
Abstract
Abstract
Aims:
The aims of this study were to develop a thin needle driver with multiple degrees of freedom and to evaluate its efficacy in multidirectional suturing compared with a conventional needle driver.
Materials and Methods:
The tip (15 mm) of the novel user-friendly needle driver (3.5 mm in diameter) has three degrees of freedom for grasping, rotation, and deflection. Six pediatric surgeons performed two kinds of suturing tasks in a dry box: three stitches in continuous suturing that were perpendicular or parallel to the insertion direction of the instrument, first using the novel instrument, then using a conventional instrument, and finally using the novel instrument again. The accuracy of insertion and exit compared with the target points and the procedure time were measured.
Results:
In the conventional and novel procedures the mean gaps from the insertion point to the target in perpendicular suturing were 0.8 mm and 0.7 mm, respectively; in parallel suturing they were 0.8 mm and 0.6 mm, respectively. The mean gaps from the exit point to the target in perpendicular suturing were 0.6 mm and 0.6 mm for conventional and novel procedures, respectively; in parallel suturing they were 0.6 mm and 0.8 mm, respectively. The procedure time for perpendicular suturing was 33 seconds and 64 seconds for conventional and novel procedures, respectively (P=.02); for parallel suturing it was 114 seconds and 91 seconds, respectively.
Conclusions:
Our novel needle driver maintained accuracy of suturing; parallel suturing with the novel driver may be easier than with the conventional one.
Introduction
Some articulating devices such as the da Vinci® Surgical System (Intuitive Surgical Inc., Sunnyvale, CA), KYMERAX (Terumo, Tokyo, Japan), Radius Surgical System and r2 drive (Tuebingen Scientific, Tuebingen, Germany), master–slave combined manipulator, 7 or 3-mm-diameter robot unit 8 were developed to overcome this problem, but none of these was a needle driver for neonatal laparoscopic surgery. The aims of this study were to develop a thin needle driver with multiple DOFs and to evaluate its efficacy in multidirectional suturing compared with a conventional needle driver.
Materials and Methods
Development of a needle driver
This was a collaboration project between the Department of Mechanical Engineering at the University of Tokyo and the Department of Pediatric Surgery at the University of Tokyo Hospital. In order to make it easy to perform multidirectional suturing, two additional DOFs for tip rotation and deflection were added to a conventional needle driver, which has only one DOF for grasping. The limited workspace in neonatal laparoscopic surgery necessitates the use of instruments with a small diameter and a short tip. Therefore, the diameter of the driver and the length of the tip were designed to be 3.5 mm and 15 mm, respectively. Specifications for the novel multi-DOF needle driver are shown in Table 1. An overview of the developed driver is shown in Figure 1a. The tip of the driver is cylindrical in shape, unlike a conventional scissors-type needle driver, and it has a slit in which a needle is fitted (Fig. 1b). The details of the mechanism were reported previously. 9 In brief, this slit is ordinarily closed by a piston, which is pushed by a spring, and opened by pulling a wire, which is attached to the piston, against the spring. The needle, which is fitted into the slit, is held by the force of the spring after the wire is loosened. The tip of the needle driver is rotated or deflected by moving two sets of geared mechanisms (Tecpha Japan Co. Ltd., Saitama, Japan), and the intersecting axes of motion facilitate intuitive tip positioning.
