
Abstract
Abstract
Background/Purpose:
Choledocholithiasis is uncommon in the pediatric population. Techniques for common bile duct stone extraction are still not well established. This article aims to describe safe and applicable techniques for pediatric common bile duct exploration.
Materials and Methods:
This was a retrospective review of a prospectively maintained database of two pediatric surgeons for patients undergoing laparoscopic common bile duct exploration at two tertiary-care centers from April 2008 to March 2012.
Results:
For 39 patients under 15 years of age undergoing laparoscopic cholecystectomy, 10 cholangiograms were performed, and 8 were found to have filling defects. Seven patients underwent successful laparoscopic common bile duct exploration with documentation of stone clearance, and 1 patient was sent for postoperative endoscopic retrograde cholangiopancreatography with stone extraction. Eleven patients had cholecystectomy performed by single-incision laparoscopic surgery, but none of these had cholangiograms or common bile duct explorations. Various methods of stone clearance were used, including the use of saline flush, balloon catheters, nitinol stone extractors, and the aide of glucagon. Depending on patient size, a choledochosope or a ureteroscope was used. There were no complications and no conversions to open surgery.
Conclusions:
Laparoscopic common bile duct exploration is feasible in the pediatric population, using many of the instruments readily available in the standard operating room. With an armamentarium of tools and techniques, the method of stone extraction can be tailored to the patient and situation.
Introduction
C
Materials and Methods
After obtaining institutional review board approval, we conducted a retrospective database study of laparoscopic common bile duct exploration and stone clearance performed by two pediatric surgeons from April 2008 to March 2012. The operative case logs of the surgeons were reviewed for laparoscopic cholecystectomy with concomitant common bile duct exploration and stone clearance. Single-incision laparoscopic cases were included. Patients were excluded if they were older than 14 years of age. Operative reports were then examined to describe the successful techniques. Patient characteristics such as age, weight, and comorbidities were reviewed, as well as preoperative laboratory and imaging studies. Outpatient follow-up records were also reviewed to detect any late complications.
Results
39 patients who underwent laparoscopic cholecystectomy. An intraoperative cholangiogram was performed in 10 patients, 3 months to 13 years of age. Cholangiograms were selectively performed on patients with a history of abnormal liver function tests, gallstone pancreatitis, or dilated common bile duct on preoperative ultrasound. Only one cholangiogram was unsuccessful; the 4-year-old patient had no postoperative complications and no evidence of a retained stone. Eight patients were found to have choledocholithiasis by intraoperative cholangiogram. Laparoscopic common bile duct exploration was performed with successful stone clearance noted by completion cholangiogram or direct scope visualization of the common bile duct in 7 patients. In the eighth patient, the surgeon elected not to perform a common bile duct exploration because of the diminutive size of the cystic duct. The patient was therefore referred for and had a successful postoperative ERCP to clear the stone. Eleven cholecystectomies were performed by single-incision laparoscopic surgery, but none of these patients had an indication for a cholangiogram, and there was no evidence of choledocholithiasis. There were no complications, including bleeding, pancreatitis, perforation, or conversions to open surgery. There were no patients found to have postoperative retained stones, including those who did not undergo cholangiography. All patients had preoperative liver function tests but did not routinely have postoperative laboratory studies. None of the patients undergoing laparoscopic common bile duct exploration received preoperative ERCP or required postoperative ERCP for a retained stone. The average length of stay was 3.28 days (range, 1–7 days), and the average total operating time, noted by the circulator as time in and time out of the room (not skin to skin), was 211 minutes (range, 122–322 minutes) (Table 1).
F, female; M, male; OR, operating room.
