
Abstract
Abstract
Background:
Peritoneal dialysis (PD) is an alternative modality to hemodialysis and is usually used to treat patients with end-stage renal disease. Dual-incision laparoscopic surgery (DILS) had been reported in several surgical fields; however, no report was proposed about DILS in PD catheter implantation (DILS-PD). In this study, we present DILS with a novel, simple, and safe procedure for PD catheter implantation with fixation and describe the long-term outcome.
Subjects and Methods:
We conducted a prospective data collection and retrospective review of all PD patients from April 2010 until June 2012. During this study period, we performed open surgery for PD catheter implantation (OS-PD) and DILS-PD concurrently. Demographic data, medical, operative, and postoperative findings, and information regarding complications were compared between these two groups.
Results:
Forty-eight patients had DILS-PD, and 70 patients had OS-PD. There was no difference between the two groups in age, gender, American Society of Anesthesiologists grade, creatinine level, body mass index, and previous abdominal surgery. There was no surgical mortality in either group. The follow-up period ranged from 6 to 24 months, with a mean of 22.4±16.5 months. There was no tube migration in the DILS-PD group, but 25.7% of the patients in the OS-PD group had tube migration (P<.001). A significantly decreased exit-site/tunnel infection rate was found in the DILS-PD group (4.2%) compared with the OS-PD group (17.1%) (P=.032). However, there was no obvious difference in peritonitis occurrence between groups. A significantly decreased catheter failure rate was found in the DILS-PD group (4.2%) compared with the OS-PD group (22.9%) (P=.006). DILS-PD group patients had a favorable survival rate for catheter implantation compared with OS-PD group patients.
Conclusions:
Our DILS-PD with fixation technique is a simple and safe procedure. This procedure minimized or even eliminated the possibility of migration without additional cost. Our DILS-PD fixatation technique should be recommended for use routinely.
Introduction
The PD catheter is conventionally placed through a small open incision that allows the catheter to be threaded through into the pelvic cavity. Furthermore, the percutaneous technique has also been used to insert the PD catheter.3,4 Over the years, more and more reports have proposed the role of laparoscopy in PD catheter insertion with advantages including less pain, faster recovery, and acceptable long-term catheter survival.5–8 However, higher cost, longer operative time, and inability to use in high-risk patients might impede usage of this procedure in the ESRD population.9–11
Dual-incision laparoscopic surgery (DILS) has been reported in several surgical fields.12–15 Compared with conventional laparoscopic surgery, DILS reduced the number of trocars and offered less pain, shorter length of incision, quicker recovery, and better cosmetic appearance. However, no report has yet been proposed about the effectiveness of DILS in PD catheter implantation (DILS-PD). In this study, we present DILS with a novel, simple, and safe procedure for PD catheter implantation with fixation and describe the long-term outcome of patients undergoing DILS-PD.
Subjects and Methods
Data collection
We conducted a prospective data collection and retrospective review of all PD patients from April 2010 until June 2012 at Chang Gung Memorial Hospital, Linkou, Tayoun, Taiwan. The Internal Review Board of Chang Gung Memorial Hospital approved the study. All patients were followed at a PD clinic at our hospital. During this study period, we performed open surgery for PD catheter implantation (OS-PD) and DILS-PD concurrently. There was no randomization or special selection of procedure in these patients. Demographic data, medical, operative, and postoperative findings, and information regarding complications were recorded into a computerized database prospectively. Follow-up time was defined as from the date of catheter implantation to the date of catheter removal or to December 2012. Demographic information was collected with the results of physiological and biochemical analyses. In addition, perioperative findings, operative time, and conversion to open surgery were recorded. Postoperative data included migration, blockage, exit-site infection, herniation, peritonitis, and catheter failure.
DILS-PD technique: a novel, simple, and safe PD catheter insertion and fixation method
A Tenckhoff catheter (coiled peritoneal silicone catheter, double cuffed, 56.5 cm, 14.7 FR; Horizon Medical Products, Manchester, GA) was used for all procedures. All patients received 1 g of cefazolin sodium intravenously prior to surgery as prophylaxis. The catheters were implanted in the operating room by two experienced surgeons (C.-N.Y. and T.-L.H.) with the same procedure.