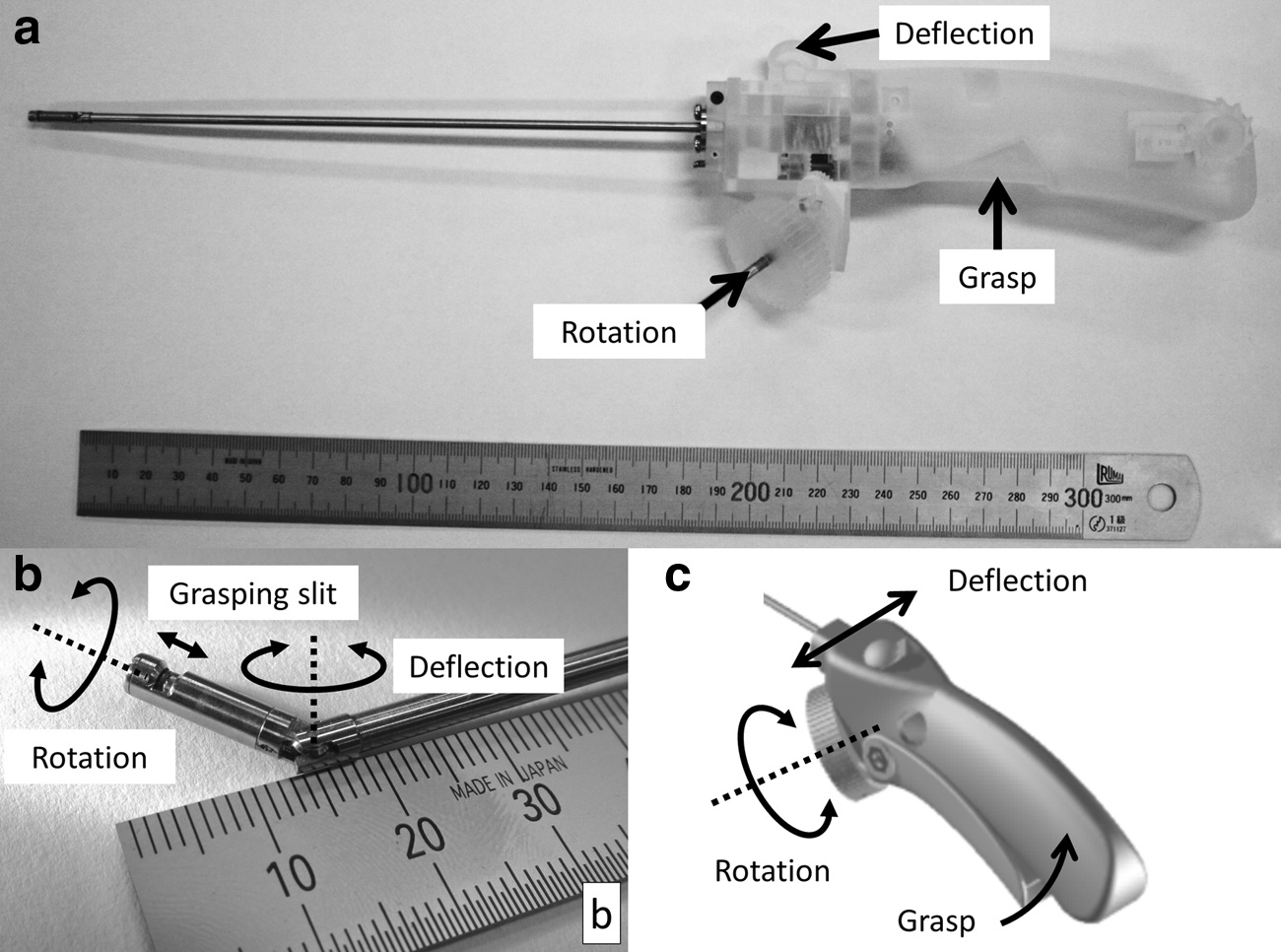
Overview and schema of the novel needle driver with 3 degrees of freedom.
An intuitive user-friendly interface was designed on the basis of our research 10 and implemented for this instrument. This interface was fabricated using a three-dimensional printer and does not require any electric devices such as motors (Fig. 1c).
Usability assessment
Experiments were conducted to evaluate the usability of this device compared with a conventional needle driver. The operators were six pediatric surgeons (three experienced surgeons, three trainees) who were asked to perform two kinds of suturing tasks on a sponge that was covered with latex in a dry box. One of the tasks was making three stitches in continuous suturing that were perpendicular to the insertion direction of the instrument, as well as three stitches that were parallel to the insertion direction (Fig. 2). Six dots were shown on the surface of the object, and the operator was required to target them in each insertion or exit of the needle. After instructions and practice in manipulating the novel needle driver, the operator was first asked to perform the tasks using the novel instrument, then by using a conventional one (3 mm in diameter; model K26167 FNS; Karl Storz GmbH & Co. KG, Tuttlingen, Germany), and finally by using the novel instrument again. The accuracy of insertion and exit was compared with the target points, and the procedure times were measured. A questionnaire was administered after the experiments. A comparative analysis was performed of the results of the conventional device and those of the second attempt of the novel device. Statistical analysis was performed by Student's t test using commercially available software (JMP™ 9.0.0; SAS Institute Japan Ltd., Tokyo, Japan). P values of <.05 were considered to be statistically significant.
