
Abstract
Abstract
Background:
For better cosmetic appearance, attempts to reduce the number of laparoscopic wounds have been sought. Investigators have thus begun to carry out procedures through a single incision or natural orifice endoscopic surgery instead of using conventional laparoscopic surgery. The authors here describe transumbilical single-incision hybrid transperineal laparoscopic surgery as a novel approach for vaginoplasty using a sigmoid graft.
Patients and Methods:
From August 2010 to October 2012, 15 young females with Mayer–Rokitansky–Kuster–Hauser (MRKH) syndrome underwent laparoscopic sigmoid vaginosplasty using a combined transumbilical single-incision and transperineal approach. A multichannel single port was placed through the umbilical incision for the main laparoscopic procedures. A 12-mm trocar as an assisting working port was inserted into the pelvic cavity through the transvaginal dimple between the rectum and urethra.
Results:
A functioning vagina 12–15 cm in length and approximately 4 cm in width was created in all the patients. The average operative time and hospital stay were 151.5±34.2 minutes and 7.4±3.2 days, respectively. The only perioperative complications were 1 case of stress ulcer and 1 case with umbilical infection. All patients were satisfied with the surgery, and 12 of them had subsequent sexual activity.
Conclusions:
Transumbilical single-incision hybrid transperineal laparoscopic sigmoid vaginoplasty offers a feasible scarless approach for females with MRKH syndrome. The favorable cosmetic results would favor use of this type of vaginoplasty as an alternative to the conventional laparoscopic approach.
Introduction
P
Patients and Methods
Patients
From August 2010 to October 2012, 15 young females ranging in age from 16 to 25 years (mean age, 21.7±3.1 years) with MRKH syndrome underwent a laparoscopic sigmoid vaginoplasty via the transumbilical single-incision hybrid transperineal approach. Before surgery, all the patients had undergone genetic evaluation, abdominal ultrasonography, computerized tomography, and intravenous pyelography. They presented primary amenorrhea with normal secondary sexual characteristics, typically female hair growth, an absent or rudimentary uterus with normal vulvar development, and an approximately 2–3-cm-deep depression at the vaginal opening. Three of the patients had other abnormalities, including 1 with Meckel's diverticulum (found intraoperatively), 1 with indirect inguinal hernia, and 1 with absence of the right kidney.