The number and size of stones extracted by common bile duct exploration varied per patient. All but 1 patient had round bilirubin stones, with the exception having small flaky stones. The intraoperative cholangiograms were achieved using either a Reddick® (LeMaitre, Burlington, MA) or Taut® (Teleflex Medical, Triangle Park, NC) catheter. The operating theater setup is depicted in Figure 1. A transcystic duct approach was used in all cases. The preferred method for stone clearance in all cases with an abnormal intraoperative cholangiogram at our institution was direct visualization with a choledochoscope via the transcystic approach with the 7.5 French choledochoschope (Karl Storz, Tuttlingen, Germany) or the 8.7 French adult or 7.2 French pediatric ureteroscope (Gyrus ACMI, Southborough, MA). The scope type was chosen based on patient habitus, with the smaller ureteroscope used for more diminutive ducts (Table 2). In all patients, a pressurized saline system was used to flush the stones. For smaller children, the cystic and common ducts were flushed with saline alone. For older patients the flexible ureteroscope with standard urologic stone extraction baskets or 1.5-mm nitinol stone extractors were used to either extract the stones or to crush and then flush the stones retrograde out through the cystic duct or antegrade through the ampulla of Vater. Other mechanical methods of clearing the stones included the use of embolectomy catheters to withdraw the stones from the cystic duct or push them into the duodenum. In the case of the 9 year old, the scope was used to mechanically push the stones into the duodenum. The use of weight-based dosed glucagon aided in ampullary relaxation and in stone clearance for 3 patients. In some patients the addition of a fifth port and an additional surgeon or assistant were useful.
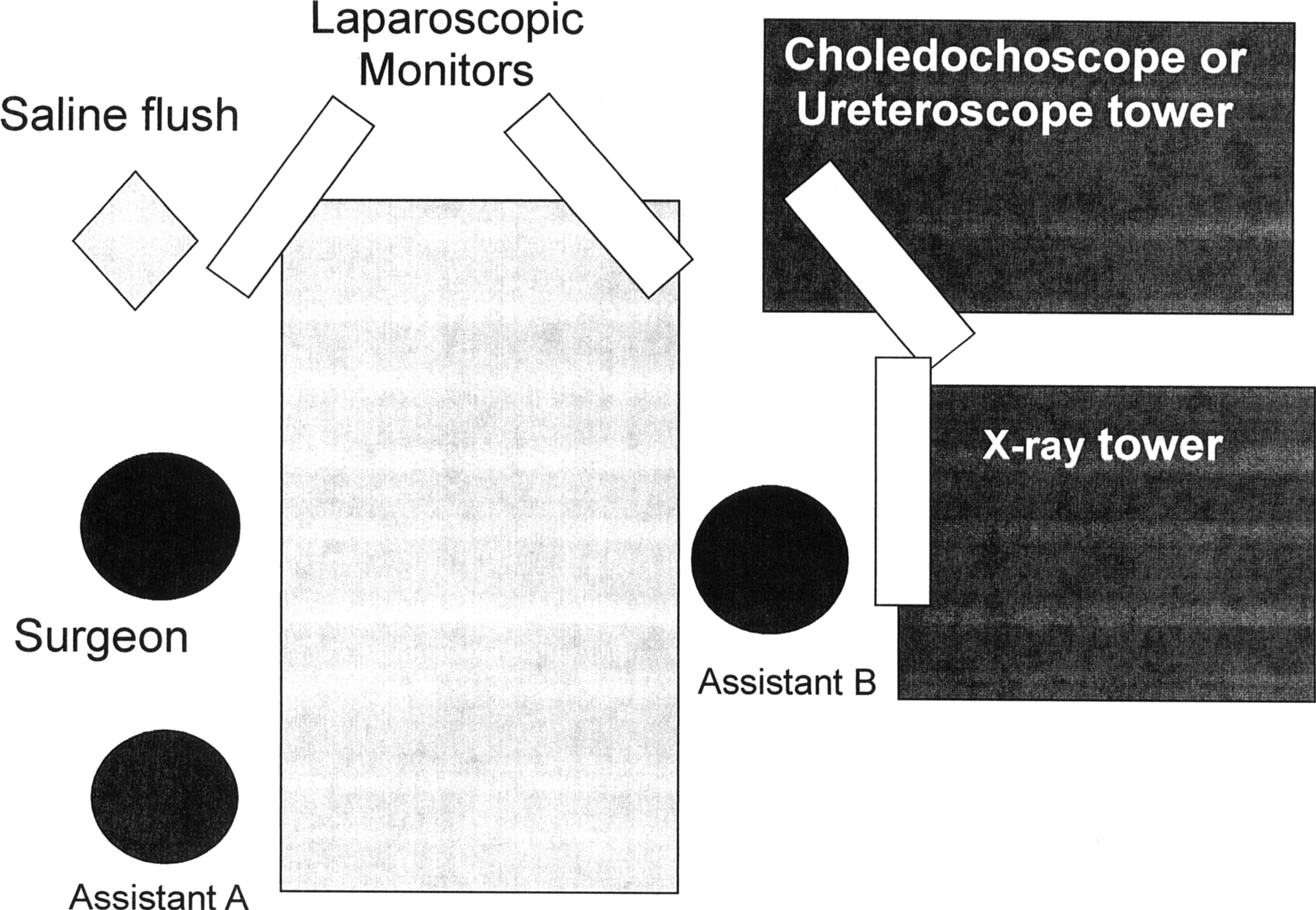
During common bile duct exploration, the surgeon operates the choledochoscope and laparoscopic instruments. Assistant A assists with insertion of the choledochoscope and operation of the flush and baskets. Assistant B holds the laparoscope and retraction instruments.
