
Abstract
Abstract
Background and Objective:
In cases of ascites of unknown etiology, tuberculosis peritonitis (TBP) is a possible cause but a diagnostic challenge. This retrospective case series assessed the effectiveness and safety of diagnostic natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and the Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) in 7 consecutive patients with suspected TBP.
Subjects and Methods:
Between September 2011 and August 2012, peritoneal biopsy was performed using transgastric NOTES for subsequent histology in 7 consecutive hospitalized patients who presented with ascites and were diagnosed with suspected TBP. The outcome measures included diagnostic accuracy and procedure-related morbidities.
Results:
Diagnostic NOTES was successfully completed in all 7 patients. Peritoneoscopy with NOTES went uneventfully and lasted 5–10 minutes. Typical peritoneal nodules characteristic of TBP were identified in all patients and confirmed pathologically as TBP. No clinically significant adverse events occurred in any patients following NOTES, except for 1 patient who experienced mild and transient pyrexia. Postoperative blood culture detected no microbial growth. Follow-up upper gastrointestinal endoscopy showed that the gastric wall wound healed well with minimal scarring. All patients were prescribed a standard four-drug antituberculosis chemotherapy regimen. The treatment outcomes were determined to be effective or curative, and no relapse was detected within the follow-up period.
Conclusions:
NOTES is an effective and safe diagnostic technique in patients with suspected TBP presenting as ascites of unknown etiology.
Introduction
TBP derives mainly from reactivated latent tuberculous foci in the peritoneum that previously spread hematogenously from a primary pulmonary focus. Less frequently it is from intra-abdominal tuberculosis, such as intestinal tuberculosis, tuberculous mesenteric lymphadenitis, and tuberculous salpingitis. Individuals susceptible to TBP are primarily patients whose immune systems are suppressed with complicating human immunodeficiency virus infection, liver cirrhosis, diabetes mellitus, malignancies, and renal failure requiring continuous ambulatory peritoneal dialysis. 4
Like other types of extrapulmonary tuberculosis, TBP has an occult onset and usually presents as fever, abdominal pain or distension, and ascites. Ascites associated with TBP usually results from peritoneal lymphatic obstruction and the interruption of peritoneal fluid reabsorption 5 and only rarely from secondary portal hypertension. 6
TBP should be added to the differential diagnosis when patients exhibit chronic, septic peritonitis, especially those with a known history of tuberculosis. However, TBP has no characteristic or specific clinical features, and current microbiological investigation techniques are not effective in isolating M. tuberculosis. Therefore, diagnosis of TBP is often a challenge for gastroenterologists, general surgeons, and radiologists, especially in cases of isolated transudative ascites of unknown etiology. Such ascites frequently mimics peritoneal carcinomatosis (PC) metastasizing from ovarian cancer and other gynecological malignancies in female patients. 7 Combinations of noninvasive imaging and laboratory techniques are reported to help differentiae TBP from PC, which is usually incurable and associated with a poor prognosis. Abdominal computed tomography scan may identify radiological signs of concomitant intestinal tuberculosis and tuberculous mesenteric lymphadenitis. 8 Paracentesis with an adenosine deaminase assay may be helpful in differentiating TBP from PC. 9 Ascites microbiology barely detects any acid-fast bacilli, 10 and DNA polymerase chain reaction assay for M. tuberculosis frequently produces false-positive results, although with an improved sensitivity. 11 All of the above methods are restricted by the failure to establish a definitive diagnosis in either the microbiological or pathological aspects.
