
Abstract

Dear Editor:
In a prospective randomized trial the authors concluded, with a very small sample size and using a nonstandard hybrid technique for cholecystectomy, that there is no difference between laparoscopic cholecystectomy (LC) and mini-cholecystectomy (MLC). The authors have systematically used a 5-mm trocar outside the umbilicus and a drain, something that really goes against the scope of minimizing trauma. 1 There are two main standard techniques for MLC, with over 1000 cases published, and none of them used trocars with a diameter greater than 3 mm outside the umbilical site.2–4 The proposed technique can be suggested as a hybrid between minilaparoscopic and laparoscopic techniques because the authors used, in a routine basis, a 5-mm port outside the umbilicus. In most MLC series, the use of a 5-mm port out of the umbilicus is considered a conversion to LC.2–4
Most of the published works were ineffective in proving differences between LC and MLC,5–7 but unfortunately none was performed using the new low-friction minilaparoscopic instruments, which can improve dexterity and cosmesis. 8 Another issue to be addressed in this article is the routine use of prophylactic drains for elective cholecystectomy, which usually are unnecessary and in fact can be responsible for an increase in costs and postoperative pain and worsen the cosmetic result, especially if a 5-mm port is used. 1
The advent of natural orifice translumenal endoscopic surgery (NOTES®; American Society for Gastrointestinal Endoscopy [Oak Brook, IL] and Society of American Gastrointestinal and Endoscopic Surgeons [Los Angeles, CA]) and subsequently laparoendoscopic single-site surgery (LESS) has called the attention of surgeons to look for even less invasive modalities of surgical access.9–11
Minilaparoscopy (MINI) is a natural advancement of laparoscopy, which proposes to diminish surgical trauma by reducing the diameter of the standard laparoscopic instruments without losing range of motion in triangulation, important aspects that can be a major issue in NOTES and LESS. MINI was first described more than 15 years ago and is not really a new modality of access,12,13 but needs to be carefully revisited because several aspects have changed over this period of time:
New instruments were developed, much better designed and with more resistant materials, which are now giving a totally new face to MINI
8
(Fig. 1). In procedures where enhanced visualization in a restricted space is necessary, MINI offers advantages over regular laparoscopic surgery (for example, for mini-total extraperitoneal inguinal hernia repair, mini-lumbar or thoracic sypmpathectomies, mini-common bile duct exploration/reconstructions, and tranasanal endoscopic operations)14–16
(Fig. 2). When it is necessary to suture or even just to tie a knot, the enhanced precision of the new low-friction MINI instruments can have advantages in their handling over the conventional 5-mm equipment that uses rubber sealing and valves that can preclude some amplitude of movement
8
(Fig. 1).

Views from transanal endoscopic microsurgery with neodermal simulation.
MINI is no longer an experimental procedure, and it is here to stay. As a matter of fact, one may say that the MINI has returned to stay: the same MINI that Michel Gagner, Peter Goh, and co-workers described on the 1990s,12,13 which did not become popular because the instruments were deemed too flimsy and surgeons were not used to working with very thin, fragile, and expensive scopes. Moreover, surgeons insisted on clipping every structure from the umbilical port, which resulted in changing the scope several times in a single procedure, making MINI not only complicated, but also boring and time consuming.12–14 Stigmatized as an expensive and complicated surgery, at that time MINI seemed to have no major advantages and did not progress the way industry had imagined, and many thought had been relegated to a footnote in the surgical texts. 14
With some minor adjustments in the technique, what we have named the clipless cholecystectomy technique, we could overcome the problems of the MINI optics simply by tying knots to the cystic duct and cautherizing the cystic artery.2,14,17 This technique has been described in detail in a publication of 1000 cases 2 (a series that now surpasses 1700), without mortality, conversion to open surgery, or common bile duct injuries. Using the new MINI instruments we could safely complete more than 97% of cases with purely mini-instruments. In the case of placement of even one 5-mm trocar (what is considered standard by the authors of the article under discussion 1 ), we have considered it to be a conversion to LC.1,2 In order to avoid the use of mini-scopes, all gallbladders were removed in a bag, and most of our patients were discharged in less than 24 hours with virtually no pain. Currently, MINI clipless is a 1-day surgery, safe, with all the advantages of laparoscopy, highly reproducible, cost-effective, and with great esthetic appeal2,14,17 (Fig. 3).
