
Abstract
Abstract
Background:
It remains controversial whether laparoscopy-assisted total gastrectomy (LATG) is a safe or better alternative to open total gastrectomy (OTG) for the treatment of gastric cancer. We aimed to evaluate the safety and efficacy of LATG by pooling comparative studies of LATG and OTG in a meta-analysis.
Materials and Methods:
Original articles comparing LATG and OTG for gastric cancer, published in the English language since 1990, were searched for in PubMed, Embase, Medline, and the Cochrane Library. The outcome variables analyzed were number of harvested lymph nodes, postoperative complications, postoperative mortality, 5-year survival, operative time, blood loss, time of analgesic use, first flatus day, and postoperative hospital stay.
Results:
Eight studies were considered suitable for the meta-analysis, for a total of 1161 patients (409 LATG and 752 OTG). Compared with OTG, LATG showed a similar number of lymph nodes harvested, morbidity, and postoperative mortality. There was also no difference in 5-year overall and disease-specific survival between groups, according to two enrolled studies where such data were available. LATG required longer operative times than OTG but also resulted in significantly less blood loss, earlier return of bowel function, less time of analgesics use, and shorter postoperative hospital stay.
Conclusions:
This meta-analysis suggests that LATG in the treatment of gastric cancer is similar in safety and efficacy to OTG. LATG has the advantages of less blood loss and faster postoperative recovery, at the expense of a longer operative time.
Introduction
We aimed to determine the safety and efficacy of LATG by pooling comparative studies of LATG and OTG in the treatment of gastric cancer.
Materials and Methods
Types of studies
All published English language studies comparing LATG and OTG with curative intent for gastric adenocarcinoma were evaluated. Included studies were required to clearly state the technique used. If multiple similar studies by the same author(s) were found, only the most recent or the most informative were included. Two reviewers extracted data independently.
Inclusion criteria and exclusion criteria
Patients were all diagnosed with gastric cancer, as proven by biopsy. The intervention group underwent LATG, and the control group underwent OTG. During either approach, inclusion criteria included sparing of the spleen. Any extent of lymphadenectomy from D1 to D2 and any pattern of reconstruction were acceptable.
All potentially included studies were required to report at least one or more of the considered outcome measures. There were no limitations for race, age, or sex.
Studies that did not conform to the above criteria or where essential data could not be extracted were excluded. For example, studies on LATG accompanied by a splenectomy or on hand-assisted total gastrectomy were not included.
Outcomes of interest
Outcomes measured were:
1. Primary: number of harvested lymph nodes, rate of postoperative complications, (including anastomotic leak, stenosis, wound complications, etc.), operative mortality, and survival rate 2. Secondary: operative time (minutes), intraoperative blood loss (mL), time of first flatus (days), time of analgesics use, and postoperative hospital stay (days)
Literature search