Diagnostic laparoscopy with target biopsy, namely, peritoneoscopy, enables a rapid and accurate diagnosis of TBP with a favorable safety profile. Its diagnostic efficacy has been well acknowledged in current practice.12,13 However, this minimally invasive technique is still subject to some procedure-related complications, such as intra-abdominal bleeding, enterocutaneous fistula, tuberculous dissemination, and hepatorenal failure.12,13 Additionally, the use of diagnostic laparoscopy is risky and less helpful in cases of the fibroadhesive form of TBP, where it sometimes requires conversion to laparotomy. 14
First described by Anthony Kalloo and colleagues 15 in 2004, natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and the Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) is a newly emerging, experimental, interventional endoscopy. In most cases NOTES entails the insertion of a flexible endoscope into a natural orifice, such as the mouth, anus, or vagina, and then through an internal incision made in the stomach, colon, or vagina, respectively, for entry into the abdominal or pelvic cavity. This technique allows direct visualization and histological examination of ascites and peritoneal disease, in the absence of pneumoperitoneum and without making an abdominal skin incision. Thus, NOTES overcomes the access restriction of traditional endoscopy by the gastrointestinal lumen. Multiple diagnostic and therapeutic procedures have been successfully completed using NOTES, such as peritoneal exploration with biopsy, 16 liver biopsy, appendectomy, 17 cholecystectomy, 18 hysterectomy, 19 oophorectomy, 20 and even nephrectomy. 21
Beginning in September 2011 we have used peritoneoscopy with NOTES for the definitive diagnosis of suspected TBP that presented as nonspecific ascites of unknown etiology. The present study is a retrospective case series of 7 patients, undertaken to assess the diagnostic effectiveness and safety of diagnostic NOTES in the differential diagnosis of suspected TBP.
Patients and Methods
Patient selection
The Institutional Review Board at the First Affiliated Hospital of Nanchang University (Nanchang, China) approved the study protocol in accordance with the latest edition of the Helsinki Declaration. Seven patients (3 men and 4 women) exhibiting ascites of unknown etiology, which was suspected to be TBP, were consecutively referred to our gastroenterology unit between September 2011 and August 2012. All of these patients, who were hospitalized for elective peritoneal exploration and biopsy using NOTES, were retrospectively identified based on the review of medical charts (Table 1).
Diagnostic workup of ascites
The routine hematology test showed anemia (reference range, <120 g/L for males and <110 g/L for females) in 2 female patients, normal white blood cell count (4.0–10.0×109/L) in 4 patients, leukocytosis (>10.0×109/L) in 1 patient, and leukopenia (<4.0×109/L) in 2 patients. Biochemistry identified normal hepatorenal function in all patients, except for 1 patient with mild elevation in serum aspartate transaminase activity (>40 U/L). The erythrocyte sedimentation rate (0–15 mm/hour for males and 0–20 mm/hour for females) increased in 3 patients. Serial serum tumor marker assays showed the level of cancer antigen 125 was increased significantly in all patients (range, 338–1547 U/mL; mean, 686.5 U/mL; normal limit, <35 U/mL), but levels of carcinoembryonic antigen (0–10 ng/mL) and cancer antigen 19-9 (<35 U/mL) remained within normal limits. The skin purified protein derivative test was performed in 3 patients, and the reaction was positive in 1 patient and negative in 2 patients. The blood ELISPOT (TSPOT.TB) assay (Oxford Immunotec, Abingdon, United Kingdom) was used in 5 patients, all of whom showed positive results.
Chest radiography and computed tomography scan revealed no pulmonary tuberculosis foci, but concomitant pleural effusion in 3 patients and pulmonary infection in 3 patients were seen. Abdominal computed tomography scan identified moderate to massive ascites in all 7 patients, mesenteric thickening in 3 patients, and mesenteric lymph node enlargement in 2 patients. Esophagogastroduodenoscopy and colonoscopy were ordered to identify any signs that were suggestive of gastrointestinal tuberculosis, inflammatory bowel disease, or malignancies, but no clinically significant abnormalities were found in any of the patients.
To characterize ascitic fluid in terms of cytology, biochemistry, and microbiology, bedside ultrasonography-guided paracentesis was performed. Serum-ascites albumin gradient was determined to be low in 6 patients (<1.1 g/dL) and high in 1 patient (>1.1 g/dL). Ascitic fluid analysis showed a lymphocyte-dominated cellularity, with a total number of nucleated cells ranging from 450 to 2400/mL (<100/mL for transudate and >500/mL for exudate), but without any detectable neoplastic cells on cytology. The ascitic lactic dehydrogenase level ranged from 194 U/L to 474 U/L (mean, 330±91 U/L) (ascites lactic dehydrogenase:serum lactic dehydrogenase ratio ≥0.6 for exudate and <0.6 for transudate). The adenosine deaminase level ranged from 17 U/L to 52 U/L (mean, 31.1±11.8 U/L; normal limit, <50 U/L), with mild elevation in 1 patient.
