
Abstract
Abstract
Müllerian duct anomalies include a wide spectrum of genital tract defects resulting from a development alteration of the genital tract. An 11-year-old girl with a hybrid septate variety uterus with left hemi-obstruction was identified. Beside preoperative imaging evaluation done with ultrasound, magnetic resonance, and hysterosalpingography, a combined laparoscopic and hysteroscopic procedure was fundamental for the diagnosis. The surgical procedure also allowed us to perform a successful and safe treatment. We propose that the American Fertility Society classification of these anomalies should be revised and that hybrid entities should be considered in the differential diagnosis of genital tract malformations.
Introduction
Case Report
The patient, an 11-year-old girl, presented to the emergency room of another hospital with complaints of acute lower abdominal pain. She had been having dysmenorrhea and low-level bleeding since menarche had occurred (5 months earlier). The pain was described as extremely crampy and continuing a few days after menstruation. Her medical history included the diagnosis of type 1 diabetes mellitus when she was 2 years old and the identification of left renal agenesis shortly after birth. The lower abdomen was painful during palpation, but no masses were appreciable. External genitalia and general physical examinations were unremarkable.
We immediately performed pelvic ultrasound (US), which showed a double uterus with a distended left Fallopian tube and hematometra in the left uterine horn. The right ovary had a normal shape and limits, whereas the left one was not identified. Pelvic magnetic resonance (MR) confirmed the presence of a bicornuate uterus. The right part had a slightly thickened wall but a normal ovary. A fluid blood collection was responsible for left uterus distension. The left tube was greatly dilated. The left ovary was normal but dislocated by the dilated Fallopian tube. A single cervix and vagina were evident.