A comprehensive literature search was performed in the PubMed, Embase, Medline, and Cochrane Library databases for English language-only studies comparing LATG and OTG published since 1990. The following search terms were used: “laparoscopic,” “laparoscopic assisted,” “laparoscopy-assisted,” “total gastrectomy,” and “gastric cancer.” MESH terms and the function of explosion search were also used to broaden the search. The last literature search was performed on January 17, 2013. Details on the literature search and selection process are listed in Figure 1.
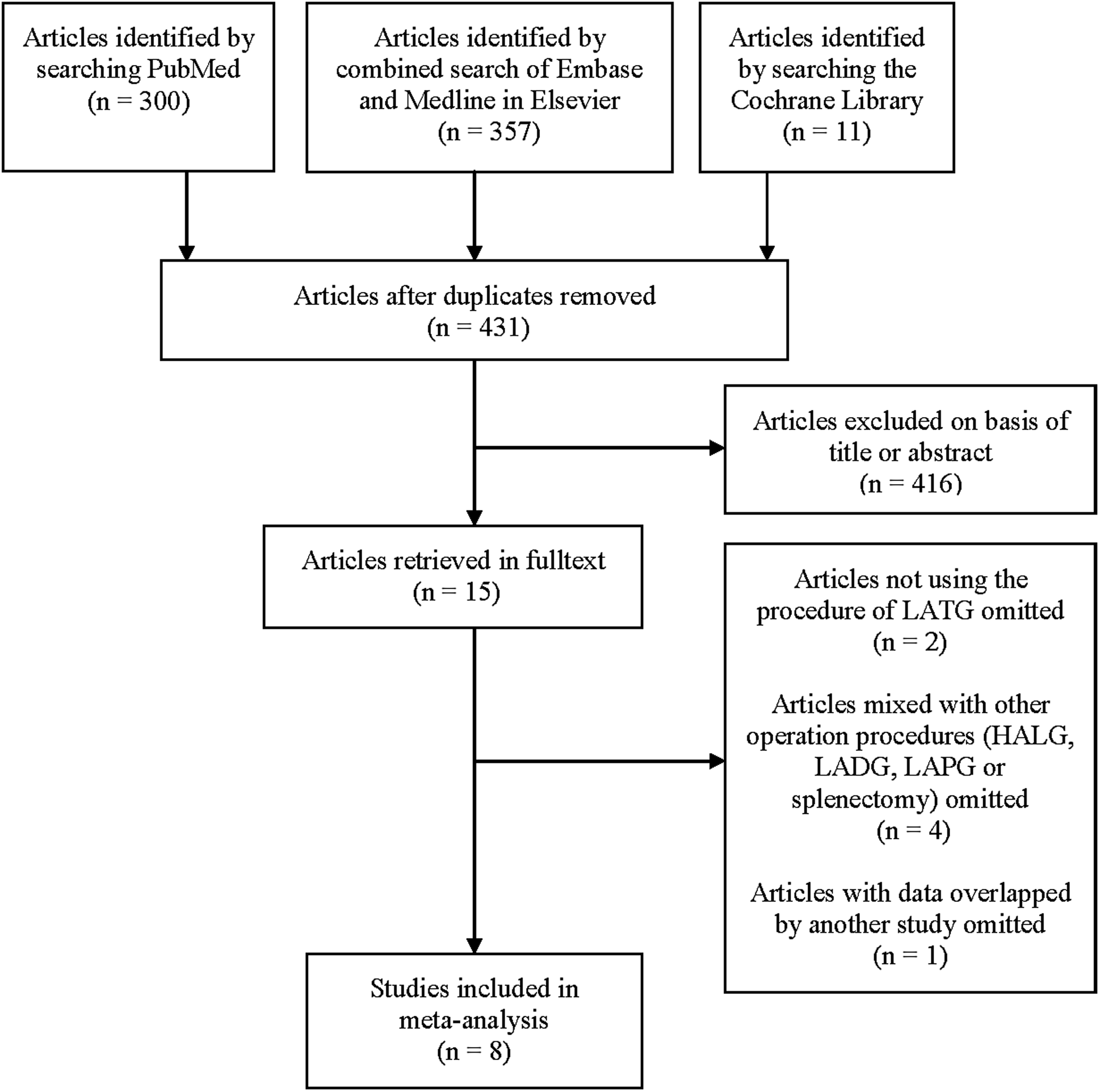
Literature search and selection process. HALG, hand-assisted laparoscopic gastrectomy; LADG, laparoscopy-assisted distal gastrectomy; LAPD, laparoscopy-assisted proximal gastrectomy; LATG, laparoscopy-assisted total gastrectomy.
Selection, data collection, and quality assessment
Selection of studies, quality assessment, data extraction, and statistical analysis were completed by two independent reviewers (H.S. and M.Q.). General data extracted included publication year, sample size, patient demographics, and intervention details. Abstract data for primary and secondary outcome measures mentioned above were extracted. Abstracted data, including total number of participants and events for each group, were extracted as dichotomous variables. For the continuous variables, the mean, standard deviation, and total number of participants for each group were extracted concurrently.
Quality assessment of the included studies was based on the Newcastle–Ottawa Scale system12–14 with some modifications to match this study. A star rating of 0–14 was assigned to each included study based on the criteria listed (see the footnote to Table 1). Studies that obtained 11 or more stars were regarded as high-quality studies and were used for subgroup analysis.
Features matching between laparoscopy-assisted total gastrectomy (LATG) and open total gastrectomy (OTG): 1, age; 2, sex; 3, body mass index; 4, comorbidities; 5, American Society of Anesthesiologists score; 6, tumor size; 7, histological type; 8, depth of invasion; 9, lymph node metastasis; and 10, lymphadenectomy.
Outcomes of interest: 11, operative time; 12, blood loss; 13, number of harvested lymph nodes; 14, time of flatus; 15, time of analgesics use; 16, length of postoperative hospital stay; 17, complications; 18, postoperative mortality; 19, 5-year overall (cumulative) survival rate; and 20, 5-year survival rate.
Rating system: for selection, 1=Any inclusion criteria reported? (if yes, one star), 2=How representative was the patients undergoing LATG to population undergoing surgery for gastric cancer? (if yes, one star), 3=How representative were patients undergoing OTG to population undergoing surgery for gastric cancer? (if yes, one star); for comparability, 1=group comparable for (1) age, (2) sex, (3) body mass index, (4) comorbidities or American Society of Anesthesiologists score, (5) tumor size, (6) histological type, (7) depth of invasion, and (8) lymph node metastasis (one star was assigned for each of these eight characteristics if there was no difference between the two groups); and for outcome assessment, 1=outcome clearly recorded (yes, one star; two stars if seven or more outcomes were reported) and 2=adequacy of follow-up (one star if 5-year survival data were available in over 90% of patients).
High-quality study.