Peritoneal exploration with NOTES
Peritoneal exploration with transgastric NOTES was scheduled to facilitate a definitive diagnosis of TBP and rule out possible PC. None of these patients had cases with complications of coagulopathy, serious cardiopulmonary insufficiency, peptic ulcer, or gastroduodenal obstruction on preoperative assessment. All patients, or their legal representatives for minors, volunteered to give informed consent in writing prior to peritoneal exploration. An assigned endosurgical team led by a board-certified endosurgeon (Y.-X.C.) performed the surgery. The team consisted of surgical residents, anesthesiologists, surgical nurses, histopathologists, clinical microbiologists, and research nurses. Preoperative fasting and intravenous antimicrobial prophylaxis were routinely given.
The operative procedure was performed as previously reported. 22 In brief, patients were intubated under combined intravenous–inhalational anesthesia and placed in the left recumbent position. A flexible, single-channel, video endoscope (model GIF-260; Olympus, Tokyo, Japan), 9.0 mm in outer diameter, 110 cm in length, was inserted using the Seldinger technique through the mouth into the gastric cavity, and the anterior wall of the gastric body was marked at the middle portion using a high-frequency needle-knife (model HPC-3; Cook Endoscopy, Bloomington, IN) for the proposed incision. Gastric content was completely aspirated, and the gastric cavity was repeatedly rinsed with 1000 mL of sterile water. The incision mark was disinfected using 5% povidone–iodine (Viacom Pharmaceutical, Shenyang, China). The stomach was inflated with medical nitrogen dioxide, and an endoscopic needle-knife (HPC-3; Cook Endoscopy) was used to make a 1-cm-long full-thickness incision in the gastric wall along the proposed incision line (Fig. 1A).
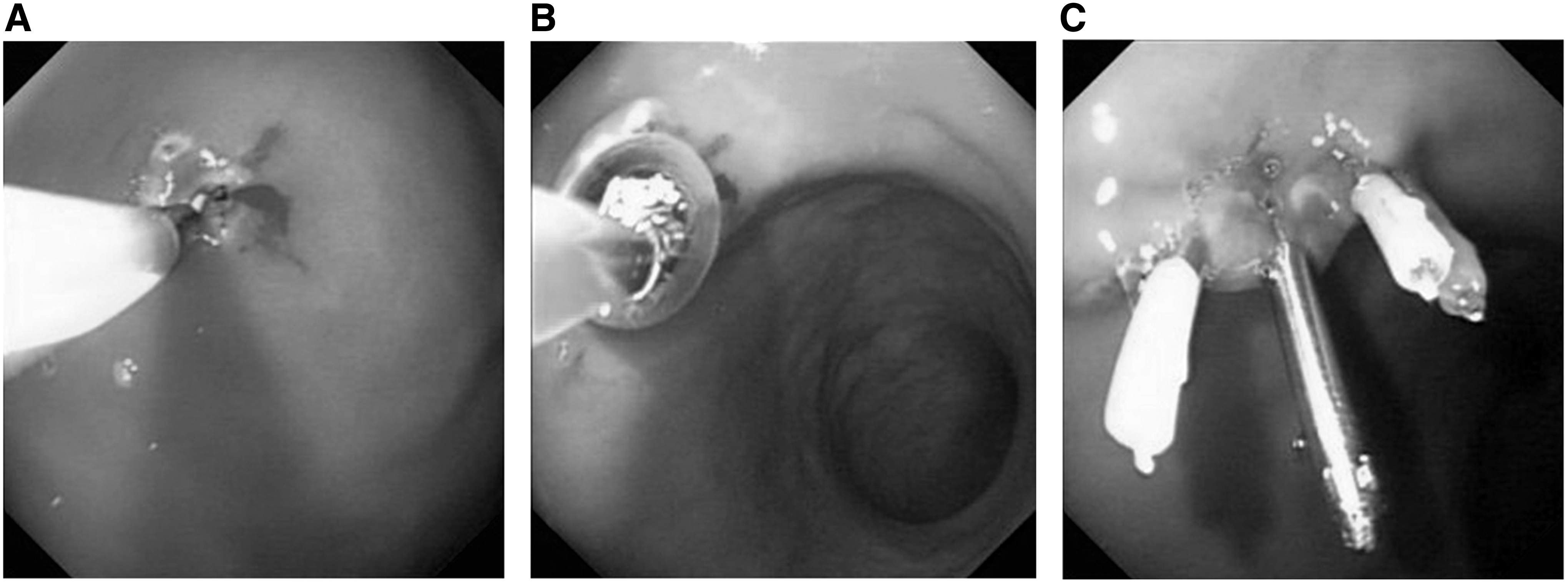
Operative procedure of peritoneoscopy using natural orifice translumenal endoscopic surgery.