During the operation, the patient was placed in a supine position under general anesthesia, and a nasogastric tube and a Foley tube were inserted. A 10-mm subumbilical incision was made, and the pneumoperitoneum was increased to 12 mm Hg. A 10-mm trocar was inserted in the incision, and then a 30° rigid 5-mm videoscope was inserted. Another 5-mm port was inserted at the left or right pararectus line at the proper height under direct visualization (Fig. 1). Then we switched the scope to a 5-mm trocar. At first, the patient was placed in the Trendelenberg position, which allows most of the viscera out of the pelvis. The peritoneal cavity was fully explored, and all potentially interfering adhesions were lysed. One 2-0 silk suture with a straight needle was inserted into the inner opening of the catheter after one thread of suture was passed through the side hole of the catheter (Fig. 2A). Then the catheter was introduced through the 10-mm trocar, and its internal tip was brought to the medial umbilical ligament. The straight needle was passed through the medial umbilical ligament under direct vision to prevent vessel injury (Fig. 2B). Then the catheter was fixed to the medial umbilical ligament after the two threads of suture were fixed by hemoclips (Fig. 2C). The proximal end of the catheter was brought out to arise from the umbilical port, and the inner cuff was fixed to the underlying fascia using a 3-0 Vicryl® suture (Ethicon Inc., Somerville, NJ). The remaining proximal catheter was placed in the subcutaneous tunnel and was exteriorized from the left pararectus port. After the operation, there were one umbilical wound and another exit-site wound with tube placement.
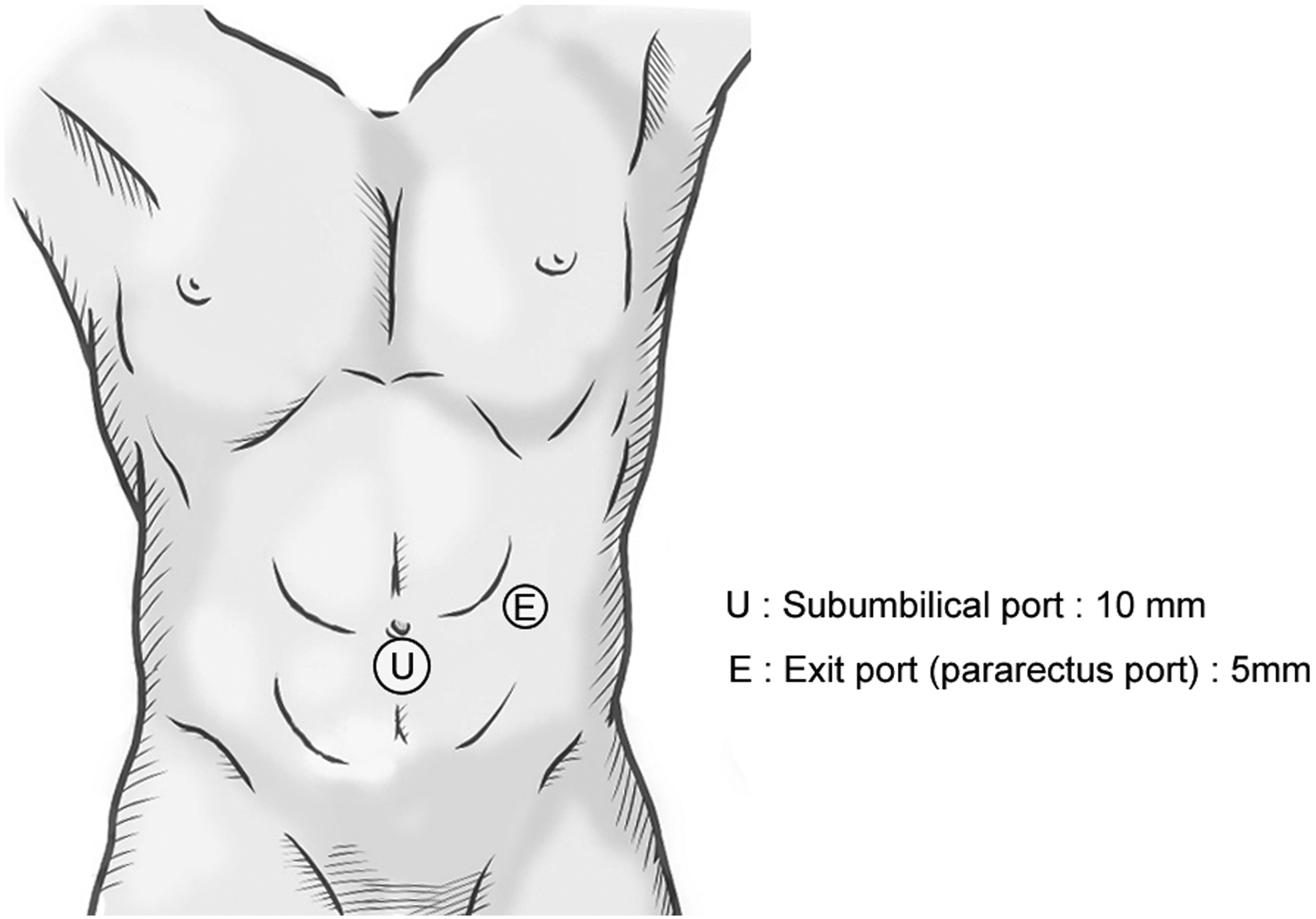
Insertion site of trocars. U marks where one 10-mm subumbilical incision was made and one 10-mm trocar was inserted in the incision. E marks the left or right pararectus line at the proper height for a 5-mm trocar.