F, female; M, male; R, retrospective study; RC, retrospective cohort study.
Funnel plots were constructed to detect publication bias in this meta-analysis by plotting standard error against treatment effect, as mean difference or log (odds ratio [OR]), for outcome variables with Reviewer Manager (RevMan) version 5.1 software (Cochrane Collaboration, Oxford, UK). Any discrepancies in quality assessment and data collection were discussed between the two reviewers until consensus was obtained.
Statistical analysis
This meta-analysis was conducted in accordance with recommendations from the PRISMA statement. 15 Outcomes of eligible studies were statistically synthesized by RevMan version 5.1 software. Pooled statistics were calculated using a fixed effects model initially. Effect sizes, OR, and mean difference were reported for dichotomous and continuous data, respectively. The OR represents the odds of an event that occurred in the treatment group (LATG) compared with the reference group (OTG). An OR of <1 favors the LATG group, except in the case of survival, where the opposite is true. The point estimate of the OR is considered statistically significant with a P value of <.05 if the 95% confidence interval (CI) does not cover the value one. The Mantel–Haenszel method was used to combine the OR for the outcomes of interest, and the inverse variance method was used to test the significance of continuous data.
Heterogeneity between comparable studies was tested in all analyses using the chi-squared test. If gross statistical heterogeneity exists, then analysis was carried out by the random effects mode.
Results
Studies selected
Eight studies published between 2008 and 201216–23 were eligible for analysis. Of a total of 1161 patients, 409 (35.2%) underwent LATG, and 752 (64.8%) underwent OTG. All patients underwent total gastrectomy in either approach without splenectomy. The extent of lymph node dissection ranged from D1+α/+β to D2. The search and exclusion strategy is shown in Figure 1. Consensus of the two reviewers was obtained wherever necessary. Demographic characteristics of included studies and quality assessment results are listed in Table 1. Four studies16,18–20 ranked 11–12 stars in quality assessment were used for subgroup analysis.
Primary outcomes
Lymph node clearance
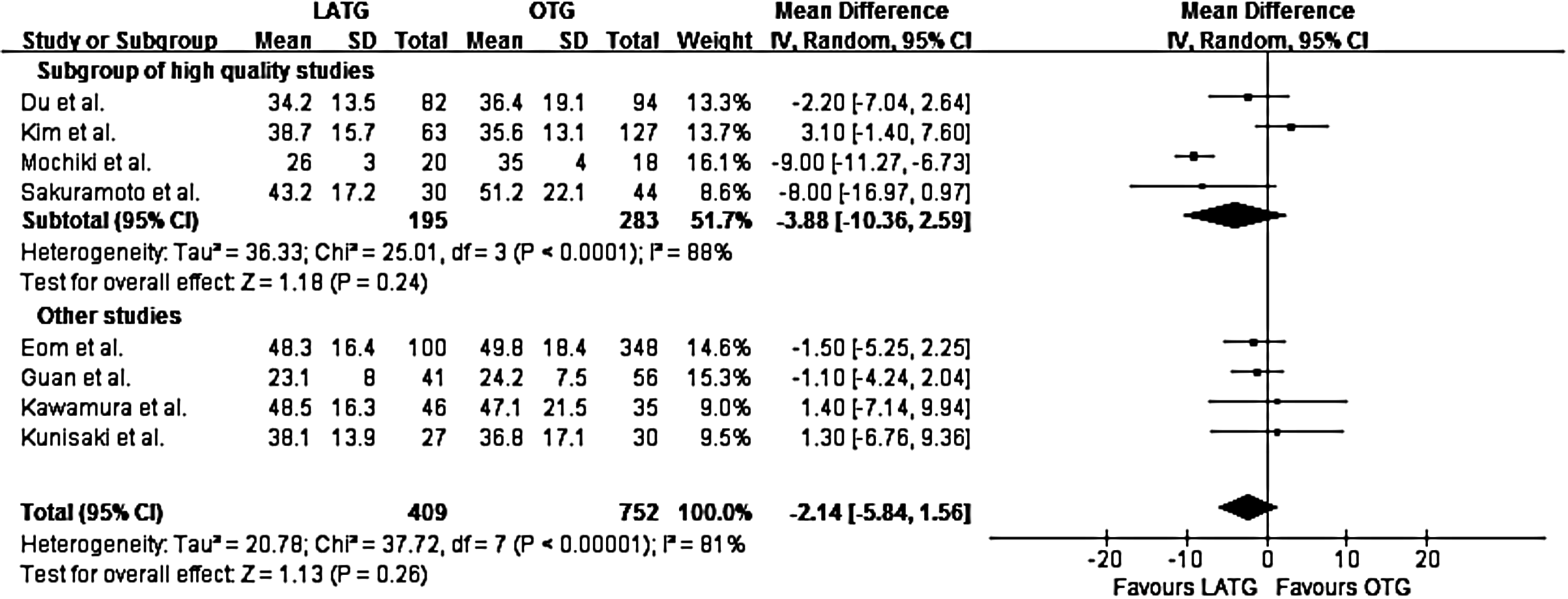
Data on the extent of lymphadenectomy from all eight studies were analyzed. The mean number of harvested lymph nodes ranged from 23.1 to 48.5 in the LATG group versus 24.2 to 51.2 in the OTG group. Overall analysis showed that a mean of 2.14 fewer lymph nodes was harvested in LATG than in OTG, but this difference was not found to be statistically significant (P=.26, 95% CI −5.84 to 1.56, Z=1.13). Subgroup analysis of high-quality studies demonstrated the same result (Fig. 2).