A guidewire (0.89 mm×450 cm; Boston Scientific, Natick, MA) was inserted into the incision, and a 1.0 cm×3.0 cm-size endoscopic balloon (model QBD-10X3; Cook Endoscopy) was used to dilate the incision in a radial manner and create a 12–15-mm gastrotomy opening for the passage of the endoscope into the peritoneal cavity (Fig. 1B). The endoscope was subsequently advanced into the peritoneal cavity, and the patient's position could be adjusted to facilitate the advancement of the endoscope. Ascitic fluid aspiration or low-pressure pneumoperitoneum was used, if necessary, to ease the exploration of parietal peritoneum, mesenteries, liver, and intestines.
Peritoneoscopy was performed to identify any characteristic signs of TBP as described by Bhargava et al. 23 Any suspicious peritoneal disease sites were appropriately biopsied for pathological examination; a small amount of oozing required no hemostasis, and significant bleeding was controlled using cauterization. The endoscope was withdrawn, and titanium endoclips (model HX-610-135/L; Olympus) were deployed to close the gastric wall wound appropriately (Fig. 1C).
Postoperative care and follow-up
Gastroduodenal decompression was routinely administered, and a 19-gauge needle (1.0×30 mm; TWLB; Jiangxi Sanxin Medtec, Nanchang) was punctured into McBurney's point to deflate the peritoneal cavity. Patients were instructed to fast until the removal of the gastric tube and medicated with intravenous first-generation cephalosporin and proton pump inhibitor. Blood culture using BacT/Alert®-FA blood culture bottles (bioMérieux SA, Marcy l'Etoile, France) was ordered in 6 patients to detect any bacteremia.
Definitive diagnosis of TBP was established on the basis of caseous granuloma on histology, positive acid-fast staining, or both. A standard, 6-month, combined antituberculosis chemotherapy regimen for extrapulmonary tuberculosis was started immediately after a pathological diagnosis of TBP, in accordance with the 2010 World Health Organization Guidelines for Treatment of Tuberculosis, 4th edition. 24 Intravenous isoniazid (0.5 g daily) was given until the patient's body temperature returned to normal, when it was replaced by oral isoniazid (0.3 g daily). Daily supplementary rifampicin (0.45 g), ethambutol (0.75 g), and pyrazinamide (1.0 g) were concomitantly given for 2 months, followed by 4 months of daily isoniazid (0.3 g) and rifampicin (0.45 g) as consolidation therapy. The outcome of antituberculosis treatment was evaluated in accordance with World Health Organization/IUATLD criteria. 25
All patients were scheduled for follow-up at outpatient clinics at quarterly intervals. Routine hematological and biochemical assays were ordered to monitor any adverse drug effects associated with antituberculosis chemotherapy, and follow-up abdominal ultrasonography or computed tomography scan was done to identify any reactivation of abdominal tuberculosis infection.
Results
Operative results
Peritoneal exploration using NOTES was successfully completed in all 7 patients without conversion to laparoscopy. Low-pressure pneumoperitoneum was used in all patients. Suspicious peritoneal nodules were detected and biopsied in all patients. None of the patients required conversion to emergency laparotomy due to uncontrollable bleeding, incidental gastrointestinal perforation, or iatrogenic organ injuries. The duration of peritoneal exploration was 4–10 minutes (mean, 7±3 minutes), and the overall operative time was approximately 30 minutes (mean, 30±10 minutes). Intraoperative bleeding was minimal, and no blood transfusion was given to any of the patients. No iatrogenic injuries or clinically significant incidents occurred intraoperatively.
