
Abstract
Abstract
Background:
Minimally invasive repairs of pediatric diaphragm eventration have been well described via a thoracoscopic approach, oftentimes requiring single-lung ventilation and tube thoracostomy, with the disadvantage of not being able to clearly visualize what lies beneath the diaphragm. We describe a novel pediatric diaphragm eventration repair using a laparoscopic transperitoneal approach and an endostapler device. We also describe our initial experience with this technique.
Patients and Methods:
Four pediatric diaphragmatic eventration patients underwent laparoscopic transperitoneal repair using an endostapler device. Repairs were performed in both male and female patients with right-sided eventrations. We approach the repair in a transperitoneal fashion using inverting sutures at the apex of the diaphragm to create tension toward the pelvis. Subsequently, an endostapler is used to remove the redundant portion of diaphragm, leaving a repaired, taut diaphragm.
Results:
The median age at operation was 10.5 months. The median operative time was 70 minutes. There was no mortality, surgical complications, or recurrence at a median follow-up of 17 months.
Conclusions:
This laparoscopic approach allows for clear visualization of the intraabdominal organs and, at least in our early experience, a very simple, straightforward operation. Additionally, with the use of the endostapler, the redundant, often weakened diaphragm is removed, leaving the native, healthy diaphragm behind, resulting in a reliable and reproducible repair. This repair should be considered as a feasible alternative approach to the more traditional open and thoracoscopic repairs.
Introduction
Regardless of the etiology, diaphragm eventration must be differentiated from congenital diaphragmatic hernia, in which there is an absence of part, or all, of the diaphragm, allowing herniation of abdominal contents into the thoracic cavity. Diaphragmatic eventration results in paradoxical motion of the diaphragm due to pressure from the abdominal contents along with simultaneous negative inspiratory pressure pulling the diaphragm into the chest cavity. This is the mechanism by which diaphragm eventration can result in significantly impaired pulmonary function.
Symptoms of diaphragm eventration range from being asymptomatic to being unable to wean from mechanical ventilation. Within these extremes, symptoms include respiratory distress, frequent severe pneumonias, and failure to thrive. Patients who have symptomatic eventration meet criteria for repair. 2 An asymptomatic patient with an elevated hemidiaphragm above the fourth intercostal space meets the relative indication for repair, which should be considered up until the age of 7 or 8 years given the potential for the eventration to compromise lung growth. When injury to the phrenic nerve is suspected as an etiology, a reasonable trial of nonoperative therapy is warranted.
Surgical plication of diaphragmatic eventration with prosthetic reinforcement was first described in 1923, 3 with complete repairs in the both adult and child being reported decades later.4–6 The general technique centers around incising the diaphragm at the costal attachments and placing nonabsorbable sutures in a horizontal mattress fashion at the costal attachments when the diaphragm is under tension. 7 The use of a prosthetic was subsequently introduced as an alternative to or reinforcement of the plication.8,9 Since then, a variety of open techniques have been described, with approaches from the chest and the abdomen.
The minimally invasive approach to eventration repair in the pediatric population has been thoracoscopic until now. In the thoracoscopic technique, suture is used to invaginate the eventration and gather redundant diaphragm, while a second suture is used to maintain and adjust the desired tension. 10 This technique has been described with both running and interrupted sutures.11,12 The use of an endostapler to assist in the surgical correction of the eventration via a thoracoscopic approach has been described. Tension was created by grasping the central diaphragm, and the stapler was used to attach opposing sides of the diaphragm while leaving the remaining diaphragm in situ.11,13 Minimally invasive techniques have gained in popularity owing to the perceived decrease in morbidity.
The laparoscopic approach has been described in adults using a variety of techniques, including suture plication, mesh reinforcement, and endostapler repair.14–16 Proponents of this approach tout the advantages of less intercostal nerve pain, avoidance of single-lung ventilation, improved working space, and improved visualization of intraabdominal organs with reduced risk of visceral injury.15,16
Here, we demonstrate the use of an endostapler in a minimally invasive eventration repair in pediatric patients and describe our initial experience with this novel approach. We approach the repair laparoscopically. The redundant diaphragm is inverted downward toward the pelvis with suture, and with an endostapler, the weakened portion of the diaphragm is resected. In our experience, this approach allows for clear visualization of the intraabdominal organs, avoids a thoracostomy tube, and gives a reliable and reproducible result. Furthermore, this procedure has a reasonable operative time and has the potential to be done on an outpatient basis.