Preparation included a low-residue semiliquid diet and oral metronidazole and gentamicin for 3 days before operation. An isotonic saline enema was also given once a day, and a cleaning enema was added on the day of surgery. Antibiotic prophylaxis was administered 1 hour before the procedure.
The operative approach (including details of each operative step in sequence) was approved by our institutional review boards. Informed consent was obtained from all patients.
Surgical procedure
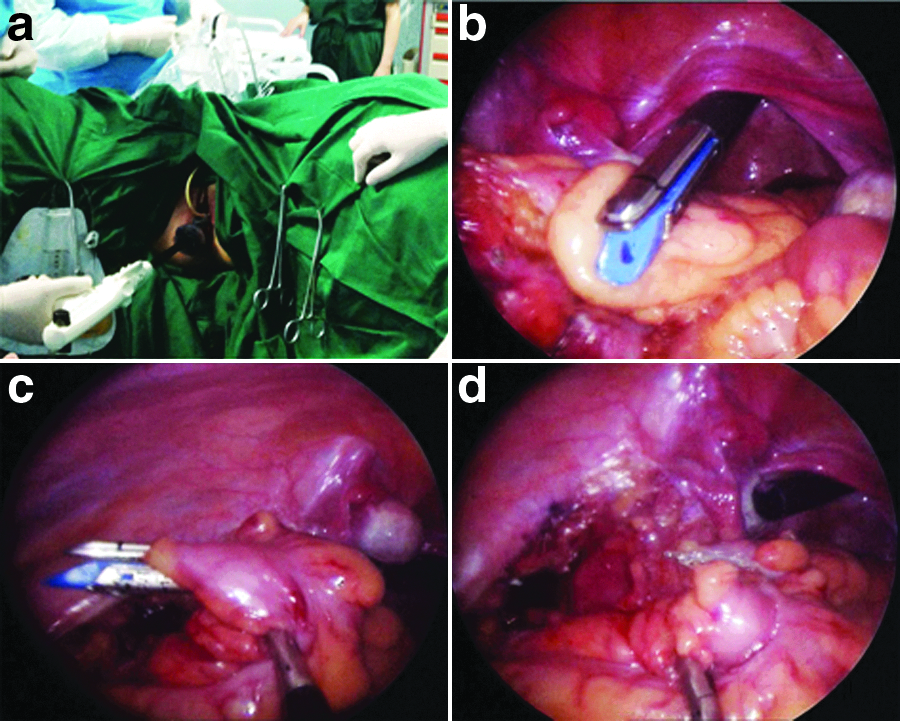
Under endotracheal anesthesia, the patient was placed in an extended lithotomy Trendelenburg position as for a synchronous combined abdominoperineal approach. A 25–30-mm incision was made at the left edge of the umbilicus to gain initial entry into the peritoneal cavity. A multichannel single port was placed through the incision (Fig. 1). Carbon dioxide was insufflated to maintain the intraperitoneal pressure at 12 mm Hg. A 5-mm 30° rigid laparoscope was first introduced for a diagnostic exploration of MRKH syndrome. The operative table was adjusted 30° head-down with the patient's left side slightly tilted to facilitate clearance of the intestines from the pelvis. Subsequently, a U-shaped incision was made in the deepest depression of the vaginal vestibule, and a tunnel between the rectum and urethra or bladder up to the pouch of Douglas was dissected bluntly by the surgeon using his index finger. Under laparoscopic vision, another 12-mm trocar as the assisted working port was inserted into pelvic cavity through the canal.

View of the multichannel single port in the umbilicus with the patient tilted in the Trendelenburg position.
The surgeon positioned himself at the right side of the patient using a 5-mm extra-long curved grasper with his left hand and the dissecting instrument (5-mm monopolar hook or Harmonic® [Ethicon Endo-Surgery, a subsidiary of Johnson & Johnson, Cincinnati, OH] scalpel) in his right hand. The first assistant operated the camera, and the second assistant manipulated the sigmoid by a 10-mm transperineal grasper.