The patient was admitted to our Department of Pediatric Surgery with suspected hematometra due to Müllerian duct anomaly. The girl was given a luteinizing hormone-releasing hormone analog (leuprolide acetate [Enanton®; Orion Corp., Espoo, Finland], 3.75 mg/monthly dose) in order to inhibit ovarian function, normal ovulation, and menstruation. A few hours after the first administration of the drug she had vaginal spots (dark coagulated blood). Symptoms improved after the introduction of Enanton, and we had time to perform another pelvic US that showed disappearance of the fluid left tube component (Fig. 1).

We decided to perform a contrast study. During hysterosalpingography (HSG) the right uterine horn became opaque soon after the retrograde insertion of contrast (Fig. 1). A Foley catheter helped us to increase pressure into the system and to point out the left uterine horn. The left Fallopian tube appeared closed (contrast distal blockage).
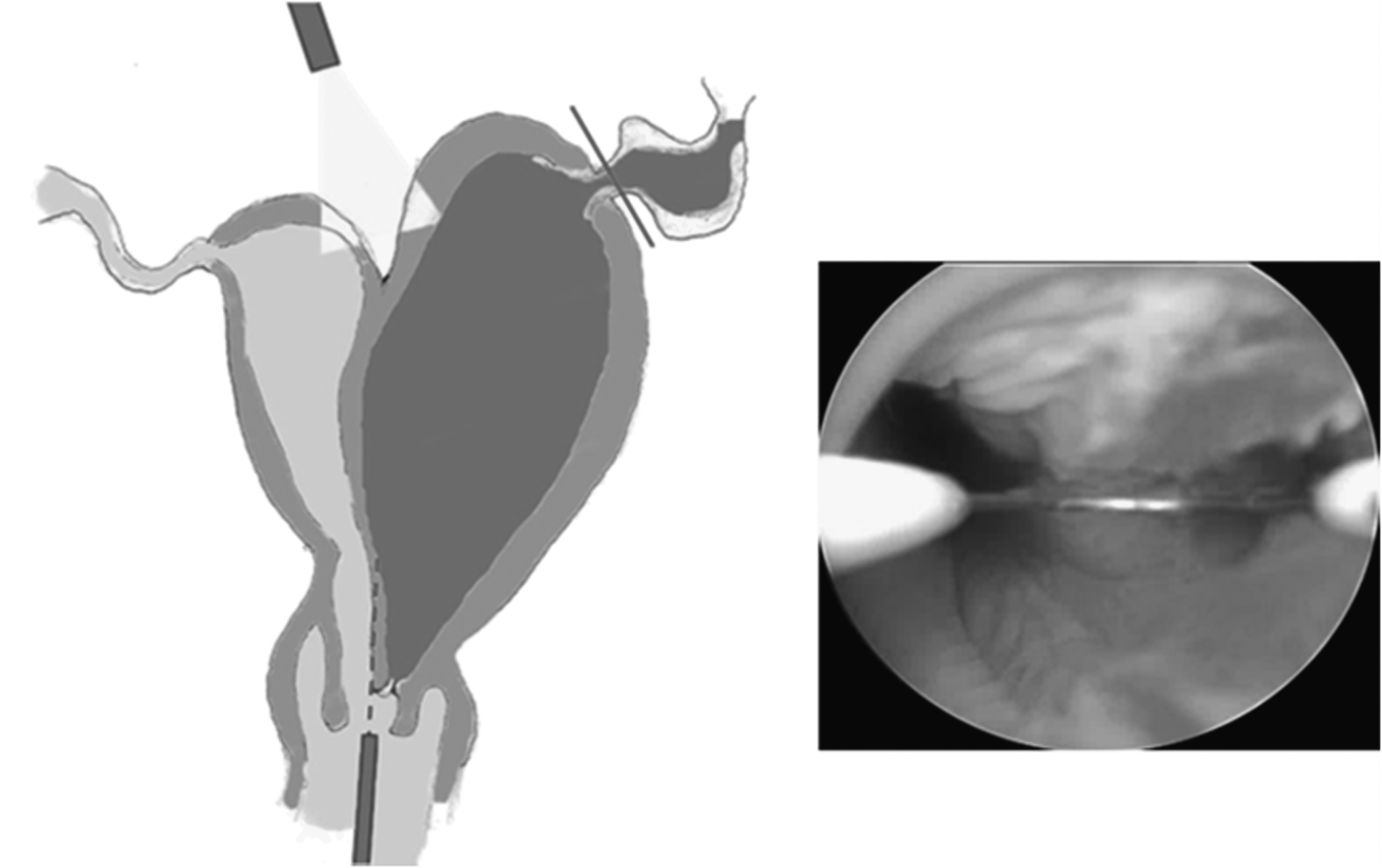
After careful imaging evaluation we decided on surgical intervention. We performed a combined hysteroscopic and laparoscopic approach (Fig. 2). We started with the laparoscopic procedure. A 5-mm port (for the optic) was inserted just below the umbilicus. The pneumoperitoneum was created with CO2 at a pressure of 10 mm Hg and a flow of 1 L/minute. Two 5-mm operative trocars were placed under direct vision in the right and left lower quadrants. The first step was the exploration of the abdominal cavity. We visualized a bicornuate uterus with a deep fundal depression that reached the middle third of the uterine corpus (Fig. 2); the left Fallopian tube and the left uterine horn were dilated, whereas the homolateral ovary was unremarkable. The right ovary, Fallopian tube, and uterine horn were normal. At the same time, a diagnostic hysteroscopy was performed with a 17 Ch, 30° cystoscope. The vagina appeared unique and regular. At the end of the vaginal canal there