Patients and Methods
General patient data
We conducted repairs on four pediatric patients (Table 1) with right-sided diaphragmatic eventration with a median age of 10.5 months old (range, 4 months–10 years), both males and females. We do not report left-sided eventration repairs because of the lack of presentation. Three of the four patients had recurrent pneumonia as the indication for repair of the diaphragmatic eventration. Patients were discharged by postoperative Day 1 or 2. Follow-up shows no recurrences, with a median follow-up of 13.5 months (range, 5–24 months).
With circumcision.
With tracheostomy replacement, bronchoscopy, fundoplication, and gastrostomy.
CXR, chest x-ray; F, female; M, male; OSH, outside hospital.
Procedures
Patient evaluation
This transperitoneal approach we describe requires no additional work-up beyond the work-up required for traditional approaches. For our patients, we obtained anteroposterior and lateral view x-rays of the chest (Fig. 1). Generally, a right-sided eventration is suspected when the diaphragm appears two ribs higher than the contralateral side. A left-sided diaphragm is suspected when the diaphragm appears one rib above the contralateral diaphragm. Subsequently, the addition of either diaphragm fluoroscopy or ultrasonography allows dynamic visualization of the diaphragm and confirms the diagnosis by demonstrating paradoxical or the absence of diaphragm movement with inspiration. The specific work-up for each of the four patients is shown in Table 1.

Preoperative chest radiograph demonstrating right-sided diaphragmatic eventration.
Operative technique
Anesthesia is standard, using both intravenous and inhalational agents as in typical laparoscopic surgery. With this laparoscopic approach, there is no need for single-lung ventilation.
The patient is positioned supine and centered on the bed, allowing access to both sides of the chest for both suture traction and stapler placement. A slight reverse Trendelenburg position allows for the intestinal contents to fall away from the diaphragm to aid in visualization.