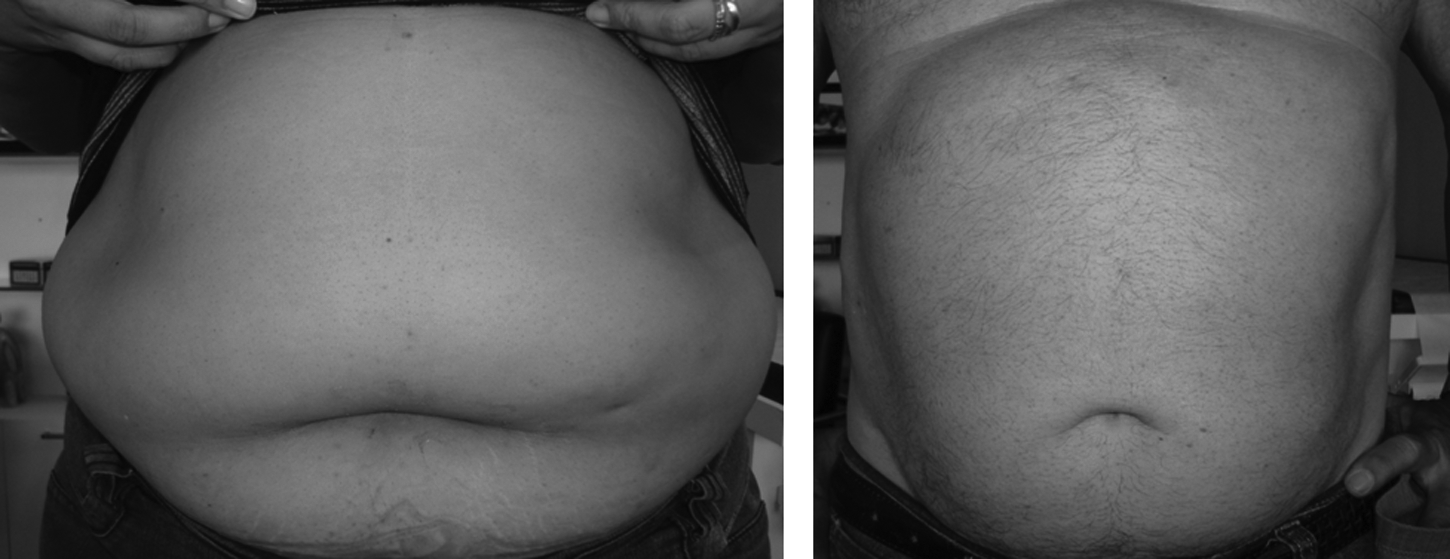
Mini-scars (3.5-mm trocar) on unselected average cholecystectomy patients after
Another great advantage of the MINI approach that usually is forgotten by many authors, who really want to address only the cosmetic issue, is the enhanced view. A surgeon who uses MINI can work much closer to the subject without being disturbed by the 5-mm forceps. Mathematically speaking, we can find gains up to 2.7 times in magnification when using MINI instruments, as the thinner instruments occupy less of the visual field14–17 (Fig. 2).
In endoscopic surgery, peripheral vision is limited by the visual field of the laparoscope. In this tunnel vision, thinner instruments occupy less space, and a much better view can be obtained. MINI instruments fit well into the concept of amplified vision provided by laparoscopes. The increase in vision scale seen in laparoscopy does not find a perfect partnership with conventional 5-mm instruments, and they become coarse instruments for dealing with more delicate situations, such as biliary anastomosis, resection of a sympathetic ganglion adherent to the vena cava, or dissection of the deferens duct from the hernia sac during hernia surgery.14–17 This is especially important in retroperitoneal surgeries, where the space is naturally restricted and inadvertent movements may result in peritoneal perforations, thus causing gas escape and further space reduction. Another great application for the new low-friction mini-instruments is in tranasanal endoscopic operations, where an enhanced view and more freedom of movements can be experienced. 15 More delicate surgeries should be preferably done by MINI because you can get better vision and work with more precision owing to the thinner instruments14–17 (Fig. 2).