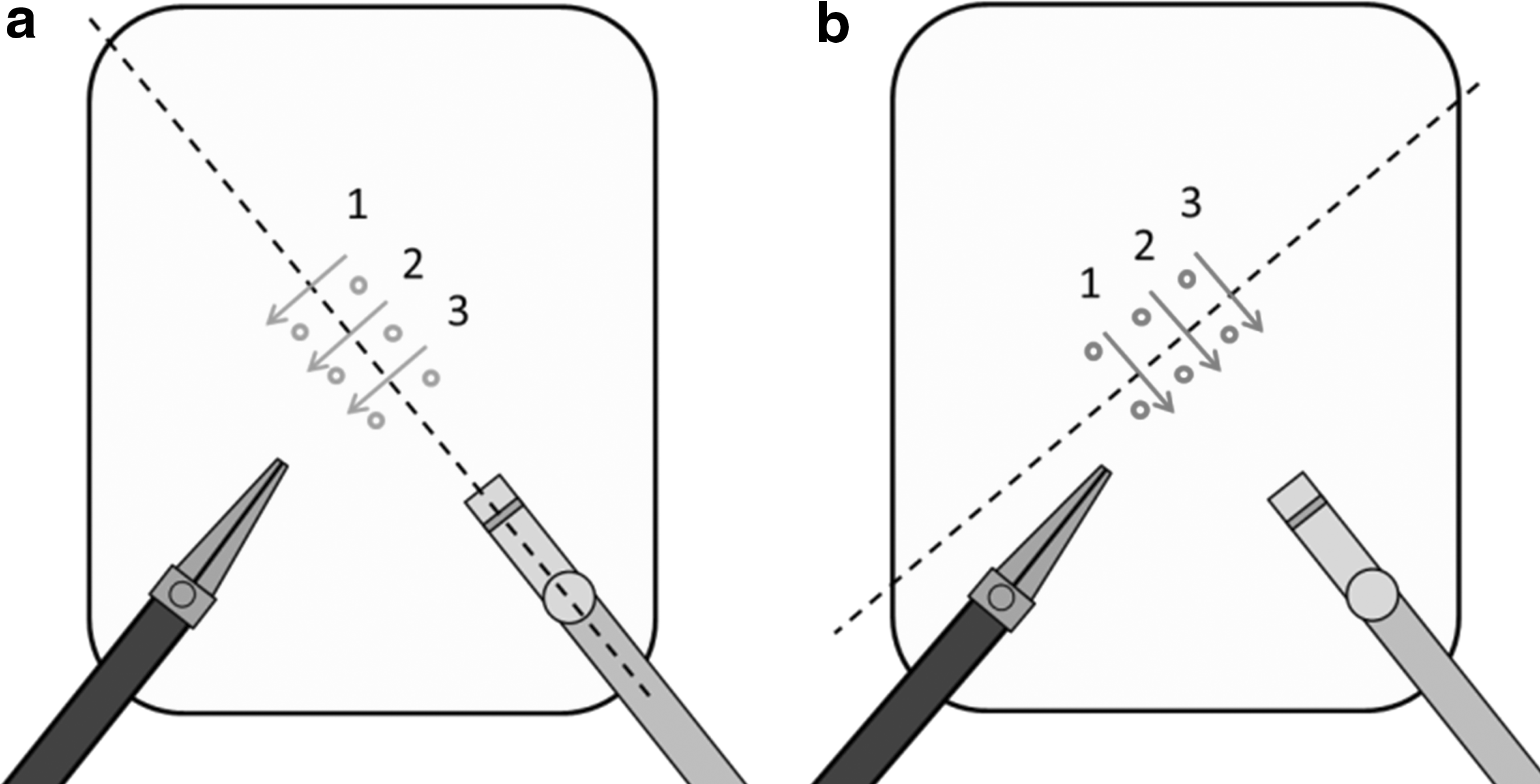
Schema of the tasks. The subjects were asked to make three stitches in continuous suturing that were
Results
The mean gap (standard deviation) values from the insertion point to the target in perpendicular suturing using the conventional needle driver and the newly developed needle driver were 0.8 (0.2) mm and 0.7 (0.2) mm, respectively, and those in parallel suturing were 0.8 (0.4) mm and 0.6 (0.3) mm, respectively. The mean (standard deviation) gap values from the exit point to the target in perpendicular suturing with the conventional and the novel needle drivers were 0.6 (0.3) mm and 0.6 (0.3) mm, respectively, and those in parallel suturing were 0.6 (0.3) mm and 0.8 (0.3) mm, respectively. There were no significant differences in accuracy of suturing between the two instruments (Fig. 3).