Port placement is critical and dependent upon the side of the eventration (Fig. 2). A 5-mm camera port is placed in the umbilicus, and the abdomen is insufflated to 15 mm Hg. For a right-sided eventration, a 12-mm port is then placed in the left upper quadrant in the anterior axillary line just below the costal margin, and a 5-mm port is placed in the right lower quadrant. For a left-sided eventration, the 12-mm and 5-mm port sites are reversed. Once the instruments are in the abdomen, the falciform ligament is taken down with cautery up to the hepatic veins. The apex of the eventration is usually easily visualized, as it is nearly transparent. This transparency allows visualization of the lung parenchyma in the thorax (Fig. 3). Through the 5-mm lower quadrant port, a 2-0 suture is advanced and then grasped inside the abdomen. Prior to placing sutures in the diaphragm, the lung movement is visualized, and an inspiratory arrest may be assistive. The suture is then placed through the apex of the eventration and brought back out through the same 5-mm port (Fig. 4). This is done with an additional 2-0 suture to help disperse the tension on the thin tissue. Maximal tension is then applied to the sutures to invert the diaphragm into the abdomen and to create a taut repair. An Ethicon Endo-Surgery (Cincinnati, OH) ATS 45-mm articulating endostapler with a TR45W staple load (2.5 mm open height and 1 mm closed height) is then brought into the abdomen through the 12-mm port in the upper, lateral abdomen. Using the endostapler, the redundant diaphragm is subsequently divided transversely from medial to lateral (Fig. 5). This repair generally requires three or four separate staple fires (depending on size) to come across the redundant diaphragmatic muscle, which is then removed through the 12-mm port. Inspection of the diaphragmatic staple line confirms repair (Fig. 6). The ports are removed, and the sites are closed with absorbable sutures. The technique reported here has not been previously reported in the literature in the pediatric patient; however, it is similar to a technique discussed in the Rainbow Babies Children's Hospital “Tricks of the Trade in Pediatric Surgery Web Symposium 2010.” 17
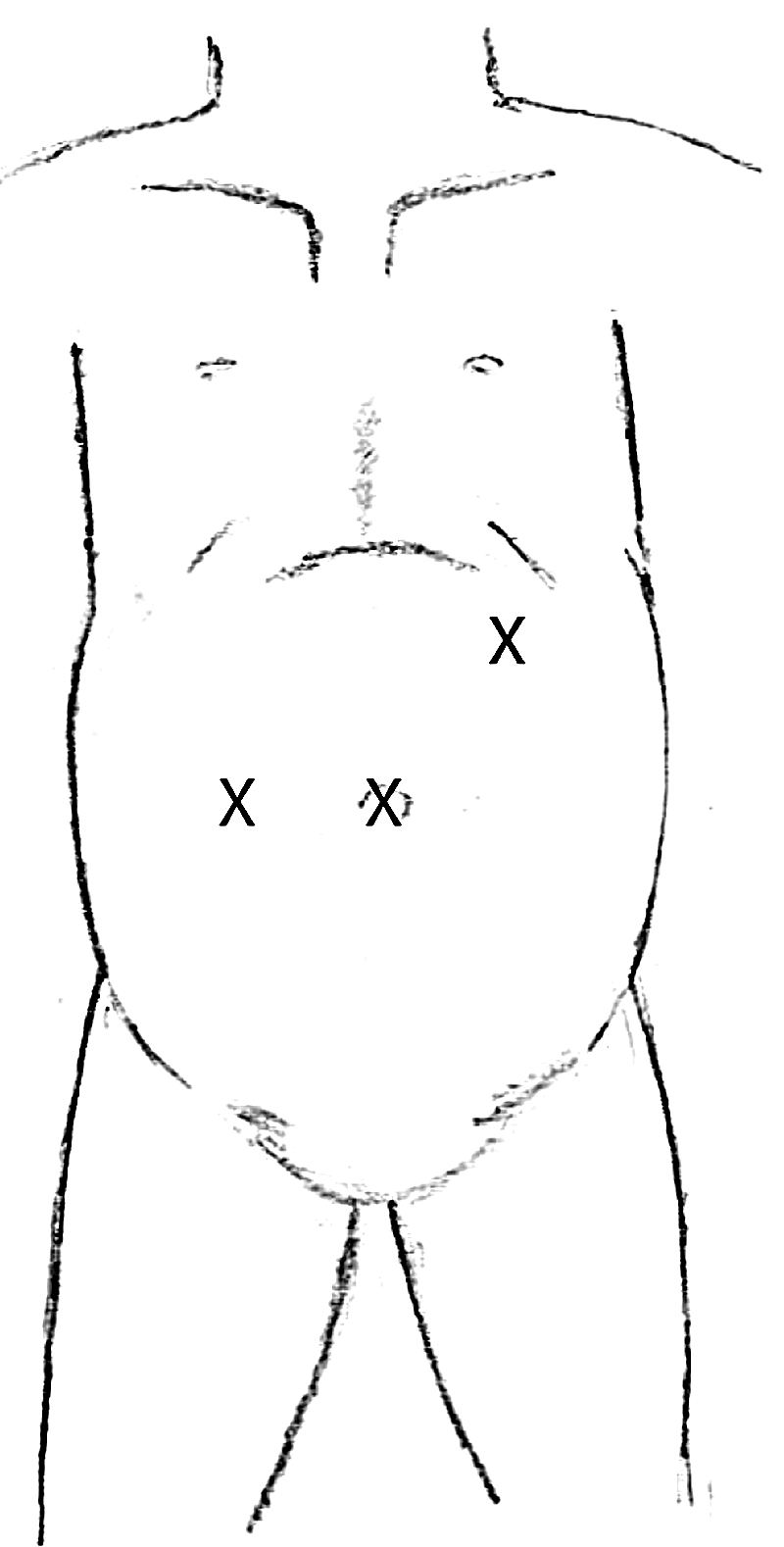
Port placement for a right-sided diaphragmatic eventration. A 5-mm camera port is placed in the umbilicus, a 12-mm port is placed in the left upper quadrant in the anterior axillary line just below the costal margin, and a 5-mm port in the right lower quadrant.
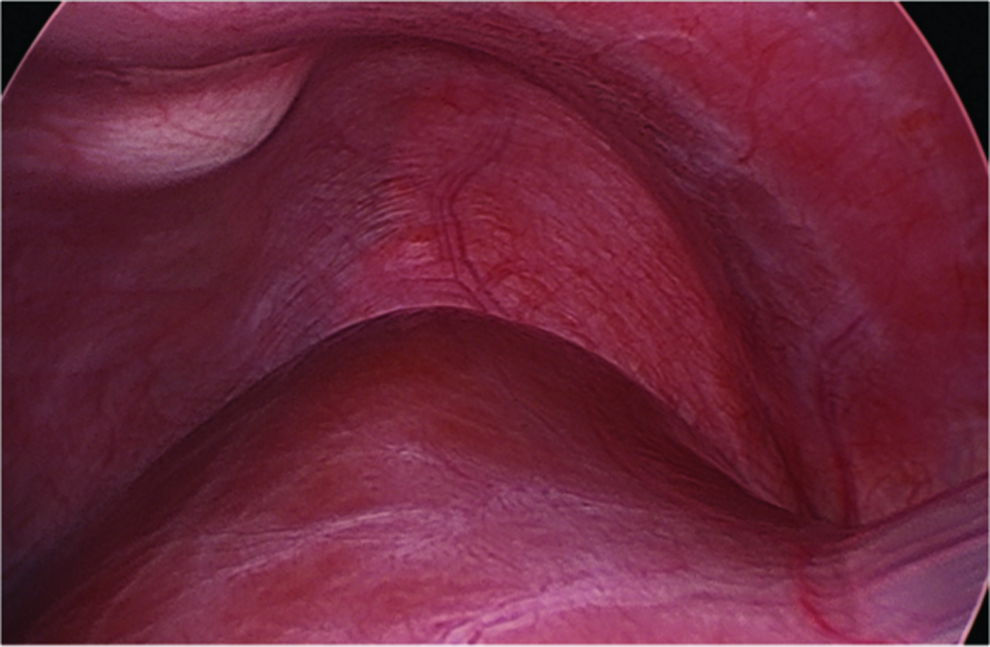
Laparoscopic view of diaphragmatic eventration prior to plication. The apex of the eventration is easily visualized, and it is nearly transparent, allowing for visualization of the lung parenchyma on the other side of the diaphragm.