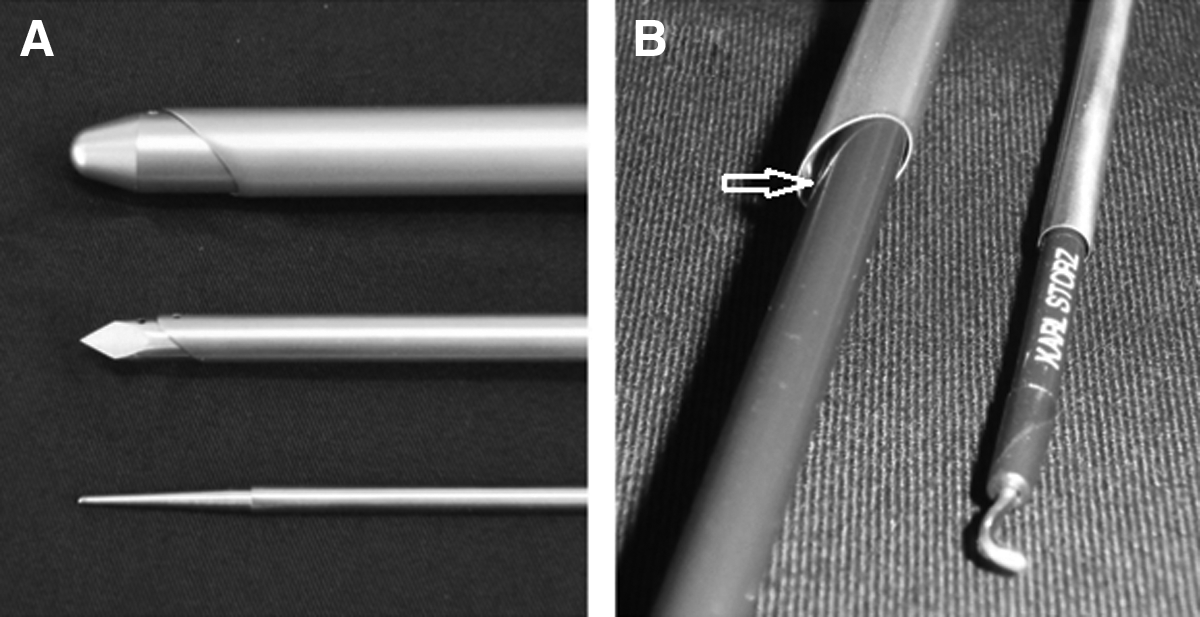
Current technical limitations of MINI are being solved by the efforts of the industry in crafting more resistant and higher-performing instruments. Longer trocars without sealing (low friction) help to stabilize mini-forceps and increase the strength and durability of the mini-equipment without limiting surgical movements. 8 Even though MINI instruments are more delicate, when properly used they do not need much more maintenance than standard 5-mm laparoscopy instruments. Current low-friction MINI trocars (unlike their ancestors from the 1990s) do not have a sealing membrane (what can be called “no rubber” or “low-friction” trocars) (Fig. 4). They have very low friction, and therefore almost no force is needed to move the instruments inside the trocars, which prevents undesirable movement and eventually the total trocar displacement of the trocars, injuring the skin and worsening cosmesis. Another important aspect of the new MINI trocars is that they have a ball-shaped dilating tip with a very imperceptible smooth transition between the tip and cannula, allowing for a minimal skin incision by radially dilating the skin, muscle layers, and fascia. Adding this to the absence of friction with the rubber, there is no dislocation of the trocar during operation and, hence, improved cosmesis at the site of penetration of the trocar8,14 (Fig. 3).

Mini-trocar insertion (low-friction mini-trocar with dilating tip).
The ball-shaped tip introducer also helps to minimize injuries to vessels and nerves when the trocar is introduced gently, by dissecting/splitting instead of cutting. There is an extra precise fit between the instrument and the cannula, resulting in extremely reduced friction and minimal gas leakage (<0.1 L/minute). The increase in CO2 leak, formerly regarded as a reason for criticism, but actually without any real consequence in the performance of the procedure, is being successfully corrected by these new trocar models8,14 (Fig. 4).
In brief, there is much more than ”just a pretty face” to be emphasized when evaluating the benefits of actual minilaparoscopic surgery (Fig. 3). Gains that can go far beyond the cosmesis (only proven gains so far of single-port surgery and LESS), including less abdominal wall trauma, more precise surgical movements, enhanced view, and better dexterity, without significantly increasing the operative time, surgical effort, or costs and, the most important of all, without compromising the standards of surgical safety.14–21
Footnotes
Disclosure Statement
G.L.C. is a consultant, without financial interest, for Karl Storz for the development of the new minilaparoscopic low-friction trocars. L.T.C. and P.R. have no disclosures relevant to this article.