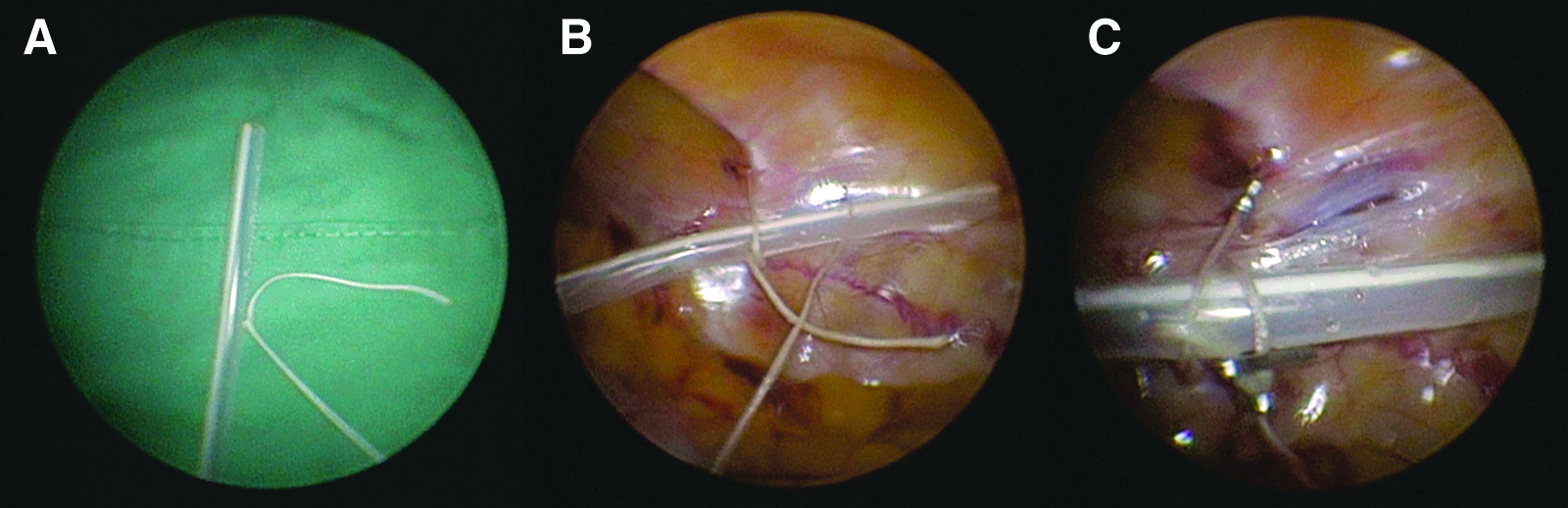
Fixation of the peritoneal dialysis catheter.