Laparoscopic view of nonabsorbable sutures through the port, providing external tension in order to pull the redundant diaphragmatic tissue into the abdominal cavity. An inspiratory arrest may be assistive in placing suture through the apex of the eventration. An additional 2-0 suture to helps disperse the tension on the thin tissue. Maximal tension is then applied to the sutures to invert the diaphragm into the abdomen.

Laparoscopic view of the endostapler across the diaphragm eventration. Using the endostapler, the redundant diaphragm is subsequently divided from medial to lateral. Generally, three to four separate staple fires are needed to come across the redundant diaphragmatic muscle.
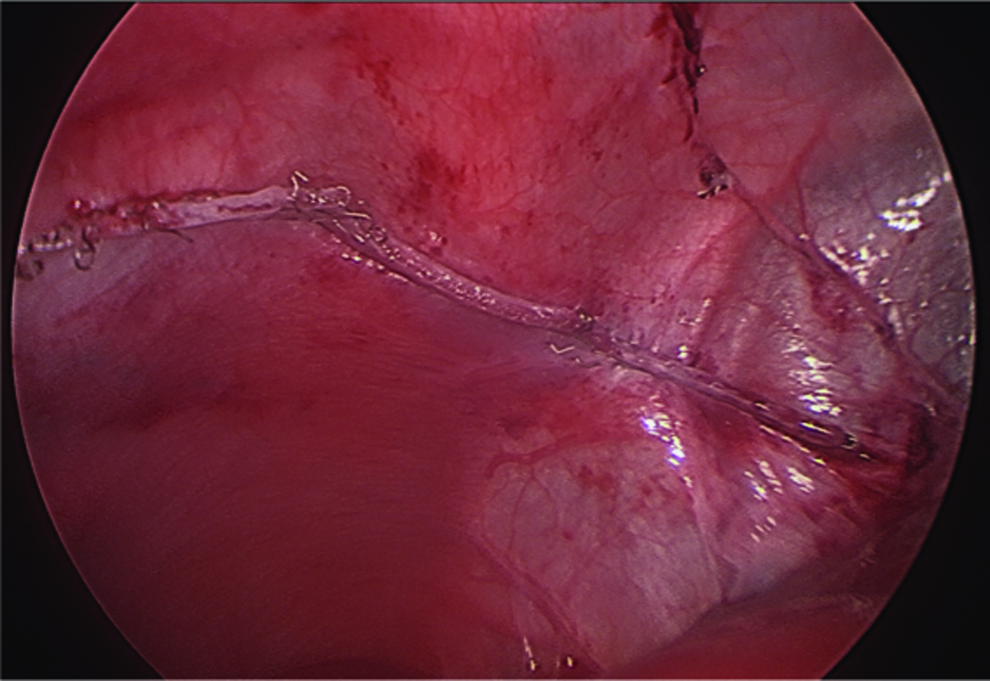
Laparoscopic view of the completed diaphragmatic plication. Inspection of the diaphragmatic staple line confirms repair.
A postoperative chest radiograph is obtained to establish a new baseline as well as to confirm the absence of a pneumothorax (Fig. 7). The patient can resume a regular diet and potentially be discharged as early as the day of the operation. Oral pain medication is used for postoperative pain control. The initial follow-up is performed at 2 weeks with a chest radiograph. Follow-up is then performed yearly for 4 years, as the remaining diaphragm may continue to atrophy, depending on the degree of phrenic nerve dysfunction.

Postoperative chest radiograph confirming repair of the eventration with no evidence of a pneumothorax.