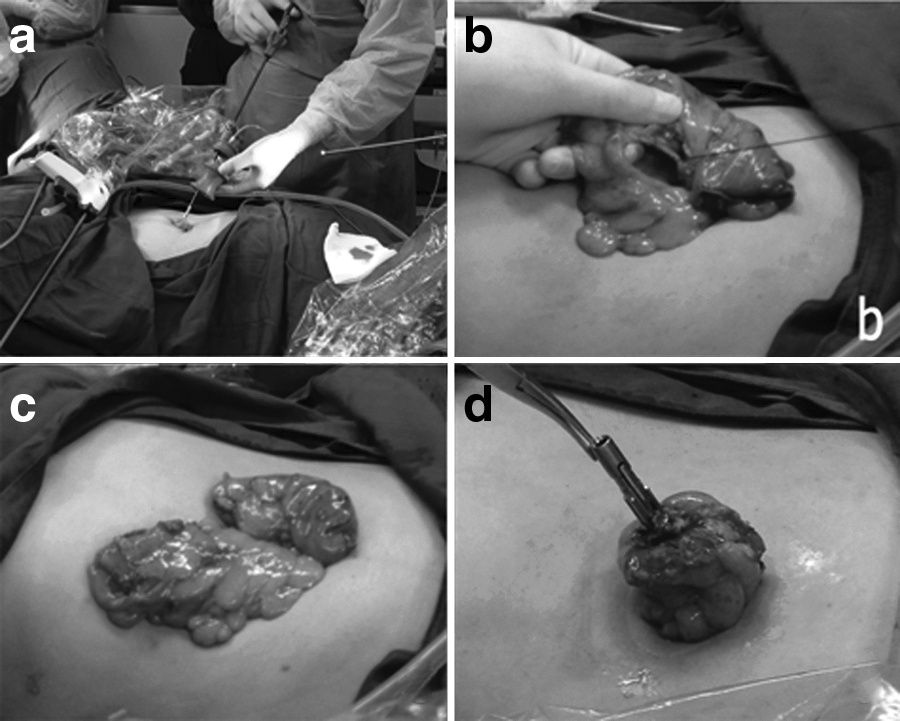
The sigmoid was examined by transillumination to verify its vascularization, and its length was determined before the intestinal graft was mobilized. The medial side of the sigmoid mesocolon was incised, and the avascular plane between the visceral and parietal pelvic fascia was entered at the level of the sacral promontory. Blunt dissection was used to lift the inferior mesenteric vessels away from the retroperitoneum. The dissection was continued to the lateral attachment of the sigmoid and descending colon. After full mobilization of the sigmoid, the rectum was sealed and transected using a 60-mm Endo-GIA® stapler (Reach Surgical, Beijing, China) through the perineal trocar (Fig. 2). Following the umbilical multichannel single-port withdrawal, the mobilized sigmoid was exteriorized and shielded by gauze pads. Extracorporeal preservation of the vascular arcades after several ligations of mesenteric vessels, transection for the upper part of the sigmoid, and preparation for colorectal anastomosis were done as with the open method (Fig. 3). The sigmoid graft was 10–12 cm long and remained vascularized by the inferior sigmoid artery, the proximal end was sealed by continuous suture for the new vaginal introitus, and the segment was then placed back into the pelvic cavity. Before the distal descending colon was returned, a purse-string suture was placed for the anvil. The single port was replaced, and the pneumoperitoneum was recreated. Then, an intracorporeal end-to-end colorectal anastomosis was performed using a transrectally introduced circular stapler to restore the bowel continuity (Fig. 4).
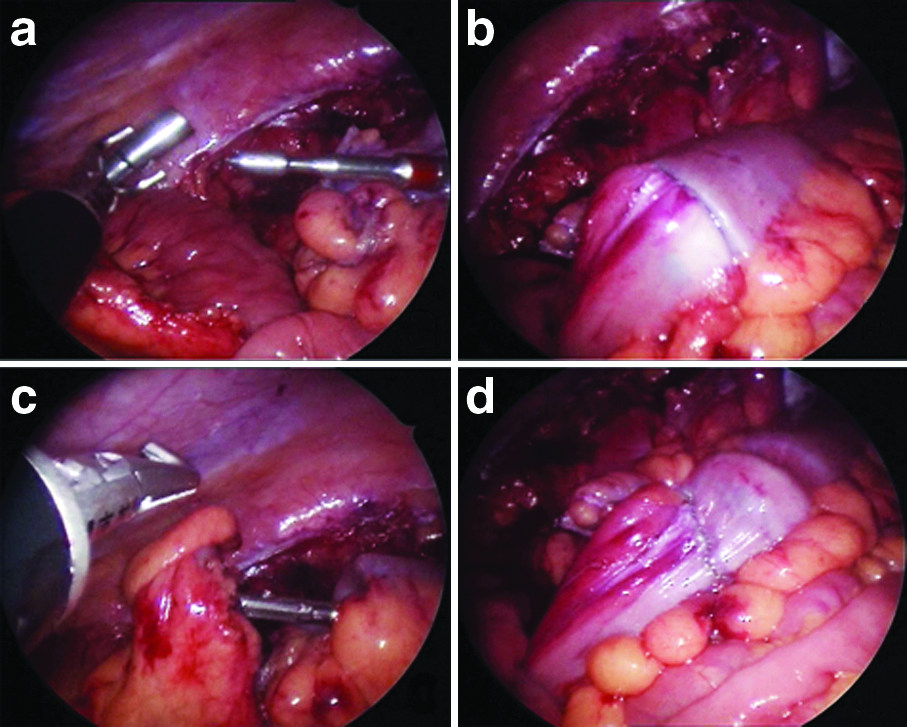
Under laparoscopic guidance, the perineal trocar was removed, and this tunnel was enlarged. The sigmoid graft was rotated 180° clockwise and pulled down through the tunnel to the new vaginal orifice. The colon–perineal anastomosis was completed with interrupted absorbable sutures (Fig. 5). A vaginal stent (32–38 mm in diameter) was left in the neovagina until the healing environment was stabilized. At the end of the surgery, the pelvis was inspected to confirm the vascularization of the sigmoid graft. Finally, the umbilical incision was closed appropriately (Fig. 6).

Good width and depth of the neovagina.