was a single external portion. After an initial single part (almost one-third of the entire length), the cervical canal split into two parts in the presence of an asymmetric fibrous septum (Fig. 2). The right hemicavity was easily accessible by the scope: it was a tubular canal with thin endometrium and regular tubal ostium. The left uterus was tortuous, and it had blood clots in it. The left tubal ostium appeared normal.
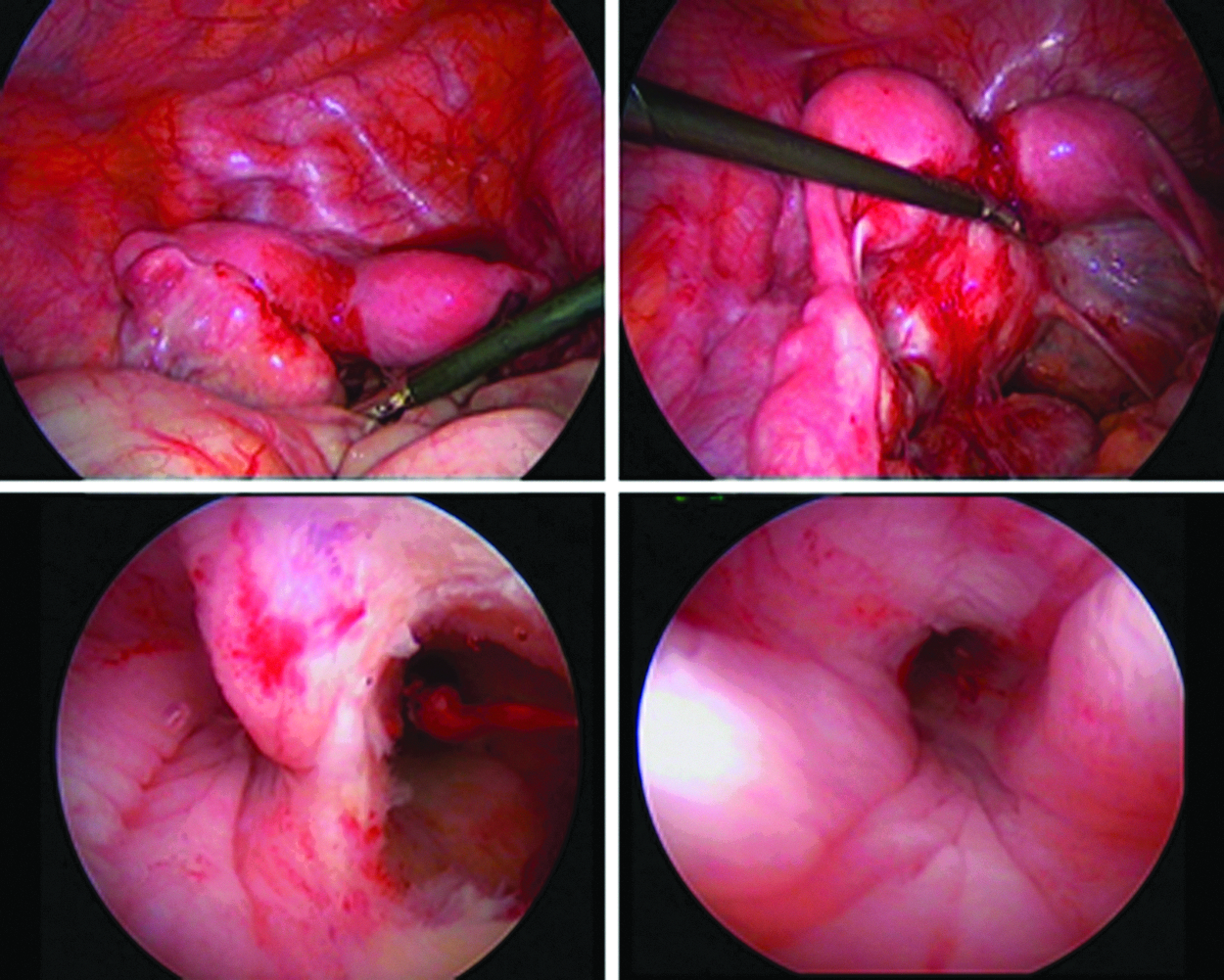
We decided to perform a septum resection under laparoscopic surveillance. We obtained cervical dilatation with 10 Ch Hegar bougies. Later a resectoscope was introduced into the left hemi-uterus, and the monopolar hook was used to perforate the septum near the cervical part. This maneuver facilitated the access to the left uterus. Laparoscopic surveillance helped as a reassuring guide. The resection was stopped when the residual septum was almost 0.5 cm long (Fig. 3).
Septum resection under laparoscopic surveillance.
The left tube appeared dilated and damaged. We replaced the umbilical trocar with a 10-mm one in order to remove the tube after endoloop ligation (Fig. 4).
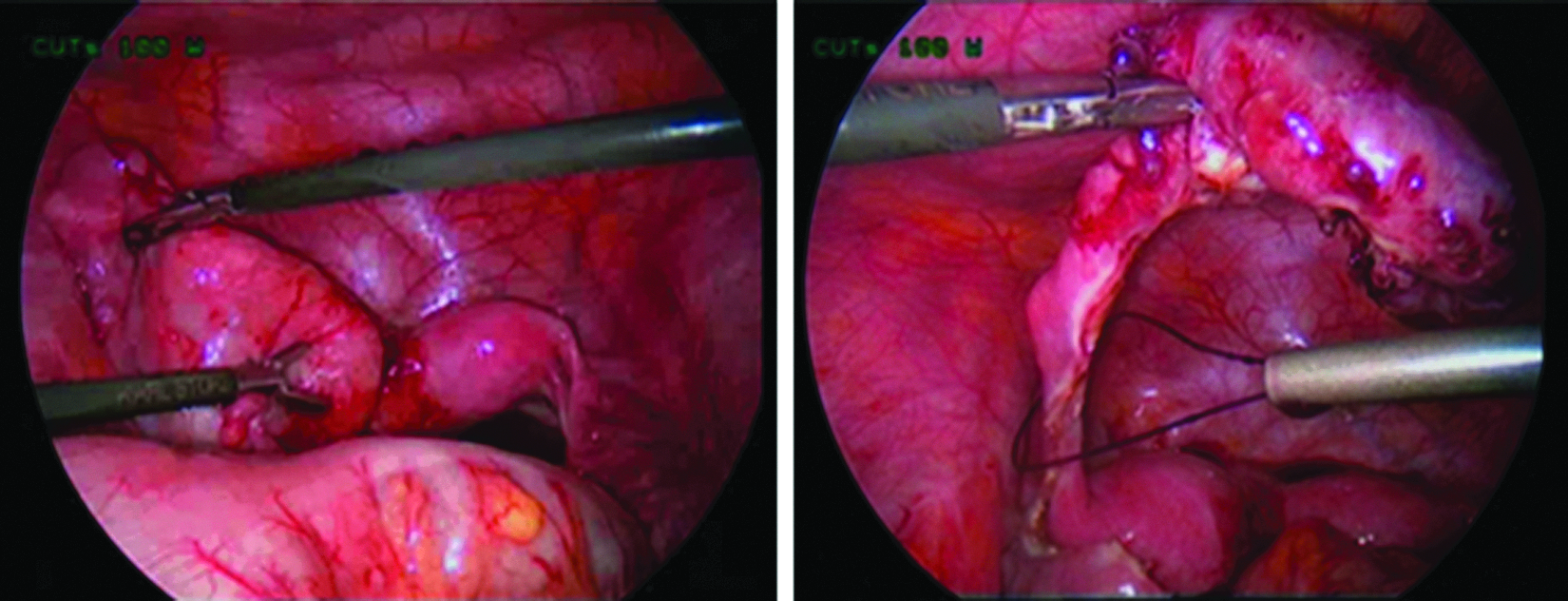
The left Fallopian tube appeared damaged, and it was resected after endoloop ligation.
The histological examination showed a chronic salpingitis with microscopic aspects of intraluminal tubal endometriosis. The overall operative time was 2 hours. There were no intraoperative or postoperative complications.
The girl was discharged on postoperative Day 2. Follow-up consisted of US and clinical evaluations at 1, 3, and 12 months after surgery. The menstrual cycle resumed after 5 months, and it was described as less painful and abundant. The patient is now doing well 2 years after surgery.
Discussion