Postoperative complications
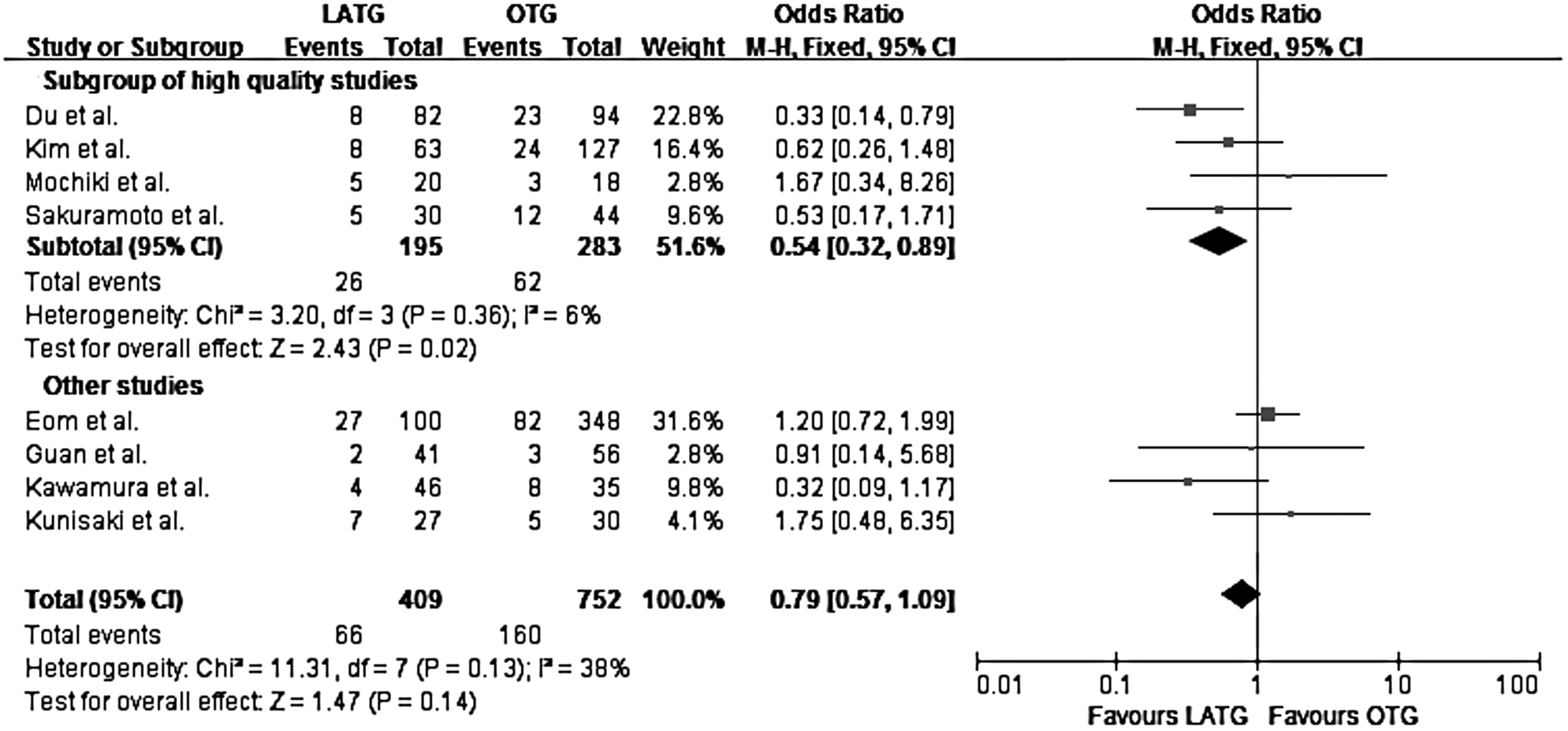
When data of all studies were pooled, the postoperative complication rate was 16.1% (66/409) in the LATG group versus 21.3% (160/752) in the OTG group. The overall rate of postoperative complications in LATG was statistically similar to that in OTG (OR=0.79, P=.14, 95% CI 0.57 to 1.09, Z=1.47). However, in the subgroup of high-quality studies, the overall postoperative complication rate was significantly lower in LATG than in OTG (OR=0.54, P=.02, 95% CI 0.32 to 0.89, Z=2.43) (Fig. 3).