Macroscopic and pathological results
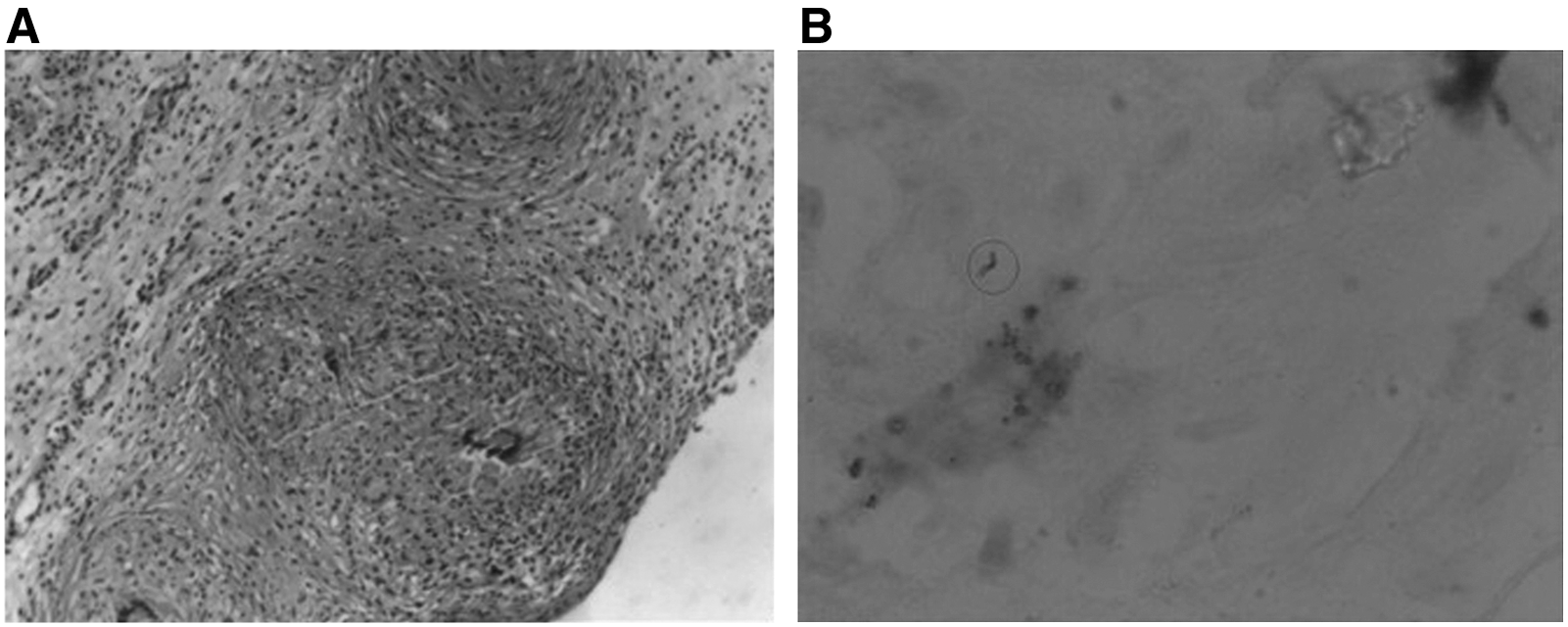
On peritoneoscopy with NOTES, yellowish ascitic fluid that was clean or slightly cloudy and containing no blood was observed in all patients (Fig. 2A). Large numbers of disseminated, white, miliary nodules, at a maximum size of 0.3 cm, were present on the surfaces of thickened parietal peritoneum, mesenteries, liver, and intestines in all patients (Fig. 2B). Massive fibrinous exudates and adhesive bands were identified in 2 patients (Fig. 2C). Additionally, enlarged mesenteric lymph nodes were detected in 2 patients. All these endoscopic findings suggested a preliminary diagnosis of TBP. Further pathological examination revealed granulomatous inflammation with caseous necrosis in all patients (Fig. 3A) and the presence of acid-fast bacilli in 2 patients (Fig. 3B), consistent with a diagnosis of tuberculosis. Therefore, the diagnosis of TBP was established as predefined in all patients.