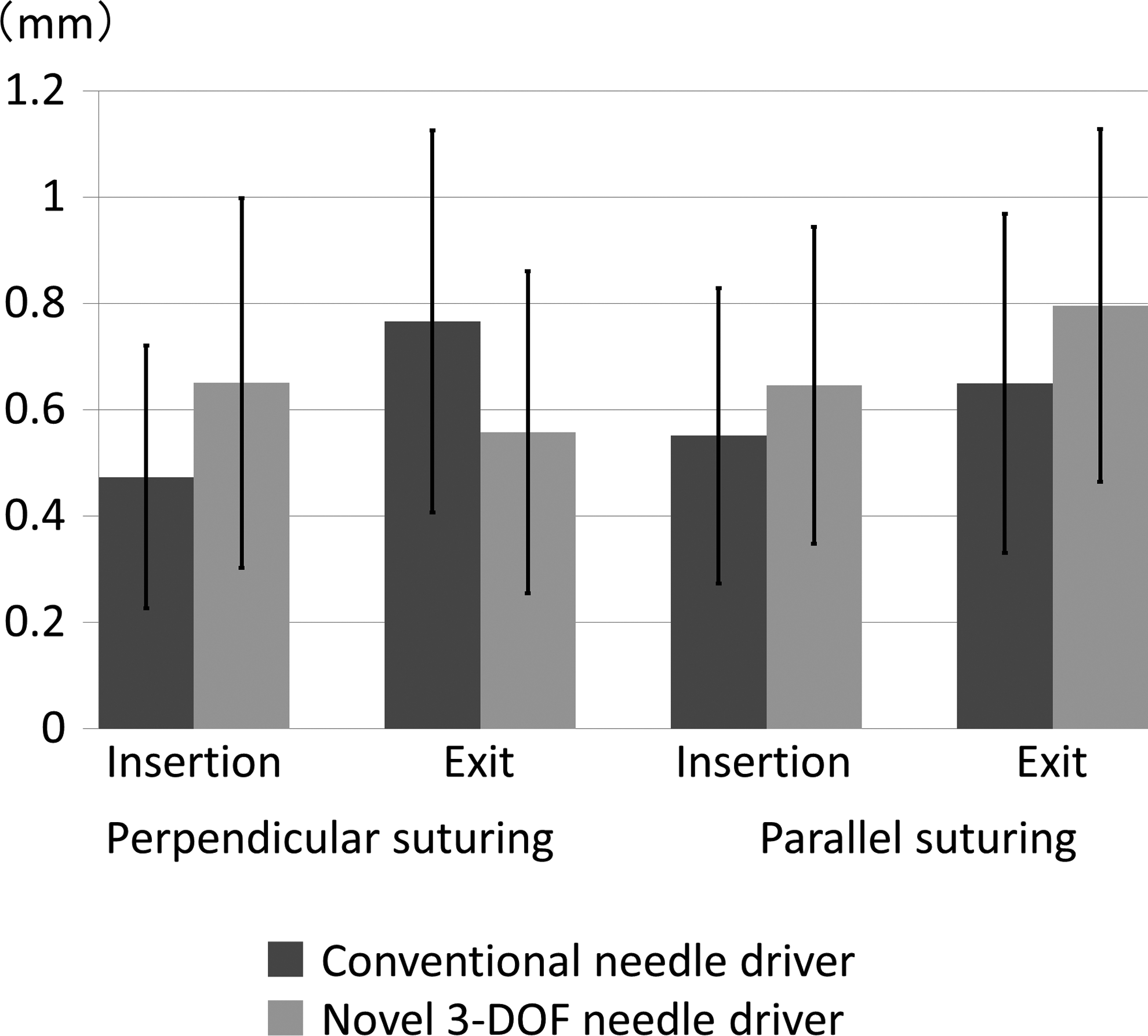
Accuracy of suturing. Gaps between an insertion point and a target point and gaps between an exit point and a target point were measured. There was no significant difference in accuracy of suturing between the two instruments, the conventional needle driver and the novel needle driver with 3 degrees of freedom (DOF).