There was no difference in incidence of anastomotic leak and stenosis, wound complications, pancreatic leak, and pneumonia (Table 2).
1, Mochiki et al. 16 ; 2, Kawamura et al. 17 ; 3, Sakuramoto et al. 18 ; 4, Du et al. 19 ; 5, Kim et al. 20 ; 6, Eom et al. 22 ; and 7, Guan et al. 23 The study of Kunisaki et al. 21 was not included as this study did not provide data for individual complications.
When the P value was less than .05 in the test for heterogeneity, the random effects model was used for meta-analysis; otherwise, the fixed effects model was applied.
CI, confidence interval; LATG, laparoscopy-assisted total gastrectomy; OTG, open total gastrectomy.
Postoperative mortality
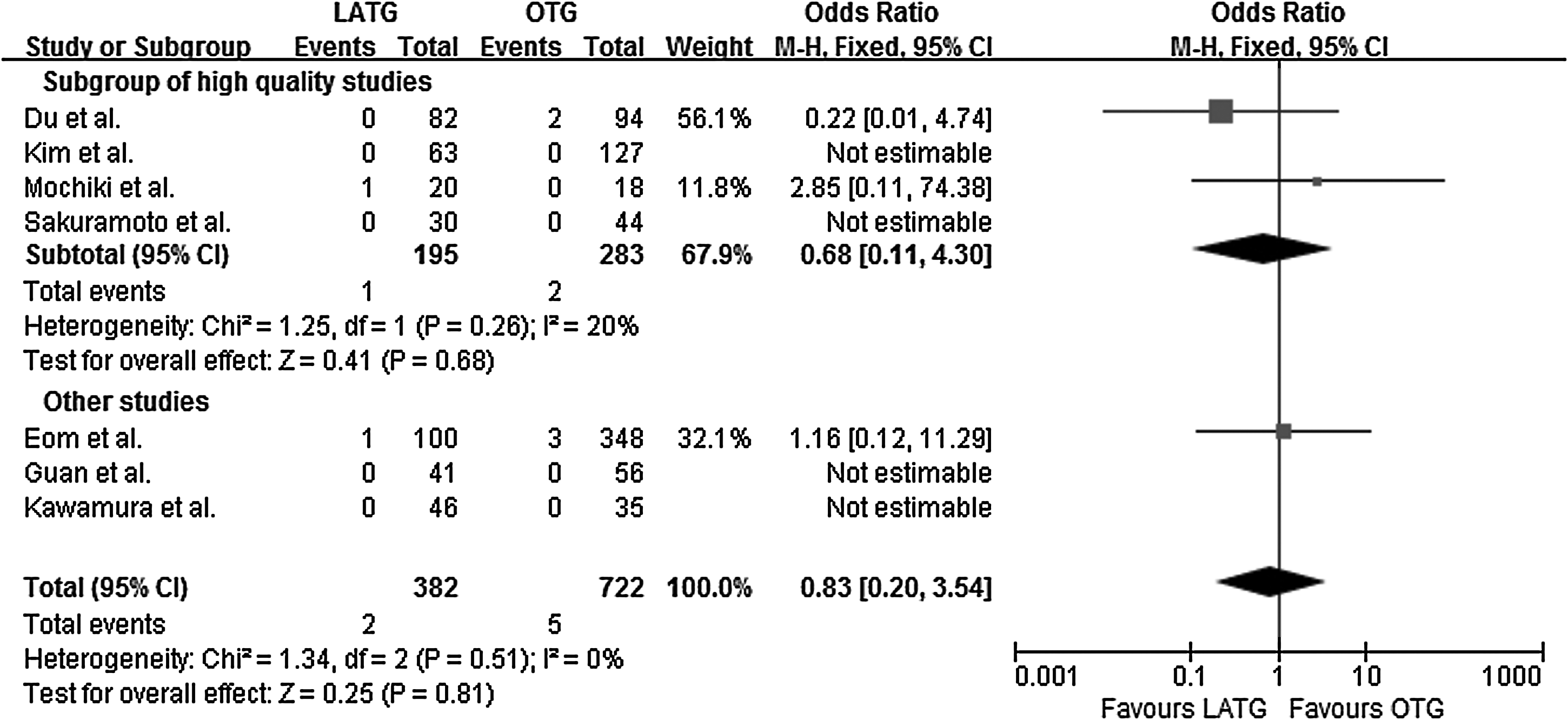
Mortality was rare in both groups and not significantly different between LATG and OTG (OR=0.83, P=.81, 95% CI 0.20 to 3.54, Z=0.25). There were two mortalities in the LATG group and five in the OTG group. Subgroup analyses yielded similar results (Fig. 4).