Postoperative care
Vital signs were monitored every 4 hours in the first 24 hours after surgery. Regular medical treatment was resumed, and the patients were evaluated for evidence of pulmonary congestion, acid–base abnormalities, or hyperkalemia. All patients were encouraged to resume oral intake as soon as possible. Not longer than 1 week after discharge, all patients underwent a physical examination in the PD clinic, focusing on catheter patency, exit-site infection, and signs of peritonitis. A rapid in-and-out exchange was performed. A plain film of the abdomen was obtained to ascertain the position of the catheter in the pelvis (Fig. 3). The patient was scheduled for the first cycle of PD. Further PD cycles were performed as scheduled by the nephrologists, according to the patient's status. Peritoneal fluid cultures were taken every 14 days, and the patient was treated accordingly. The diagnosis of peritonitis was made on the basis of at least two of the following: (1) abdominal pain or cloudy peritoneal dialysis fluid, (2) leukocytosis in the peritoneal dialysis fluid (white blood cell count, >100/mL), and (3) positive Gram stain or culture from PD fluid. Migration was defined as migration of the catheter tip out of the pelvis, which was proved by abdominal plain film. Blockage was defined as inflow or outflow decreased even after three shots of intracatheter instillation of urokinase. Exit-site infection was defined as local redness, swelling, tenderness, or purulent discharge limited to the exit site or extending into the subcutaneous tunnel. Bloody peritoneal dialysate was defined as pinkish or red discoloration of the dialysis fluid. Catheter failure was defined as persistent peritonitis, exit-site/tunnel infection refractory to antibiotic treatment, persistent dialysate leak, or outflow obstruction refractory to conservative treatment.

A plain film of the abdomen. The film was obtained to ascertain the proper position of the catheter in the pelvis fixed with hemoclips.
Statistical analysis
Pearson's chi-squared test and Fisher's exact test were used as appropriate to compare categorical variables. Quantitative variable were compared by Student's t test. The odds ratio and 95% confidence interval were calculated by logistic regression in the case of qualitative variables and linear regression for quantitative ones. The cumulative PD catheter survival estimates were generated using the Kaplan–Meier method, and survival analysis was compared using a log-rank test. Statistical analysis was done with SPSS version 20.0 for Macintosh software (SPSS Inc., Chicago, IL). A value of P<.05 was considered statistically significance.
Results
In total, 118 patients who had PD catheter implantation were enrolled into this study during this period. Forty-eight patients had DILS-PD, and 70 patients had OS-PD. Patient characteristics are summarized in Table 1. There was no statistical difference between the two groups in age, gender, American Society of Anesthesiologists grade, preoperative creatinine level, body mass index, and previous abdominal surgery. There was no surgical mortality in either group. In the DILS-PD group, no conversion to open surgery was noted. The DILS-PD group had a longer operative time than the OS-PD group, but the difference did not reach statistical significance (62.47±11.98 versus 56.37±19.65 minutes, P=.061).
ASA, American Society of Anesthesiologists; BMI, body mass index; Cr, creatinine; DILS-PD, dual-incision laparoscopic surgery-peritoneal dialysis; OS-PD, open surgery-peritoneal dialysis.
The follow-up period (Table 2) ranged from 6 to 24 months, with a mean of 22.4±16.5 months. No mortality occurred in this series. There was no tube migration in the DILS-PD group, but 25.7% patients in the OS-PD group had tube migration (P<.001). Although decreased catheter blockage (4.2%) and herniation (4.2%) rates were observed in the DILS-PD group compared with the OS-PD group, this did not reach statistical significance. A significantly decreased exit-site/tunnel infection rate was found in the DILS-PD group (4.2%) compared with the OS-PD group (17.1%) (P=.032). However, there was no obvious difference in peritonitis occurrence between the two groups. A significantly decreased catheter failure rate was found in the DILS-PD group (4.2%) compared with the OS-PD group (22.9%) (P=.006).
DILS-PD, dual-incision laparoscopic surgery-peritoneal dialysis; OS-PD, open surgery-peritoneal dialysis.
In the DILS-PD group, the catheter survival rate was 96%, 96%, and 96% at 30 days, 180 days, and 360 days, respectively. In the OS-PD group, the catheter survival rate was 91%, 87%, and 81% at 30 days, 180 days, and 360 days, respectively. The mean catheter survival rates in DILS-PD and OS-PD were 608.9±18.0 days and 500.87±24.4 days, respectively. The DILS-PD group patients had a favorable catheter survival rate compared with OS-PD group patients, demonstrated by the log-rank test (P=.013) (Fig. 4).