The mean procedure time (standard deviation) of perpendicular suturing using the conventional driver was 33 (13) seconds, which was significantly shorter than that using the novel needle driver (64 [25] seconds) (P=.02). The mean (standard deviation) procedure time for parallel suturing using the newly developed 3-DOF needle driver (91 [26] seconds) was shorter than that using the conventional instrument (114 [42] seconds), but the difference between the two instruments was not significant (Fig. 4).
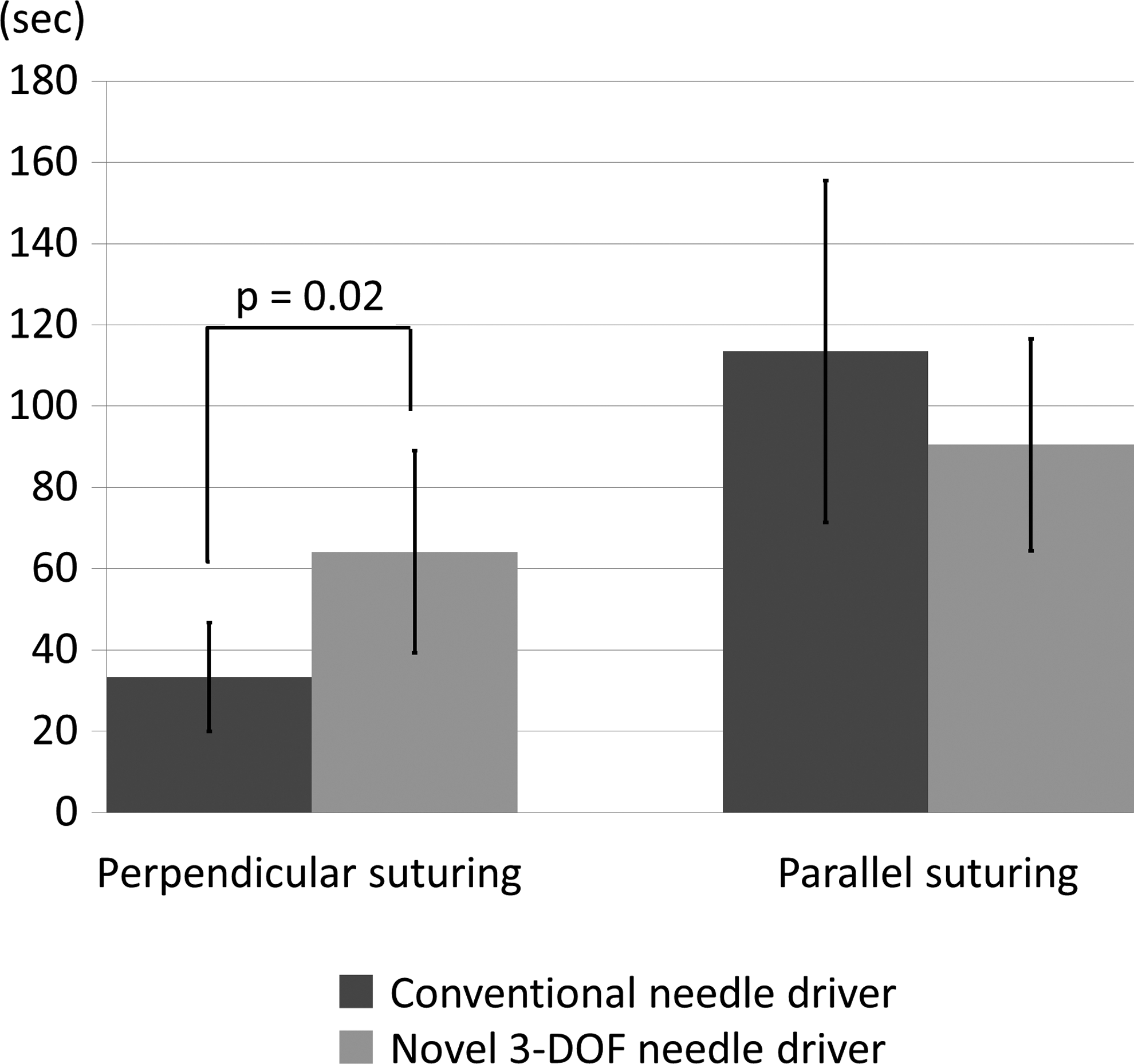
Procedure time. The procedure time for perpendicular suturing using the conventional driver was significantly shorter than that using the newly developed instrument, the novel needle driver with 3 degrees of freedom (DOF). Although the procedure time for parallel suturing using the novel 3-DOF needle driver tended to be shorter compared with that using the conventional instrument, there was no significant difference between the two instruments.