Survival rate
Two studies16,21 compared 5-year overall (cumulative) survival of LATG and OTG, which was 96.2% versus 64.1% in the study of Kunisaki et al. 21 and 95% versus 90.9% in the study of Mochiki et al., 16 respectively, with no statistical difference between the two studies. The same was true for 5-year disease-specific survival (100% versus 72.7% in the study of Kunisaki et al. 21 and 100% versus 91.7% in the study of Mochiki et al., 16 respectively).
Secondary outcomes
Operative time and intraoperative blood loss
Mean operative time ranged from 150.8 to 291.9 minutes in the LATG group versus 131.2 to 272.1 minutes in the OTG group. LATG took 41.06 minutes longer than OTG (P=.0001, 95% CI 20.37 to 61.75, Z=3.89).
Mean blood loss in the LATG group ranged from 54.9 to 299 mL versus 272.7 to 758 mL in the OTG group. An average of 253.17 mL less blood loss was seen in LATG (P=.00001, 95% CI −340.40 to −165.95, Z=5.69). Analysis of the subgroup of high-quality studies demonstrated similar results in these two variables (Table 3).
Studies ranked 11 or more stars in quality assessment were used for subgroup analysis.
1, Mochiki et al. 16 ; 2, Kawamura et al. 17 ; 3, Sakuramoto et al. 18 ; 4, Du et al. 19 ; 5, Kim et al.20] ; 6, Kunisaki et al. 21 ; 7, Eom et al. 22 ; and 8, Guan et al. 23
When the P value was <.05 in the test for heterogeneity, the random effects model was used for meta-analysis; otherwise, the fixed effects model was applied.
CI, confidence interval; WMD, weighed mean difference.
Postoperative recovery
Mean time to flatus was 1.9–4.1 days in the LATG group and 3–5.3 days in the OTG group. Time to flatus was 0.90 days earlier in LATG (P=.004, 95% CI −1.53 to −0.28, Z=2.85). The LATG group required a mean of 3.5–6.8 times analgesia use versus 5.3–11.8 times in OTG. LATG required 2.55 less times of analgesia use (P<.00001, 95% CI −3.15 to −1.95, Z=8.36). Subgroup analysis demonstrated similar results in these variables.
Patients in the LATG group had a mean length of postoperative hospital stay of 8.1–19 days versus 9.6–29 days in the OTG group. Pooled data showed that LATG patients had a mean length of postoperative hospital stay that was 4.08 fewer days compared with OTG patients (P=.001, CI −6.59 to −1.57, Z=3.18). No difference between the two approaches was found in subgroup analysis (weighed mean difference −5.39, P=.07, CI −11.14 to 0.36, Z=1.84) (Table 3).
Heterogeneity and publication bias
Heterogeneity was detected in the number of harvested lymph nodes, operative time, intraoperative blood loss, time to first flatus, and postoperative hospital stay, where the random effects model was used for analysis. Funnel plots were produced for primary outcome variables. Figure 5 suggested that the finding of each variable was symmetrical on the whole, apart from the limitations in the use of funnel plots to detect publication bias when less than 10 studies were included.
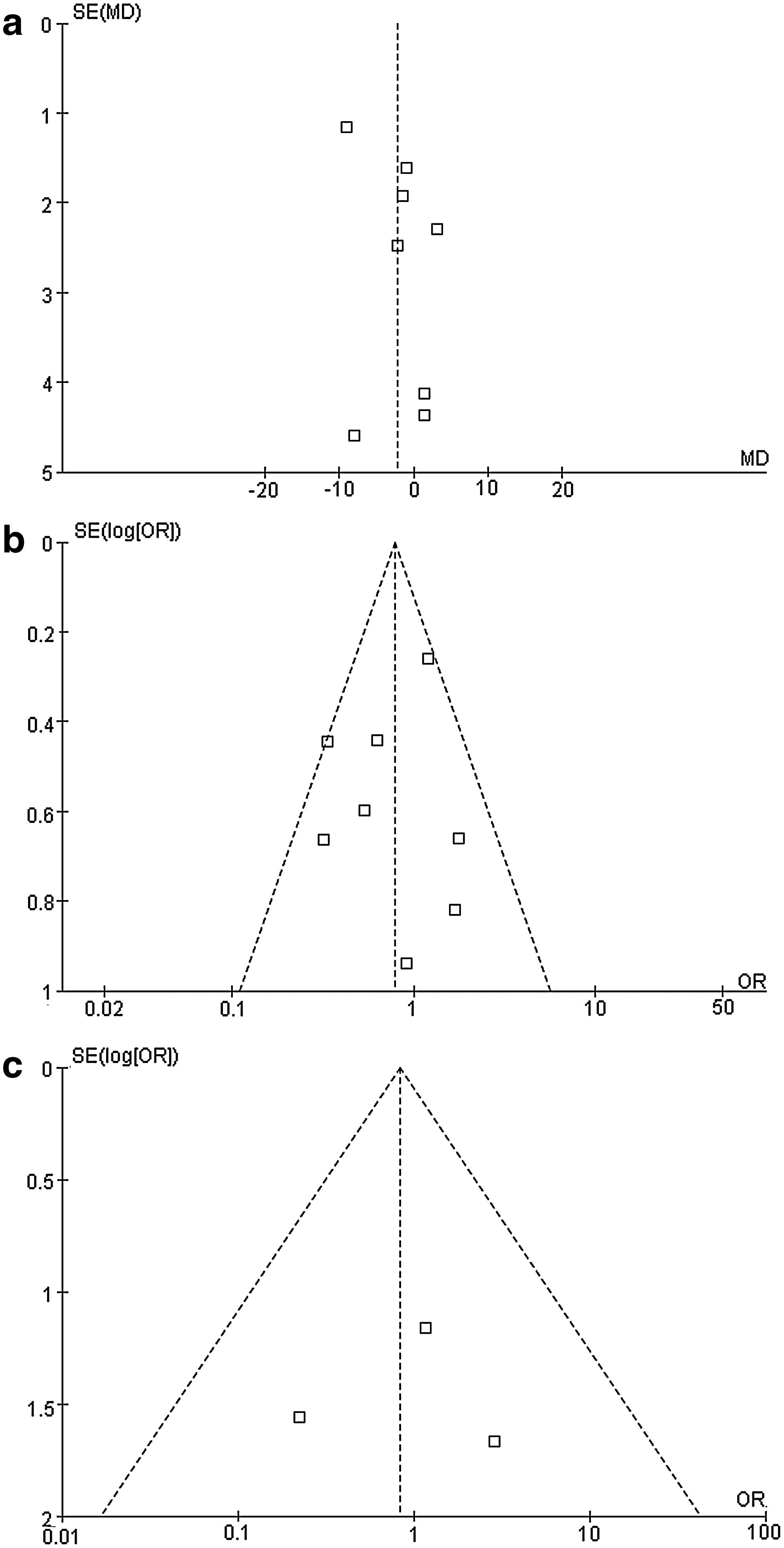
