
Abstract
Abstract
Background:
Recently, single-port surgery for colon cancer has been increasingly attempted. However, prospective studies investigating the efficacy of single-port colectomy for colon cancer are lacking. The aim of this study is to determine whether single-port colectomy for sigmoid colon cancer is a safe and effective surgical option.
Subjects and Methods:
Forty-eight patients were enrolled for this prospective single-arm Phase II trial. All patients underwent single-port laparoscopic-assisted sigmoidectomy through the umbilicus. The primary outcome was the number of retrieved lymph nodes. Secondary measures included the conversion rate, postoperative morbidities, mortalities, and short-term clinical outcomes.
Results:
The mean number of retrieved lymph nodes was 21.1 (95% confidence interval, 18.1–23.99). The conversion rate was 14.6% (open conversion, 4.2%), and the overall proportion of morbidity was 31.2%. The majority of complications involved wound problems (18.8%); the mortality rate was 0%. The median postoperative hospital stay was 8 days (range, 7–12 days), and the median time from surgery until the first episode of flatus was 3 days (range, 1–5 days).
Conclusions:
Single-port colectomy for sigmoid colon cancer is safe and oncologically feasible in selected patients. Considering the relatively high conversion rates, improvement of the instruments for single-port colectomy is needed.
Introduction
Subjects and Methods
Study design
We designed a single-arm Phase II trial of single-port colectomy for sigmoid colon cancer. The study was conducted in the Center for Colorectal Cancer of the National Cancer Center Hospital, Goyang, Korea. The trial was conducted from January 2011 through August 2011. The study was reviewed and approved by the Institutional Review Board of the National Cancer Center (protocol number NCCCTS-10-484). All of the patients provided written informed consent.
Patients
Patients were eligible if they were >18 and <80 years old, had been diagnosed with sigmoid colon cancer proven by pathology, had adequate bone marrow function (hemoglobin, ≥10 g/dL; white blood cell count, ≥3000/mm3; platelet count, ≥100,000/mm3) and kidney function (serum creatinine ≤1.5 mg/dL), had no evidence of heart or lung dysfunction, and signed a written informed consent. Candidates were excluded if they had distant metastases, had a large tumor (larger than 5 cm in diameter as measured by colonoscopy or computed tomography), had a tumor with other organ invasion, had an intestinal obstruction or a stent insertion, used steroids, required emergency surgery, exhibited mental impairment, had a history of other organ cancer (except those with radical excisions for skin cancer) or other serious disease, or had a contraindication for surgery.
Study intervention
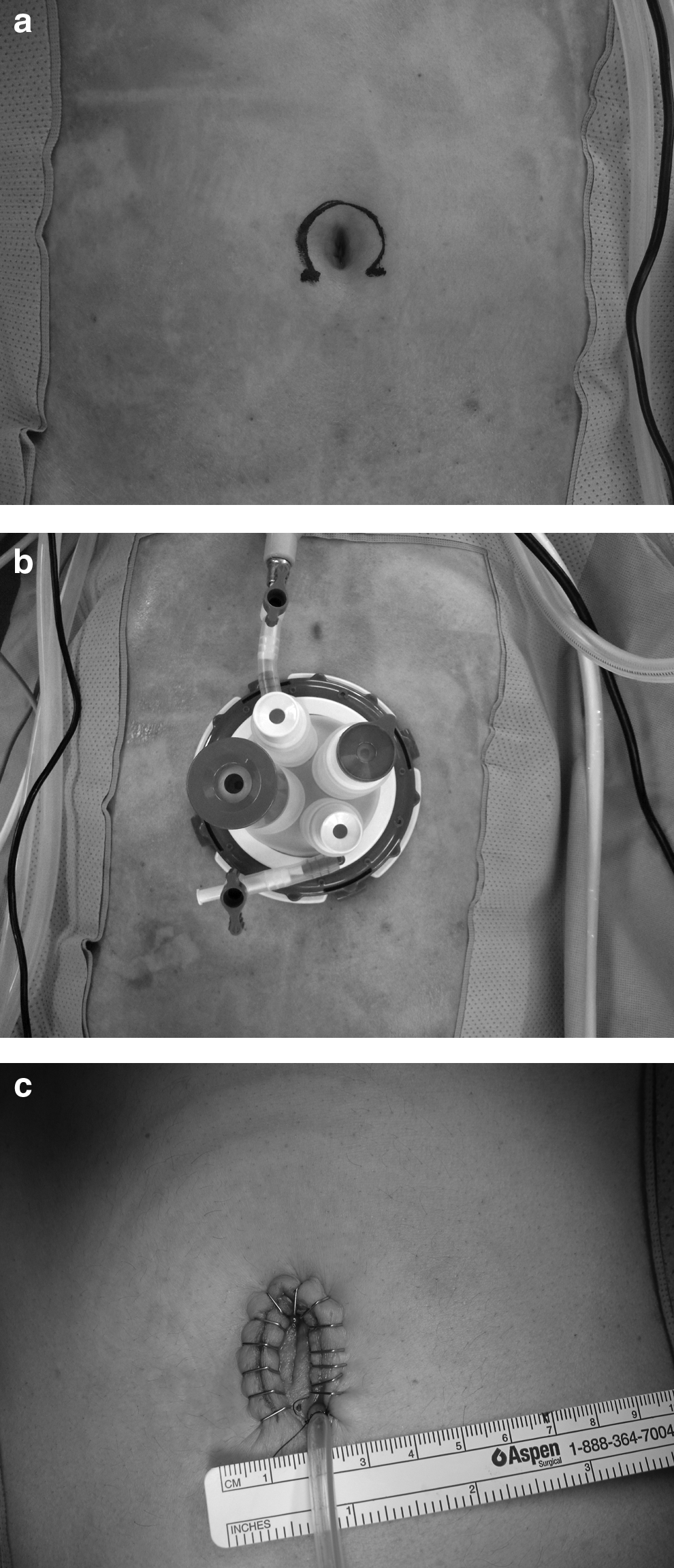
The surgical team had adequate experience in conventional multiport laparoscopic-assisted colectomy. Three surgeons who participated in the present study had sufficient experience (over 500 cases) with conventional laparoscopic colorectal surgery. The operations were performed with the patients under general anesthesia in the Trendelenburg position, tilted to the right. The operator and scopist stood to the right side of the patient. We used a modified umbilical incision for single-port insertion, as described by Casciola et al. 8 The umbilical cutaneous incision was made three-fourths of the way along the circumference of the umbilicus in a circular shape (Fig. 1a). A fascia incision was made in a cranium caudal direction. After the second half of the study period, we modified the incision into a 2-cm vertical transumbilical incision because of wound problems. A four-channel single port (OCTO™ port; Dalim Surgnet, Seoul, Korea) was inserted though the umbilical incision (Fig. 1b). Under pneumoperitoneum with CO2 gas at a maximum of 12 mm Hg, the peritoneal cavity was explored using laparoscopy.