All but one surgeon answered that the new instrument was easy to use in perpendicular suturing, and the remaining one said that the usability of the novel device and the conventional device was the same. Two of the three experienced surgeons preferred to use the conventional device in parallel suturing, but the other experienced surgeon and the three trainees answered that the novel needle driver was superior to the conventional one.
Discussion
We developed the novel needle driver for neonatal laparoscopic surgery in order to perform multidirectional suturing easier. This instrument has several characteristics. First, the tip of the instrument has 3 DOFs for deflection, rotation, and grasping. Second, the shaft has a small diameter. Third, the tip of the instrument is short. Finally, the interface is intuitive and user-friendly.
Several multi-DOF devices have already been used in adult clinical practice and have helped to overcome challenging situations in which it was difficult for surgeons to perform certain procedures by using conventional straight 1-DOF devices. However, as far as we know, there is no multi-DOF needle driver that is commercially available for neonatal endoscopic surgery. It is clear that adding 2 DOFs for rotation and deflection to the conventional needle driver makes multidirectional suturing easier. So, downsizing the device was an essential as well as difficult issue in developing the novel device. Lee et al. 11 evaluated the influence of instrument size on endoscopic task performance and concluded that smaller instruments were better in neonatal or infant surgery. However, simple miniaturization of devices does not always achieve the goal because there is a possibility that strength or motion stability of the devices is lost owing to their extreme downsizing. Actually, we initially tried to develop a scissors-type needle driver. Motions of its prototype were smooth and stable and satisfied requirements. We could hold a needle, but the grasping force was too small to do suturing. So, we were forced to think of a new mechanism for secure grasping and developed the piston-type needle driver. The way of holding a needle and applying ligatures by using the piston-type instrument are slightly complicated compared with a scissors-type instrument; however, from our experiences, it seems that a surgeon with basic laparoscopic skill does not take a long time to master manipulation of our novel instrument.
The usability assessment showed that the novel needle driver did not affect the accuracy of suturing. Looking into surgeons' performance in detail, they all made stitches without rotating or deflecting the tip of the 3-DOF needle driver in perpendicular suturing, as if they used the conventional needle driver. In parallel suturing with the conventional needle driver, some surgeons used a left-handed forceps to assist the suturing by pushing an object strongly. Moreover, some stitches were completed by passing a thread through an extremely superficial layer of the object. These acts should be avoided in neonates, whose tissues are very fragile, and our 3-DOF needle driver may be effective in this respect.
The mean procedure time in parallel suturing using the novel needle driver tended to be shorter than that using the conventional one, but there was no significant difference between the two instruments. There was a concern that the operators were still on the learning curve and not familiar with using the 3-DOF piston-type needle driver. If we would spend more time on practicing how to use it, we might be able to see a significant difference in procedure time between the two instruments.
In the questionnaire answered after the experiments, all but one surgeon said that the usability of the novel device and the conventional device was the same in perpendicular suturing. Two of three experienced surgeons preferred to use the conventional device in parallel suturing, but the other experienced surgeon and the three trainees answered that the novel needle driver was superior to the conventional one. These results suggested that this needle driver could be used like a conventional needle driver in perpendicular suturing and that it made parallel suturing easier than with the conventional driver. In addition, this instrument may be useful especially for novice surgeons.
Further studies on the trajectory of the needle, force acting on the object, or multidirectional suturing on a vertical surface may show the significant usefulness of our thin 3-DOF needle driver. Examining a learning curve for this instrument is also required in the future.
Footnotes
Acknowledgments
This study was supported by Grant-in-Aid for Scientific Research (B) number 21390473 and Grant-in-Aid for Scientific Research (S) number 23226006 from the Ministry of Education, Culture, Sports, Science and Technology of Japan.
Disclosure Statement
No competing financial interests exist.