Funnel plots for primary outcomes:
Discussion
Laparoscopic surgery for gastric cancer is still less preferred than for colorectal cancer because it is especially technically demanding. However, laparoscopic gastrectomy is gaining increasing popularity, especially in Eastern countries. The feasibility of using LADG as an alternative to ODG has already been proven by meta-analysis. 5 Nevertheless, laparoscopic total gastrectomy is technically more difficult. Although many studies on this approach have been reported, its efficacy in gastric cancer treatment remains controversial. By reviewing the relative studies, we find three types of laparoscopic total gastrectomy. The first is to perform gastrectomy completely laparoscopically (often called totally laparoscopic total gastrectomy). 24 The second is to carry out the operation primarily under the laparoscope, with a small epigastric incision for extracorporeal anastomosis (LATG). The third is to do the operation with the aid of a hand in abdominal cavity (hand-assisted total gastrectomy). 25 Among the three types, LATG is most often used. This approach has the advantages of both open surgery, which provides direct vision, and laparoscopic surgery, which entails fine dissection and less invasiveness. 26 Application of LATG in both early and advanced gastric cancer has been reported.26–28 Some of such studies are retrospective nonrandomized controlled studies16–23 ; the others are noncomparative descriptive studies. To our knowledge, there are no completed randomized controlled trials comparing LATG and OTG, although there are a few randomized controlled trials comparing laparoscopy-assisted gastrectomy and open gastrectomy, 29 which involved procedures other than LATG. Therefore, as a preliminary evaluation, a meta-analysis based on existing nonrandomized controlled trials is still meaningful for determining whether LATG can be used as a safe or even better alternative to OTG. In all included studies in this meta-analysis, the spleen is preserved. Avoiding splenectomy whenever possible is generally encouraged in gastrectomy for gastric cancer. 30 What is more, the benefit of splenectomy has not been confirmed even in Stage II, IIIA, and IIIB cancers. 31
As a crucial indication to evaluate oncologic safety of laparoscopic gastrectomy, efficacy of lymphadenectomy is an important factor for the prognosis of gastric cancer. In the case of LADG and ODG, the latter procedure is often believed to be superior to lymphadenectomy.6,32 However, pooled data of high-quality studies by recent meta-analysis showed a similar number of lymph nodes harvested in LADG and ODG. 5 Similar results were found in this meta-analysis on LATG and OTG. Although fewer lymph nodes (a mean of 2.14) were harvested in LATG, there was no statistically significant difference between the two approaches (P=.26). The same is true in the analysis of high-quality studies (P=.24). These results support the oncological validity of LATG.