Wound in the umbilicus at the end of the operation.
Postoperative management
Broad-spectrum antibiotics were given intravenously for 2–3 days. The patients were kept fasting for the first 2–3 days. All patients were then able to return their normal diet and activity by 5–7 days. Every patient received a physical examination before discharge. The neovaginal length, defined as the straight distance from the introitus to the tip of the neovagina, was measured. The patients were advised to wash the neovagina with 0.1% benzalkonium bromide solution and wear a vaginal stent every night until regular sexual intercourse took place. The regular follow-ups were usually 2, 6, and 12 months later and thereafter once a year. The frequency of sexual activity, the use of lubricants, the presence of painful intercourse, any difficulty of urination and defecation, and the use of the vaginal stent were recorded through interviews.
Results
All the procedures were successfully performed with no intraoperative morbidity. Concomitant Meckel's diverticulum excision and herniorrhaphy were carried out in 2 cases. The average operative time was 151.5±34.2 minutes. The perioperative complications included 1 patient with a stress ulcer and another with an umbilical infection. The hospital stay was 7.4±3.2 days. A functioning vagina was created in all women. The mean length of the neovagina was 13.12±1.14 cm (range, 12–15 cm), and the mean width was 3.99±0.26 cm before discharge. Mean follow-up was 13.6±4.1 months (range, 5–30 months). No length shrinkage was observed during postoperative follow-up. All patients were satisfied with the surgical outcome.
Twelve patients had subsequent sexual activity. The interval between the operation and first intercourse was 2–6 months. None of these 12 women from interviews developed vaginal stenosis as a result of the contracture that caused painful intercourse or had spontaneous bleeding from the vagina. The other three women still required a vaginal stent every night because they have had no sexual partner.
Discussion
MRKH syndrome may be diagnosed during adolescence, but its treatment is usually delayed until the woman is ready to start sexual activity. It may be either nonsurgical or surgical, but the chosen method needs to be individualized depending on the patient's needs, motivation, and the options available. 7 The goal of any method is to create a vaginal canal with an adequate diameter and length, appropriate axial direction, and normal secretion/lubrication to accommodate sexual intercourse. Frank's method, as a nonsurgical technique, has the advantage of avoiding surgery; however, it requires long-term catheterization, which may not be accepted by younger women, and the depth of the neovagina is often limited. There are many reports on different surgical procedures and their outcomes following postoperative anatomical and functional results: some popular methods include split- and full-thickness skin grafts, bladder or buccal mucosa grafts, local genital flaps, and intestinal flaps; Baldwin was the first to describe the use of an intestinal segment for vaginoplasty in 1904; and Wallace was able to use the sigmoid colon successfully in 1911.8–11
For several decades vaginoplasty using a rectosigmoid graft has been the first choice for the correction of congenital vaginal agenesis. In contrast with other techniques, rectosigmoid vaginoplasty results in a self-lubricating and good-sized neovagina, which does not require postoperative dilatation for extended periods of time. In our series, no intraoperative or intestinal complications occurred. Intestinal complications are rarely reported with sigmoid vaginoplasty, and we suggest that preoperative bowel preparation, previous experience with bowel surgery, and meticulous use of staplers for colonic transection and anastomosis are essential prerequisites to avoid such complications. On vaginal examination of our patients, we found that all patients had an excellent cosmetic appearance of the neovagina with an adequate vaginal orifice. Most of all patients were satisfied with their surgical outcome. Therefore, using the sigmoid as a pedicled graft for the creation of a neovagina of sufficient length is effective, as it may be harvested with an excellent blood supply that could prevent complications such as contractions, shrinkage, or narrowing. This segment is thick-walled and large in diameter and can tolerate trauma better than the small bowel, bladder, or skin grafts. Postoperative management is simple and easy.