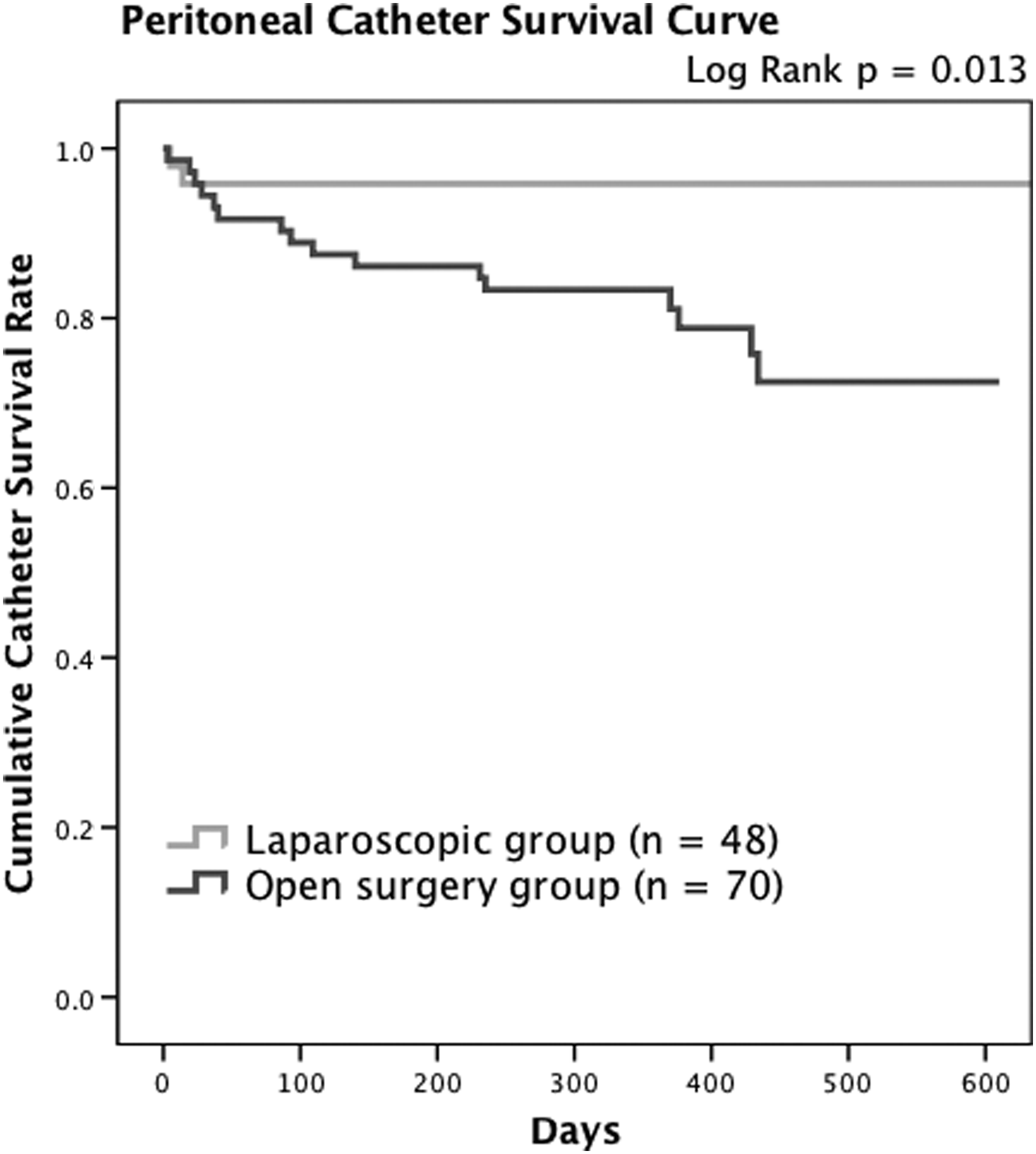
The peritoneal dialysis catheter survival rate between dual-incision laparoscopic surgery-peritoneal dialysis (n=48) and open surgery-peritoneal dialysis (n=70) patient groups. The laparoscopic surgery group patients had a more favorable catheter survival rate than the open surgery group patients, demonstrated by the log-rank test (P=.013).
Discussion
The laparoscopic approach has emerged as a safe and effective minimally invasive approach for PD catheter implantation. Studies have shown that the laparoscopic approach is associated with reduced postoperative pain, an acceptable incision, a short hospital stay, and quick recovery.5,6,16 Moreover, the laparoscopic approach is improved to microinvasiveness by reducing port numbers and incision length.17,18 We introduced a novel, simple, and safe method to create a route for PD with delicate implantation and fixation without any extra incision. Several important issues that have emerged from this study need to be addressed.