In our meta-analysis, the overall postoperative complication rates of LATG and OTG were similar (P=.14), despite the fact that the OR (0.79) seems to favor LATG. Nevertheless, a clear advantage of LATG was seen in the subgroup analysis (P=.02). Anastomotic leak and stenosis are among the most frequent complications after total gastrectomy; our analysis revealed no difference between the two groups. Although in the 2009 study of Lee et al. 33 indicated a higher rate of anastomotic stenosis in LATG compared with LADG, improvement in anastomotic technique helps to solve this problem. 20 A similar rate of wound complications can be seen in both groups. All pancreatic leak cases and most pneumonia cases occurred in the OTG group, although no statistical difference was found. In the case of distal gastrectomy, LADG also has similar or lower incidence of postoperative complications compared with ODG.6,7
In both LATG and OTG, postoperative mortality is low, with no difference between approaches, confirming the safety to LATG in gastric cancer.
Overall (or cumulative) and disease-specific 5-year survival rates are important variables to evaluate the effect of surgical treatment on malignancies. Data on these variables were available in only two enrolled studies,16,21 where the figures from LATG and OTG are all equivalent. These facts help to justify the long-term effects of applying LATG in gastric cancer, although the combination of such data in RevMan is difficult as survival is usually calculated indirectly by using the Kaplan–Meier method.
As far as secondary outcomes, LATG takes 41.06 minutes longer to perform than OTG, which is likely because of the complexity of this approach. Although fine dissection is possible under the laparoscope, it requires more time to adjust the camera and instruments to optimize exposure. A similar phenomenon exists for LADG, where the operative time is 48 minutes longer. This variable is affected by the proficiency of the surgeon. Kim et al. 34 compared the time needed for LATG in cases performed in early and late experience and found a significantly shorter operation time as surgeon experience increased.
This study also shows that LATG may significantly reduce intraoperative bleeding compared with OTG (253.17 mL on average). A possible explanation is that the laparoscopic approach provides enhanced visibility during dissection of the gastrosplenic ligament, the distal esophagus, and the diaphragmatic crura, facilitating hemostasis, which may be challenging in open surgery. 19 As a result, the requirement for blood transfusion will be reduced, which decreases postoperative morbidity and mortality. 35
Although operative time is longer for LATG, this group recovers more quickly compared with the OTG group. A mean of 2.55 times less analgesics usage with this approach may be due to the fact that it is less invasive, which leads to more tolerable postoperative pain. Faster return of bowel function results in earlier oral intake. Decreased length of hospital stay often results in a quicker resumption of daily life activities. Both are beneficial for reducing postoperative cardiovascular and respiratory complications. We noted no difference in postoperative hospital length of stay in the subgroup analysis and suspect that variations on criteria for discharge in different hospitals may have contributed to this discrepancy.
The heterogeneity between groups on operative time, blood loss, and number of harvested lymph nodes arises from the difference in surgeon proficiency in laparoscopic gastrectomy. Systematic training in a high-volume surgical center is a good approach to acquiring the skills to perform LATG. 36 At this point, most studies on the learning curve of laparoscopic gastrectomy focus on LADG.37,38 As LATG is more complicated, an independent study on the learning curve of LATG should be carried out.
Our study has several limitations. There are no randomized controlled trials included in this study, although in most included studies patient demographic data are matched between groups. The heterogeneity or bias between studies was detected during the analysis, indicating possible bias in the design or conduction of these studies. Specifically, in nonrandomized studies a risk of selection bias exists when the decision on which approach to take is made. Additional evidence from large randomized controlled trials is necessary to endorse LATG as a good alternative to OTG. All studies included in this meta-analysis are from East Asia, where the incidence of gastric cancer is high 39 and laparoscopic gastrectomy is frequently used. Fortunately, most patients in Eastern countries are diagnosed at an earlier stage and therefore have a higher likelihood of being resectable, compared with their Western counterparts. However, Western patients have a higher rate of both proximal and diffuse-type gastric cancer, where total gastrectomy is needed. 40 For resectable gastric cancer cases, Western patients are also more likely to be obese. These patients are more likely to benefit from laparoscopic gastrectomy. Lastly, during the database search, one study from Belgium 41 was initially considered a candidate for this meta-analysis but was excluded because of a totally laparoscopic approach and added splenectomy. Further high-quality studies on LATG from Western nations will add more evidence on the feasibility of this approach.
Conclusions
In conclusion, the available data suggest that LATG is a safe technical alternative to OTG for the treatment of upper or proximal cancer. LATG has the merits of less blood loss and quicker postoperative recovery, while maintaining the same oncologic safety and survival as OTG.
Footnotes
Acknowledgments
The authors gratefully acknowledge Associate Professor Quancai Cai for his invaluable suggestions for this meta-analysis.
Disclosure Statement
No competing financial interests exist.