F, female; M, male.
Discussion
Various techniques can be used for exploration and clearance of common bile duct stones, which can be a challenging task in small children. Many of the tools described are readily available in a standard operating room. Creating a cholangiography or common bile duct exploration kit may aid unfamiliar operating room personnel with the equipment required. As this procedure is not commonly performed, the finding of a common bile duct stone on the cholangiogram puts in motion the need to gather the equipment needed for the common bile duct exploration. There is often a delay while operating room personnel who are unfamiliar with the equipment required search for the proper tools. Therefore we created a kit to reduce waiting time in the operating room. The kit includes the following: a Reddick scoop-tip stiffer cholangiogram catheter, Taut cholangiogram catheters (4.5 French and 5.5 French), 30-mL syringes, a bag decanter, 0.9% sterile saline with a high-pressure flush system, a rubber nipple for the scope, and the System ONE™ common bile duct exploration kit (Teleflex Medical) (Fig. 2), which includes a Titanium4™ retrieval basket, Softwire™ guidewire, Trifecta™ multipurpose balloon catheter, high-pressure syringe, and percutaneous introducer. In our hands, this level of organization reduced our total operating room times substantially toward the end of the series.
Taut System ONE common bile duct exploration kit. Image available at www.weckcatalog.com/weck/products/9913
Recommendations for successful clearance of the stones include the addition of a fifth port in the left upper quadrant to guide the scope into the cystic duct. If it is anticipated even before the cholangiogram that a common bile duct stone may be present, placing the right upper quadrant working port closer to the costal margin and slightly more lateral than usual will improve the angle at which the scope enters the cystic duct. The primary surgeon stands on the patient's right side to operate the choledochoscope or ureteroscope and extraction tools. The addition of a second surgeon or assistant was also useful, standing on the left side to operate the laparoscope and laparoscopic instruments. Placing a second monitor over the patient's left shoulder allowed for simultaneous visualization of the intraabdominal laparoscopic instruments and the choledochoscope image by the choledochoscope operator.
In cases of a small cystic duct, the duct can be dilated with an internal balloon catheter and/or incised more distally, closer to the common bile duct. With regard to the extraction of the stones, a pressurized bag of saline with a three-way stopcock for flushing was very useful, as was the use of glucagon for sphincter relaxation. Various devices were used to mechanically crush and clear the stones such as an embolectomy catheter or nitinol basket. Another option was to directly push the stones with the scope. Often more than one device may be needed.
In this series we observed a higher rate of choledocholithiasis as 8 of 39 (20.5%) cholecystectomy patients showed common bile duct stones on intraoperative cholangiography. This number may be higher than historical figures because, in this practice, younger patients with cholelithiasis are frequently observed until they become symptomatic. Therefore, the patients who are selected to undergo an operation have a higher probability that they have passed stones into the common duct, compared with the average patient with cholelithiasis. As our pediatric surgeons typically care for patients 14 years of age and younger, the indication for cholecystectomy is also different than in an older patient who may have acute or chronic cholecystitis, and therefore a greater proportion have choledocholithiasis.
We noted that none of the patients who underwent single-incision laparoscopic surgery had an intraoperative cholangiogram performed. This is likely due to selection bias as these patients tended to be older, with the indication of cholecystitis rather than choledocholithiasis or other pathology. If there was suspicion of choledocholithiasis the surgeon may have opted for a standard laparoscopic cholecystectomy.
In summary, choledocholithiasis is infrequently encountered in the pediatric patient, but when required a laparoscopic common bile duct exploration is feasible using tools that are readily available in the standard operating room. Successful operative clearance also spares an additional procedure and the cost of ERCP.
Footnotes
Disclosure Statement
No competing financial interests exist.