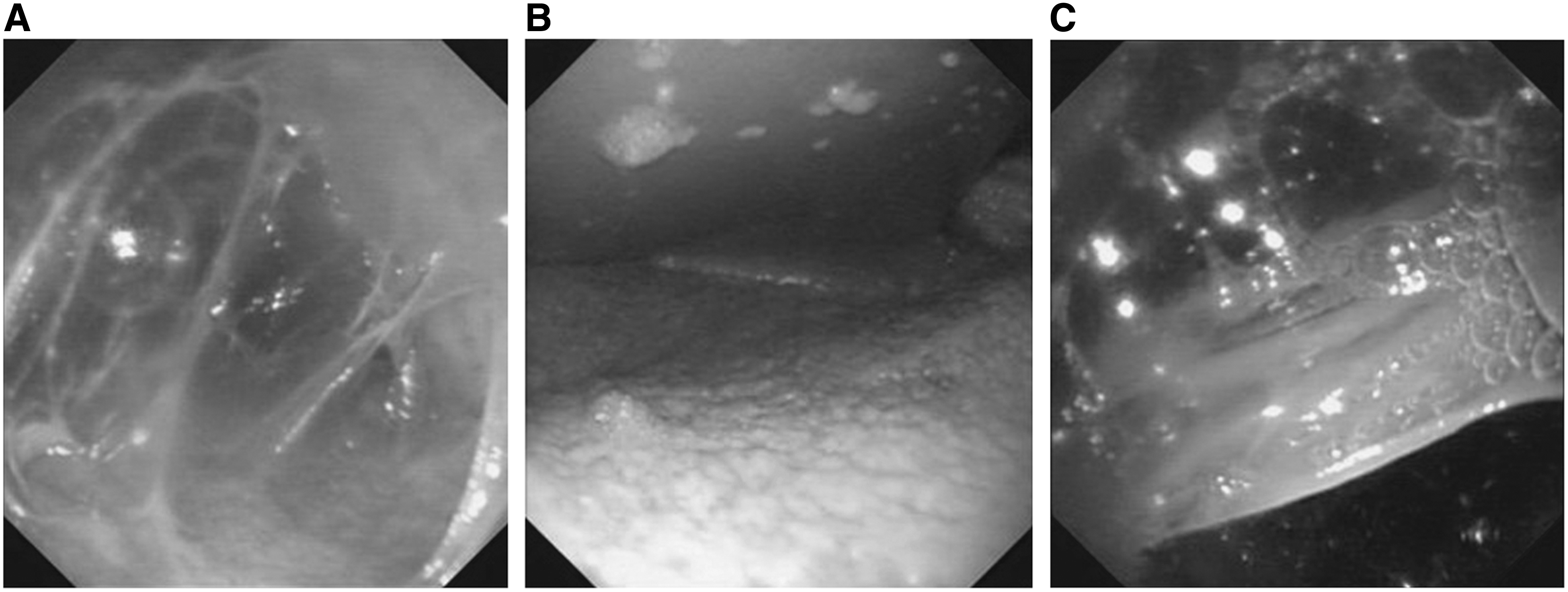
Appearances of tuberculosis peritonitis on peritoneoscopy with natural orifice translumenal endoscopic surgery:
Postoperative recovery
All patients underwent an uneventful postoperative course, except for 1 patient who experienced mild, transient pyrexia on the first postoperative day and required no specific intervention. All patients started off-bed activities on postoperative Day 1, resumed bowel movement and oral intake on postoperative Day 3, and required no additional analgesics. Antituberculosis chemotherapy was started on postoperative Day 4, to which all patients responded well. Body temperature returned to normal in all patients with preexisting pyrexia 3–6 days after the antituberculosis treatment, and ascites regressed significantly in all patients by 7–15 days. No postoperative complications such as delayed gastrointestinal bleeding or perforation, surgical site infection, bowel obstruction, acute abdomen, secondary peritonitis, or extraperitoneal dissemination occurred. No bacterial growth was identified in the 6 patients having blood culture. The duration of postoperative hospitalization ranged from 14 to 24 days (mean, 19.4 days), and the total medical cost was Chinese Yuan ¥14,460–¥25,722 (U.S.$2313–$4116).
Follow-up results
Follow-up endoscopy showed well-closed gastric wall wounds and good wound healing with minimal scars at postoperative 2 weeks (Fig. 4) and 1 month, respectively. All patients were followed up as scheduled for 6–18 months, until the time this manuscript was drafted. None of the patients was lost to follow-up. All patients completed the antituberculosis chemotherapy with good compliance. TBP was considered cured in 7 patients and healed in 7 patients. No symptoms or signs suggestive of TBP relapse or extraperitoneal dissemination were reported. No patients experienced any treatment-related adverse events such as hepatotoxicity, neurotoxicity, or thrombocytopenia.