The use of laparoscopy has become increasingly popular in the management of MRKH syndrome. Several authors reported a laparoscopic technique for isolating a segment of sigmoid to be used for vaginal construction.3–6 It has been shown that the laparoscopic approach achieved the same results as the laparotomy. However, the conventional type of laparoscopic sigmoid colpoplasty requires three to five ports, and a transabdominal incision of 5–7 cm has to be performed in the left lower quadrant to retrieve the colon and to prepare the area for the anastomosis, which might damage the inferior epigastric artery which sometimes occurred during the operation. These incisions are susceptible for wound infections and hernia formation; as a result many patients complain of transient pain at the incision site. In addition, these abdominal incisions may limit fast recovery. NOTES and SILS are the newest branches of advanced endoscopy, which make up for the limitations of traditional laparoscopic surgery by reducing the number of trocars and the length of the incision required for colon extraction. Using both technological and technique innovations, we have refined the operation so that it can be laparoscopically performed through the umbilical single-incision hybrid transperineal approach for manipulating, dissecting, and extracting the sigmoid.
To do this, we have taken advantage of one of the new generations of port systems placed at the umbilicus via an open method, which allows multiple conventional laparoscopic instruments to be worked simultaneously through separate flexible channels sited within its atrial valve. Transumbilical SILS sigmoid vaginoplasty is feasible using a combination of conventional straight and long curved laparoscopic instruments. By rotating the patient's position with her left side elevated, most of the small intestine fell out of the surgical field. Using the pneumoperitoneum, we are able to clearly identify passage and placement of the sigmoid section. The sigmoid and descending colon could be exteriorized at the umbilicus without the need for incision extension. SILS decreases parietal trauma and offers cosmetic advantage compared with a conventional laparoscopic approach. However, there are some drawbacks in SILS, such as limitations of movement due to the clashing of instruments, the difficulty of mobilizing the sigmoid or transect rectum, and awkward ergonomics for surgeons. So we had the aim of describing an innovative technique for SILS sigmoid colpoplasty, assisted by perineal access. Resembling the framework of NOTES, another 12-mm trocar as an assisted working port is inserted into the pelvic cavity via the perineal dimple between the rectum and urethra or bladder. The transperineal grasping forceps can give excellent exposition of the sigmoid, and using an endolinear stapler cuts the rectosigmoid easily. Then the perineal canal created in the operation provides a neovagina formation. It reduces the complexity and technical challenges of the operation without increasing the number of incisions in the abdomen. This technique is well suited to the vaginal reconstruction using a sigmoid colon segment because we believe that perineal access has shortened the operation time. The reported mean operation time varied from 210 to 312 minutes for laparoscopically assisted sigmoid colon vaginoplasty.3–6 In our experience, the laparoscopic procedure takes 151.5 minutes to perform, which is less than that of other reports. This shows that laparoscopic sigmoid vaginoplasty via the transumbilical single-incision hybrid transperineal approach should be significantly superior to the conventional laparoscopic method. Besides, this procedure offers excellent cosmetic outcome. This may be especially important for a young woman suffering from MRKH syndrome. The woman is less traumatized and feels as if she is not ill because she does not have any visible scars on her abdomen.
However, there are disadvantages as well, including umbilical infection and intestinal complications. In our series, the first patient suffered from an umbilical abscess (which was managed with surgical drainage), possibly because of contamination from the exteriorized segment when it was transected and placed for the anvil of the circular stapler through the incision. After the extracorporeal sigmoid had been shielded using gauze pads and the wound was thoroughly washed before closure in subsequent cases, no further infection happened. Another woman who suffered a postoperative stress ulcer was treated conservatively without subsequent problems. Other intestinal complications reported such as intestinal obstruction, bowel adhesions, diversion colitis, ulcerative colitis, peritonitis, or fistula were not seen in this study. 12
Conclusions
Transumbilical single-incision hybrid transperineal laparoscopic sigmoid vaginoplasty is a feasible and safe technique for women with MRKH syndrome. Using perineal access to insert an additional port can help the manipulation of structures in the operative field, and this has allowed the sigmoid graft pull-through to form a neovagina. It can be performed successfully without technical challenges and does not require any extra incisions in the abdomen. Both anatomical and functional outcomes of this surgical approach are satisfactory. The favorable cosmetic results would favor use of this type of vaginoplasty as an alternative to conventional laparoscopic sigmoid colpopoiesis.
Footnotes
Acknowledgments
We thank Dr. Kenneth K.Y. Wong (Department of Surgery, Queen Mary Hospital, The University of Hong Kong) for his efforts in editing this manuscript.
Disclosure Statement
No competing financial interests exist.