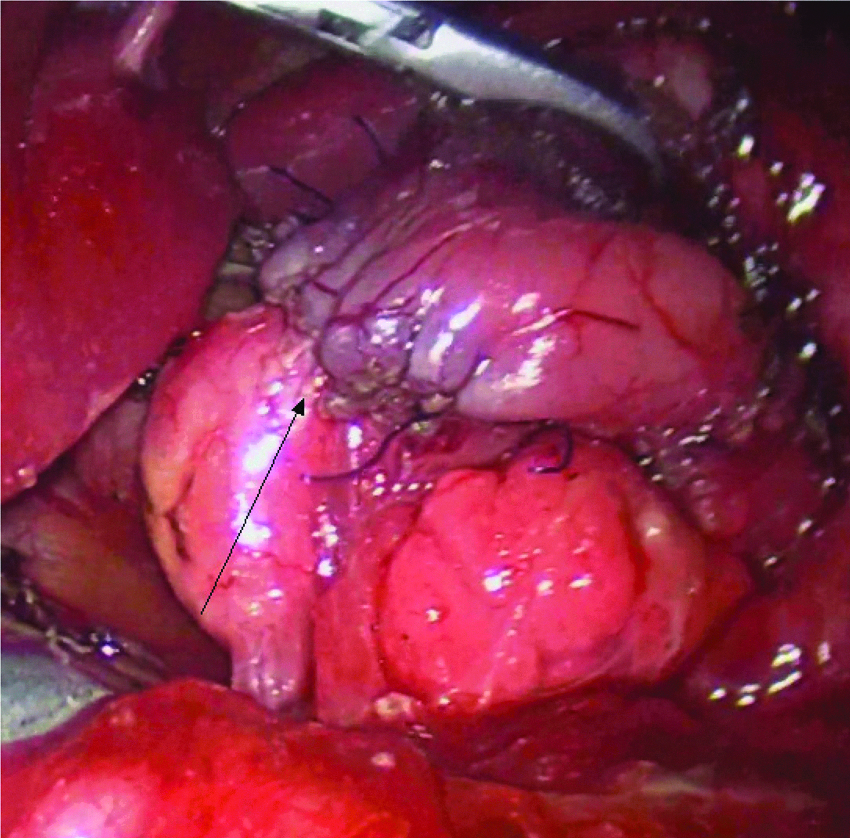
Diamond anastomosis (arrow) was accomplished.
For cases of intestinal malrotation Ladd's procedures were performed (Fig. 4). The vitality and rotational status of the intestines were assessed at laparoscopy. The intestines were rotated by gentle brushing, and Ladd's bands were divided where appropriate, widening the base of the mesentery as much as possible, before the appendectomy was performed.

Dividing Ladd's band.
Results
From September 2009 until October 2012, laparoscope-assisted procedures for duodenal obstruction in 40 neonates were performed. Of the 40 patients, 26 were male, and 14 were female, with a median age of 4.2 days (range, 1–12 days); 11 were born prematurely. Median weight was 3.1 kg (range, 2.4–3.5 kg). The median gestational age was 37 weeks (range, 34–39 weeks). Six patients had Down's syndrome, and 5 had congenital heart disease (Table 1).
Of the 40 patients who presented with congenital duodenal obstruction, for the neonate with an annular pancreas complicated with duodenal windsock deformity, duodenal web resection and diamond-shaped anastomosis were performed through a slightly enlarged umbilical port incision. The length of incision was about 2.5 cm, and the operative time was 70 minutes. One child had a high anorectal malformation, and colostomy was performed laparoscopically. Four days after the operation, the patient still had bilious vomiting, and abdominal X-ray examination showed double bubble sign. Laparoscopic exploration was performed, annular pancreas was diagnosed, and duodenal diamond anastomosis was accomplished laparoscopically. Two cases of duodenal obstruction were diagnosed as annular pancreas complicated with intestinal malrotation, and duodenal diamond anastomosis and Ladd's procedure were accomplished laparoscopically at the same time (Table 2). Other cases were all managed laparoscopically. No cases converted to open surgery. The average operative time was 145 minutes (range, 130–170 minutes).
Feedings were started on postoperative Day 3–7, without abdominal distention and vomiting, and discharge was on postoperative Day 9–14 (Table 3). The patients recovered uneventfully, and symptoms were alleviated with normal gastrointestinal function. The in-hospital and 30-day mortality rates were zero. Three patients were lost to follow-up. One patient with duodenal stenosis developed the complication of megaduodenum 2 months later and was reoperated on with the duodenoplasty technique. For 1 case of intestinal malrotation, adhesive intestinal obstruction with intestinal gangrene and perforation occurred 4 months after the operation. Although laparotomy was performed, the patient was not cured and died eventually. Another patient with anorectal malformation complicated with annular pancreas died of pneumonia complicated with heart failure 6 months postoperately. Other patients were followed up for 4–39 months (mean, 17.1 months) and were doing well.
Data are mean (range) values as indicated.
Discussion
Congenital duodenal obstruction during the newborn period is a relatively common abnormality and may be complete or partial and intrinsic or extrinsic. 2
The indications for pediatric laparoscopy have increased markedly over the last decade as improved video equipment, smaller instruments, and more experienced surgeons have pushed minimally invasive surgical techniques into the neonatal population. 3 One of the major advantages of laparoscopy in managing duodenal obstruction is visibility. 4 The lack of bowel distention was the main factor for visibility. The duodenal obstruction means the entire jejunum and ileum are decompressed; the absence of air in the bowel distal to the duodenum is of great advantage because the small intraabdominal working space in neonates makes laparoscopic operations more difficult and time-consuming than in older children and adults. 5 In all the cases of duodenal atresia and annular pancreas, duodenoduodenostomy had been performed with running suture techniques without any observed leaks and any other complication. A technical maneuver, placing a transabdominal traction suture through the duodenum, was used to facilitate our visibility when duodenoduodenostomy was performed in the cases of duodenal stenosis. 6 In the cases of annular pancreas, a traction suture was used to elevate the liver for visibility. Under laparoscopic vision, the cause of duodenal obstruction could be diagnosed, and the laparoscopic procedure could be completed easily.
Our results showed a prompt start of feedings and discharge from hospital after a short period. The long-term results in our limited series were similar to results obtained with an open technique. The anastomosis requires a prolonged operative time and a considerable learning curve.
In summary, our experience demonstrates that laparoscopic treatment for neonatal duodenal obstruction could be performed safely and successfully with excellent outcomes. Our study supports laparoscopy as a safe, first-line approach to duodenal obstruction. Moreover, patients can be managed laparoscopically, even if they require other procedures, such as Ladd's procedures. 7 The use of a 30° scope is recommended. Further refinement of laparoscopic instruments and techniques will allow pediatric surgeons to apply this method efficiently, safely, and cost-effectively to more neonates with duodenal obstruction. 8
We believe that these techniques could confer numerous benefits to the patients, including shorter recovery times and in many cases shorter hospitalization, less pain, and less adhesion formation and scarring, and are worth being considered for widespread use. 9
Footnotes
Disclosure Statement
No competing financial interests exist.