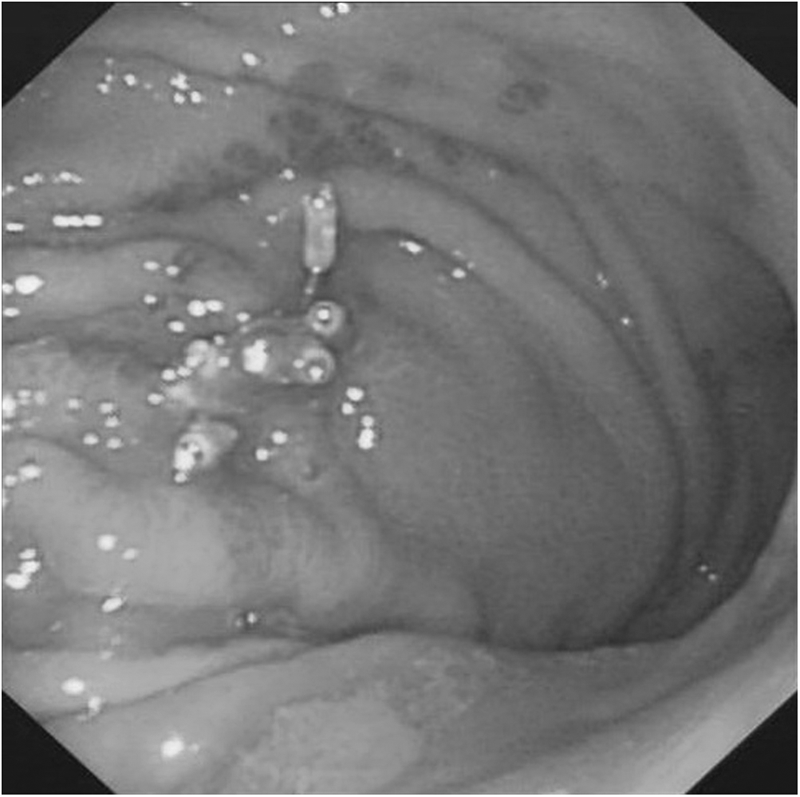
Follow-up endoscopy at postoperative week 2 showed a well-healed gastric wall wound with minimal scars.
Discussion
TBP, a common abdominal tuberculosis, has an indolent and variable disease course. It may go unrecognized and undiagnosed for months. Outside of China, in current practice about 70% of patients may present with nonspecific symptoms for up to 4 months before TBP is recognized. 26 Because of the high-level awareness of tuberculosis in the Chinese population, the mean time to diagnosis is less than 1 month.
Delayed or missed diagnosis of TBP may increase tuberculosis-associated morbidity, incur additional medical costs, and even result in treatment failure. 27 Standardized diagnostic workup protocols of TBP have been well documented in current literature and have focused mainly on the differentiation of ascites.28,29 Major investigational methods include ascitic fluid analysis and abdominal radiology, as well as tuberculosis-targeted microbiology, immunology, and molecular genetics. Clinical diagnosis of TBP can be established in most characteristic cases, and a 2-week empirical antituberculosis chemotherapy regimen can also be administered to suspected cases for the purpose of diagnosis. 30 Surgical biopsy can provide a definitive diagnosis in terms of pathology and bacteriology and remains the ultimate method to confirm the diagnosis of TBP. More important is that this technique can exclude the possibility of PC, in which the aforementioned noninvasive tests are less effective. In the present study, all our patients had significant elevation of cancer antigen 125 levels in ascitic fluid, which is a biomarker of advanced ovarian cancer 31 ; all other test results indicated a possibility of TBP. Therefore, peritoneoscopy with target biopsy was deemed necessary to exclude this possibility.