First, evidence of the safety of a new technology needs to be provided before its implementation in routine clinical practice. The present results indicated that DILS-PD is a safe and feasible procedure. There were no intraoperative complications such as bowel injury or uncontrollable bleeding associated with the procedure. There was no mortality among the patients included in the study. Most of our patients resumed their daily routine immediately after the operation. Early oral intake resumption and ambulation were noted in our patients, which indicate that DILS-PD allows early recovery. The catheter survival rate was 93.8%, and the median catheter survival was 13.5 months (range, 4–26 months). Compared with the OS-PD group, the migration and exit-site infection rates were significantly reduced, and the catheter survival was significantly prolonged. Our result was supported by a meta-analysis study recently reported by Hagen et al. 19
Second, the most common etiologies of failure of PD were tube migration and blockage.7,20 Laparoscopy has been shown to be superior to other techniques because it enables direct visualization of the entire peritoneal cavity. Several studies have presented the importance of fixation of the tube, especially under direct visualization by laparoscopy.21–24 Several peritoneal fixation devices and methods have been reported.21,25,26 However, more procedures induce more peritoneal trauma, which leads to further fibrosis and adhesion. We fixed the tube simply to the medial umbilical ligament, which limited peritoneal trauma and decreased the migration with a promising improvement, demonstrated by the 0% migration rate in the follow-up abdominal plain film. Moreover, several studies have reported that decreasing the size and number of incisions results in a lower incidence of adhesions and incisional herniations.27,28 Compared with open surgery, DILS-PD is associated with fewer incisions and limited parietal peritoneal trauma; therefore, the DILS-PD procedure should theoretically decrease postoperative adhesion formation. Catheter blockage significantly decreased to 4.1% in DILS-PD compared with OS-PD (8.5%). Contrary to other reports, the PD catheter blockage rate ranged from 4.5% to 13.1%, mainly related to migration. Using our DILS technique, we can achieve an excellent migration rate, the lowest ever recorded.
Third, infectious complication is another consideration of PD. The DILS-PD group had a significantly lower exit-site infection rate (4.2%) than the OS-PD group (17.1%). Less trauma and minimal invasiveness by our DILS-PD technique explained the reduced infection complication rate compared with other series.5,8,19,20,29 However, a disadvantage of laparoscopic implantation of the PD catheter is the higher cost compared with open surgery. The extra devices used for the previous PD implantation technique increased the cost should be the main reason.9,10,24 Our novel technique with clip fixation did not increase the requirement for additional instruments and reduced the cost as low as possible.
Fourth, another advantage of our DILS-PD technique is the low learning curve compared with other minimally invasive procedures; this was demonstrated by the nonsignificantly greater operative time. Without complex procedures, we applied the easiest fixation method with clipping enhancement. Furthermore, we fixed the cuff on the fascia under direct vision, which made the procedure simpler. Although several reduced trocar laparoscopic PD implantations have been reported,21,29–31 the suboptimal viewing angles, crowded instruments, complex procedure, and loss of triangulation may contribute to the prolonged operative time. 29
Although our results may support the safety and feasibility of our DILS-PD technique, there are several problems associated with this procedure that still need to be emphasized. First, the contraindications to DILS-PD are similar to those of laparoscopic surgery, including hemodynamic instability, inability to tolerate pneumoperitoneum, the presence of extensive intraabdominal soiling, and dense adhesions. Second, compared with the open group, DILS-PD resulted in more bloody dialysis on the first postoperative day. It might be related to oozing from the peritoneal opening of the lateral trocar. However, no further obstruction by blood clots was noted in this series, and bloody dialysis would subside thereafter in this series. Third, this was a retrospective study, and the selection of patients would not be randomized. The selective and recall bias could not be prevented completely. However, the characteristics of both groups were similar and homogeneous, so that we could perform analysis of both groups.
In conclusion, our DILS-PD with fixation technique is a feasible and safe procedure that can be performed in patients who need PD for ESRD. With DILS-PD, we fixed the catheter in the pelvis safely and easily and minimized or even eliminated the possibility of migration without additional cost. The limited length of the incision reduced postoperative pain and incisional herniation. Our DILS-PD with fixation technique can be an optimal technique for patients who need PD catheter implantation and should be recommended for use routinely.
Footnotes
Disclosure Statement
No competing financial interests exist.