Müllerian duct anomalies span a wide spectrum of genital tract defects resulting from inapt development, lack of fusion of the Müllerian ducts, or failure of resorption of the uterine septum. In particular, the altered incomplete union of the two Müllerian ducts results in a bicornuate uterus that can be associated with the persistence of the uterine septum, producing a hybrid entity. The overall incidence of these defects is approximately 0.001%–10% of women in the general population 2 and 8%–10% in women with a history of adverse pregnancy outcomes. The uterus is involved in almost all cases (90%). 3 Congenital malformations of the genital tract may be associated with urinary tract anomalies because they share a common origin. For instance, uterine malformations with unilateral renal agenesis have previously been reported in the literature. 4 The most frequent variety is the double uterus with an obstructed hemivagina and ipsilateral renal agenesis (Wunderlich–Heryn–Werner syndrome).
The most common method to sort these defects is the AFS classification, 1 which is clear and simple, but it has the disadvantage of not including hybrid varieties such as the bicornuate septate anomaly. 5 These abnormalities are often recognized after the onset of puberty. They may be symmetric or asymmetric and may or may not cause obstruction. For example, in the HSV uterus menstrual retention may cause bilateral or unilateral obstruction and dilatation associated with progressively increasing pain. 5 Obstructed asymmetric anomalies are the most common in pediatric patients.
In our case report the patient had left uterus obstruction that led to left tube distension and distortion along with clinical manifestations (abdominal pain and menstrual alterations). The high level of obstruction (uterine cervix) is rare, but it was the cause of acute symptoms because of the loss of the reservoir-like action of the duplicated vagina to accommodate the menstrual blood.
All the congenital anomalies are a spectrum, but we can still group them to understand each other and especially for their follow-up. This is a spectrum of an obstructed duplicated uterus with one cervix and one vagina.