Multiple surgical approaches have been attempted to obtain a peritoneal biopsy adequate to differentiate TBP from PC in suspected cases. Laparotomic biopsy was historically used but is subject to serious complications. Radiology- or ultrasound-guided percutaneous peritoneal biopsy is a minimally invasive technique helpful for the differential diagnosis of TBP 32 but is only applicable for patients free of fibroadhesive disease. 33 Laparoscopic biopsy is more frequently used when TBP is suspected and has a sensitivity and specificity of 93% and 98%, respectively, as reported by a recent systematic review. 34 However, laparoscopic biopsy is not suitable for patients exhibiting massive intra-abdominal adhesions, which is often present in TBP patients. Additionally, although laparoscopy is minimally invasive, it is still subject to some complications, with a reported procedure-related morbidity rate of approximately 3% in patients with suspected TBP. 5 Major vessel injuries and intestinal perforations are very likely to occur in TBP patients with the fibroadhesive form. 35 In cases of exudative ascites, it is recommended that only an experienced laparoscopic surgeon perform a diagnostic laparoscopy. 5
Like laparoscopy, NOTES also allows a direct exploration of the entire peritoneal cavity and enables a guided biopsy of suspected peritoneal diseases. The characteristic appearance of TBP features as described by Bhargava et al. 23 on peritoneoscopy using NOTES is identical to that on laparoscopy, mainly consisting of thickened, hyperemic peritoneum with ascites; scattered, yellowish or whitish, granular, peritoneal nodules; and intra-abdominal fibroadhesive tissues. All our patients exhibited a mixture of the aforementioned macroscopic features on NOTES peritoneoscopy, enabling an endoscopic diagnosis of TBP that was confirmed by subsequent histology and bacteriology. To the best of our knowledge, we are the first group to report the use of NOTES for the differential diagnosis of TBP in patients exhibiting ascites of unknown etiology.
The advantages of NOTES for peritoneal biopsy, in contrast to laparoscopy, are that abdominal trocar incisions are avoided and therefore incision-related complications such as surgical site infection, non-healing wound, and incision hernia. This can further reduce surgical stress, minimize the risk of surgical morbidities, and accelerate postoperative recovery, especially in critically ill patients. 36 The shortened postoperative hospital stay will also relieve patients of psychomental stress and financial burden. 37 Moreover, no pneumoperitoneum, or only low-pressure peritoneum, is required in NOTES exploration, which is expected to be beneficial for patients. 38 Our patients showed a rapid postoperative recovery, free of any significant complications. Follow-up study found no wound contamination by M. tuberculosis, extraperitoneal tuberculosis dissemination, or disease recurrence.
The present study was limited by a small sample size (n=7), because of the experimental nature of NOTES. In addition, the retrospective study design is inevitably subject to selection and recall bias. Lastly, this was a noncomparative, single-arm study. The enrollment of a control patient cohort undergoing peritoneoscopy with laparoscopy would allow a direct comparison between NOTES and laparoscopy in terms of diagnostic effectiveness and safety.
It must be noted that a prospective clinical study of diagnostic NOTES peritoneoscopy showed that in patients undergoing laparoscopic gastrotomy at an anterior gastric site, the visualization of visceral organs located in the right upper and both lower quadrants was adequate, but that of organs in the left upper quadrant and spleen could be limited. 39 Other authors reported that NOTES, in its current form, seemed unsuitable for diagnostic laparoscopy in terms of organ visualization, lesion detection, and biopsy capability. 40 Another possible disadvantage of NOTES compared with laparoscopy is the relatively long operative time of NOTES peritoneoscopy, which may be associated with a stronger inflammation. However, a pilot animal (porcine) study showed that inflammatory stress was similar between NOTES and laparoscopy. 41 Bacterial contamination is also a major safety concern in the use of NOTES, as the natural orifices such as the mouth, anus, and vagina are colonized by normal microbial flora. However, a recent preclinical study comparing bacterial contamination of NOTES peritoneoscopy with biopsy and laparoscopy found no significant difference in peritoneal bacterial contamination. 42 Proper preoperative antisepsis antimicrobial prophylaxis is expected to reduce the bacterial load in all NOTES access approaches.
In conclusion, peritoneal biopsy using NOTES as an alternative to laparoscopy in TBP patients with ascites of unknown etiology is safe and effective. This technique offers an accurate and definitive diagnosis when combined with histology. NOTES is associated with a rapid postoperative recovery and minimal risk of complications. Our preliminary investigation shows that comparative studies to validate the advantages of NOTES over laparoscopy are warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.