Results
Laparoscopic transperitoneal repair of a diaphragm eventration using an endostapler proved successful in all of our patients, with no recurrences at a median follow-up of 17 months. The median operating time was 70 minutes (Table 1). All of the procedures were performed without intraoperative complications, and pulmonary function was not compromised by the pneumoperitoneum. There were also no incidences of postoperative pneumothorax as assessed by a postoperative upright chest radiograph.
For the 3 patients with recurrent pneumonia as the indication for operations, our repair abated the recurrent pulmonary infections. The 10-month-old male patient with three preoperative admissions for pneumonia, on follow-up, has had no hospital admissions since the operation. The 10-year-old male patient with a tracheostomy, whose indication was also recurrent pneumonias, had a preoperative history of 13 admissions over 7 years for pneumonia. On follow-up, he was admitted twice for unrelated reasons and requires decreased ventilator settings postoperatively. The 11-month-old female patient had one preoperative admission for pneumonia with evidence of diaphragm eventration. Postoperatively, this child has not had any hospital admissions.
For the 4-month-old male child whose indication was respiratory distress and poor feeding, our repair aided in the resolution of his failure to thrive and respiratory distress.
Discussion
We describe a novel laparoscopic eventration repair in the pediatric population with the use of an endostapler as well as our initial experience with this repair. Based on our experience, this minimally invasive repair is a good alternative to the currently accepted thoracoscopic and open approaches.
This laparoscopic approach provides clear visualization of the intraabdominal organs from the vantage point of the abdominal cavity, as opposed to visualizing intraabdominal organs through the weakened diaphragm. This vantage point may be a desirable option in cases where bowel adhesions to the diaphragm are expected. This procedure is also a great alternative to an approach from the thorax when other intraabdominal procedures are planned, such as a fundoplication and gastrostomy (Table 1). Furthermore, this approach avoids the need for intraoperative placement of a tube thoracostomy for this approach, which is expected to decrease operative time, and makes this procedure compatible with outpatient status.
With regard to intraoperative anesthesia, this laparoscopic approach avoids single-lung ventilation. Single-lung ventilation in the pediatric population oftentimes is technically challenging, especially left-sided endotracheal tube placements, and therefore is time consuming. 18 Furthermore, because of the size and physiology of infants and small children, there is an increased risk of significant oxygen desaturation during surgery in the lateral decubitus position, making single-lung ventilation less desirable, and an option of providing oxygen to the operative lung should be readily available.19,20
Although the technique described here can be completed via a laparotomy, the laparoscopic approach provides the benefits of a minimally invasive approach, including better visualization of the diaphragm, decreased length of stay, minimal scarring, and decreased postoperative need for analgesia.21,22
The main limitation to this technique lies with size of the patient. As the endostapler must pass through a 12-mm port, the child must be large enough to accommodate not only the port, but also the smallest size endostapler available, which is 35 mm.
A concern with this technique may be a negative effect of pneumoperitoneum in a patient with baseline recurrent respiratory infections or respiratory distress. In our experience, we did not observe any respiratory embarrassment in our patients in the presence of pneumoperitoneum. Another concern that one might have with pneumoperitoneum in this setting may be the blowing of the diaphragm into the chest providing an obstacle to an ideal repair. This was not the case in our experience. We found that the traction sutures placed allow for countertension as well as the ability to adjust the tension in order to achieve the operative goal of a flat diaphragm. Furthermore, the degree of pneumoperitoneum can be adjusted.
As there is a concern for possible visceral injury with a thoracoscopic approach due to limited visibility of the peritoneal cavity, with this technique, there may be a concern for possibility lung injury. If this were to occur, it would be more likely from the initial traction suture as opposed the stapler. Once the traction sutures are placed, the two edges of the diaphragm stay opposed to each other secondary to the negative pressure in the chest, and therefore the lung cannot become trapped within the diaphragm that is being removed. In addition, in our experience, the lung parenchyma is easily visualized through the diaphragm eventration. We did not find it difficult to grab and invaginate the diaphragm into the abdomen in order to rule out lung adhesions to the diaphragm prior to placement of the traction suture. We also found that an inspiratory arrest during this time can aid in accurate placement of the traction suture.
We present the first description of this minimally invasive, laparoscopic repair in the pediatric age group and describe our initial successful experience. We propose that this laparoscopic transperitoneal repair with an endostapler be considered in pediatric patients who present with a symptomatic diaphragmatic eventration.
Footnotes
Acknowledgments
This study was supported by grant F32CA1591555-01 from the National Cancer Institute, National Institutes of Health (to V.V.L.).
Disclosure Statement
No competing financial interests exist.