We agree with other colleagues who state that accurate evaluation of the patient is mandatory and should not be limited to imaging findings. For instance, the presence of a fundal depression is not always the indicator of the pure or isolated bicornuate variety.5,6 Moreover, the pure septate uterus may present a mildly concave border that should not be >1.0 cm. 7 HSG can be useful to evaluate the cervical canal, uterine cavity, and Fallopian tubes but does not allow the visualization of the external uterine anatomy. Pelvic MR imaging is the technique of choice for the evaluation of these girls. It provides important details regarding not only the uterus but also other pelvic structures (Fallopian tubes and ovaries), and it helps to differentiate various uterine malformations.2,7 MR is also harmless for the patient. US scans are more manageable, and they find their role in the initial evaluation and in future follow-up. In our case MR evaluation helped us to identify the left ovary that was missed at US. In order to understand more about the anatomy of the girl we performed HSG. The contrast study added some details regarding the uterine horns and the presence of left side obstruction. In particular, it was useful to assess the patency of the left Fallopian tube. In these cases hysterosalpingosonography has been suggested as a less invasive alternative to HSG. 8
The differentiation of these anomalies (pure bicornuate uterus, pure septate uterus, and hybrid entities) is important because it affects the type of surgical procedure. Selected cases of pure bicornuate uterus are managed with uterus metroplasty (even if the treatment of choice remains the conservative one), and the presence of a septum is excluded with an intraoperative hysteroscopy. The pure septate uterus requires a hysteroscopic resection under laparoscopic surveillance.9–13 Surgery should be planned after a careful review of imaging if the patient's conditions remain stable. In our experience medical suppression guaranteed us additional time relieving the girl's abdominal pain: at first the presence of a pure bicornuate uterus (on the basis of ultrasound findings) was speculated. The MR and HSG evaluation helped us to identify the presence of a double uterus with fundal depression and obstruction of the left part. These findings led us to perform endoscopic evaluation to rule out the presence of a uterine or vaginal septum. We performed a combined hysteroscopic and laparoscopic treatment, as the literature recommends performing in the case of obstructed uterine duplications.3,5,10.14 Although hysteroscopy is a well-known procedure to treat uterine nonobstructive septums in adults, there were no previous reports of this minimally invasive approach in the pediatric age group. The preliminary data in 5 patients treated with a combined procedure for the same reason we did supported the further use of this approach. 3 The combined approach permitted us to diagnose a hybrid uterine anomaly and to correct it during the same surgical procedure. Hysteroscopic septoplasty was executable because the depression did not exceed the upper one-third of the uterine corpus, as happens in these cases and not in pure bicornuate varieties. 6
Even if hysteroscopy is classically described as a safe procedure, it is not completely free from the risk of uterine perforation. This is particularly true when there is a central uterine depression, as happens in HSV. It is thus important to keep an eye on the wall outside the uterus. The US evaluation lacks complete satisfaction to detect uterine leakages. 6
Laparoscopy is a procedure that achieves the aim with the advantages of a minimally invasive technique. Laparoscopy also permits the differentiation between uterine malformations and the exploration of the abdominal and pelvic cavities searching for endometriosis, associated anomalies, or tubal/pelvic damage.
Hysteroscopic resection of the cervical part of the septum should be performed with great care because of the risk of cervix damage. Indeed, concerns have been expressed regarding the possibility of having cervical incompetence during pregnancy. 15 Actually, most patients with a bicornuate uterus already have a cervical incompetence that is difficult to estimate. In the case of future pregnancy they therefore require close monitoring for the risk of preterm delivery, early or late miscarriage, fetal death, dystocia, and malpresentation.16,17
We decided to remove the damaged Fallopian tube in order to reduce future risks of impairing implantation and/or embryo development. The tubal factor portended an increased risk of miscarriage, and it is associated with preterm delivery and low/very low birth weight. 18 In these cases salpingectomy is therapeutic, and it is associated with a lower potential risk of ectopic pregnancies than salpingostomy or salpingoplasty, 19 without compromising the ovarian function and in vitro fertilization–embryo transfer outcomes. 20 The tube had a tenacious distal occlusion, and microscopic examination showed degenerative aspects incompatible with normal future function. Given the sensitivity of the issue, the decision to remove the tube should be carefully evaluated. Each case has its own characteristics, and it would be wrong to make generalizations about it. In the last decade the role of laparoscopy has greatly improved, and nowadays it is both diagnostic and therapeutic. 9
Conclusions
In conclusion, the present report focuses on the need for a revision of the AFS classification as advocated by many authors.5,6 We believe that, as for vaginal malformations, 21 a new simpler and satisfactory classification of uterine congenital disorders should be proposed because hybrid entities are specific anomalies requiring their own management. The combined laparoscopic and hysteroscopic approach allows us to confirm the diagnosis and to safely correct the malformation. Larger studies are still required to better understand long-term outcomes and to estimate the real incidence of the hybrid anomalies.
Footnotes
Disclosure Statement
No competing financial interests exist.