Operative photographs:
To reduce the collisions between the instruments and the camera, we used a 5-mm diameter, 45-cm long, 30° angled laparoscope with a 90° angled light cable adaptor (Stryker Endoscopy, San Jose, CA). Because the surgical instruments were also positioned at a parallel angle, we used an articulated grasper (Roticulator™; Covidien, Mansfield, MA) or a double-curved grasper (Olympus, Tokyo, Japan) in the nondominant hand. In the dominant hand, the monopolar electrosurgical instrument (ENDOPATH® Probe Plus® II system; Ethicon Endo-Surgery, Cincinnati, OH) or the Ultracision® Harmonic® scalpel (Ethicon Endo-Surgery) was used.
The sigmoidectomy was performed using a surgical technique similar to that in a standard laparoscopic procedure. The main approach was from medial to lateral. First, the inferior mesenteric vessels were identified and ligated with endoclips. By continuing the posterior dissection along the plane of the embryonic attachment between Toldt's and Gerota's fasciae, the descending and sigmoid colon were mobilized. During the mobilization of the colon, a ligating loop (Surgitie™; Covidien) was applied at the proximal colon to the tumor site. Pulling the threads of the loop facilitated the traction of colon through a single port. After the pathological part of the colon had been completely mobilized and the mesentery was divided by a Harmonic scalpel, a linear stapling device was used to transect the colon in a tangential fashion.
The specimen was extracted through the umbilical incision. The corresponding segment of the bowel and mesentery were divided. A purse-string suture was placed, followed by insertion of the anvil of a CDH29 circular stapling device (Proximate ILS™; Ethicon Endo-Surgery) in anticipation of the anastomosis. The pneumoperitoneum was re-established. Under direct visualization, a circular stapled anastomosis was completed. After the insertion of a drainage tube though the umbilical incision, the wound was closed, layer by layer (Fig. 1c).
Outcomes measures
The primary end point of the study was the number of retrieved lymph nodes. The surgical specimens were examined by one specialized pathologist (H.J.C.) with assessor blinding. In the assessment of the lymph nodes, all mesocolic fat was thoroughly dissected to identify the lymph nodes. Secondary measures included conversion rate, postoperative morbidities, mortalities, and short-term clinical outcomes. Conversion was defined as any conversion to open or laparoscopic surgery. The conversion to an open surgery was defined as an unplanned extension of the incision above the length for specimen extraction. Conversion to laparoscopic surgery was defined as the insertion of an additional port. Postoperative morbidities were defined as events that required specific medical or surgical treatment within 30 days postoperatively.
Perioperative pain was assessed preoperatively and 1, 2, and 3 days after surgery through a visual analog scale (VAS) and the present pain intensity index (PPI). 9 Quality of life was measured preoperatively and at 3 weeks and 3 months after the surgery using the validated Korean version of the European Organisation for Research and Treatment of Cancer QLQ-C30 questionnaire (version 3.0) and the colorectal cancer module QLQ-CR38.10,11
Statistical analysis
A single-arm design was used to investigate whether the number of retrieved lymph nodes was sufficient in single-port colectomy for sigmoid colon cancer. In our previous study of laparoscopic surgery, the mean number of harvested lymph nodes was 23, with a standard deviation (SD) of 11. 12 The precision-based sample size calculation was performed so that the allowable margin of error would be 3.7 (30% of the SD) at a 95% level of confidence. To achieve this goal, 43 patients were required. Allowing for a 10% loss to follow-up, the recruitment size was set at 48.
Time-course data (scores for pain and quality of life) were analyzed using repeated-measures analysis of variance. A two-sided P<.05 was considered to be statistically significant.
Results
Seventy-six patients who had sigmoid colon cancer were eligible for study. Among these patients, 28 were excluded. In total, 48 patients were included in this trial (Fig. 2). The median age of the 48 patients was 61 years (range, 35–75 years); there were 28 (58.3%) males. The mean±SD body mass index of the patients was 24.73±3.45 kg/m2. Pathological examination showed that 14 cases (29.2%) were stage I, 12 cases (25.0%) were stage II, 21 cases (43.8%) were stage III, and 1 case (2.1%) was stage IV. In a patient with stage IV disease, the enlargement of para-aortic lymph nodes near the inferior mesenteric artery was incidentally detected during the operation, and the enlarged lymph nodes were removed by a single-port approach. In the final pathology, these nodes were confirmed as metastatic lymph nodes. The mean±SD size of the tumor was 3.63±2.11 cm.
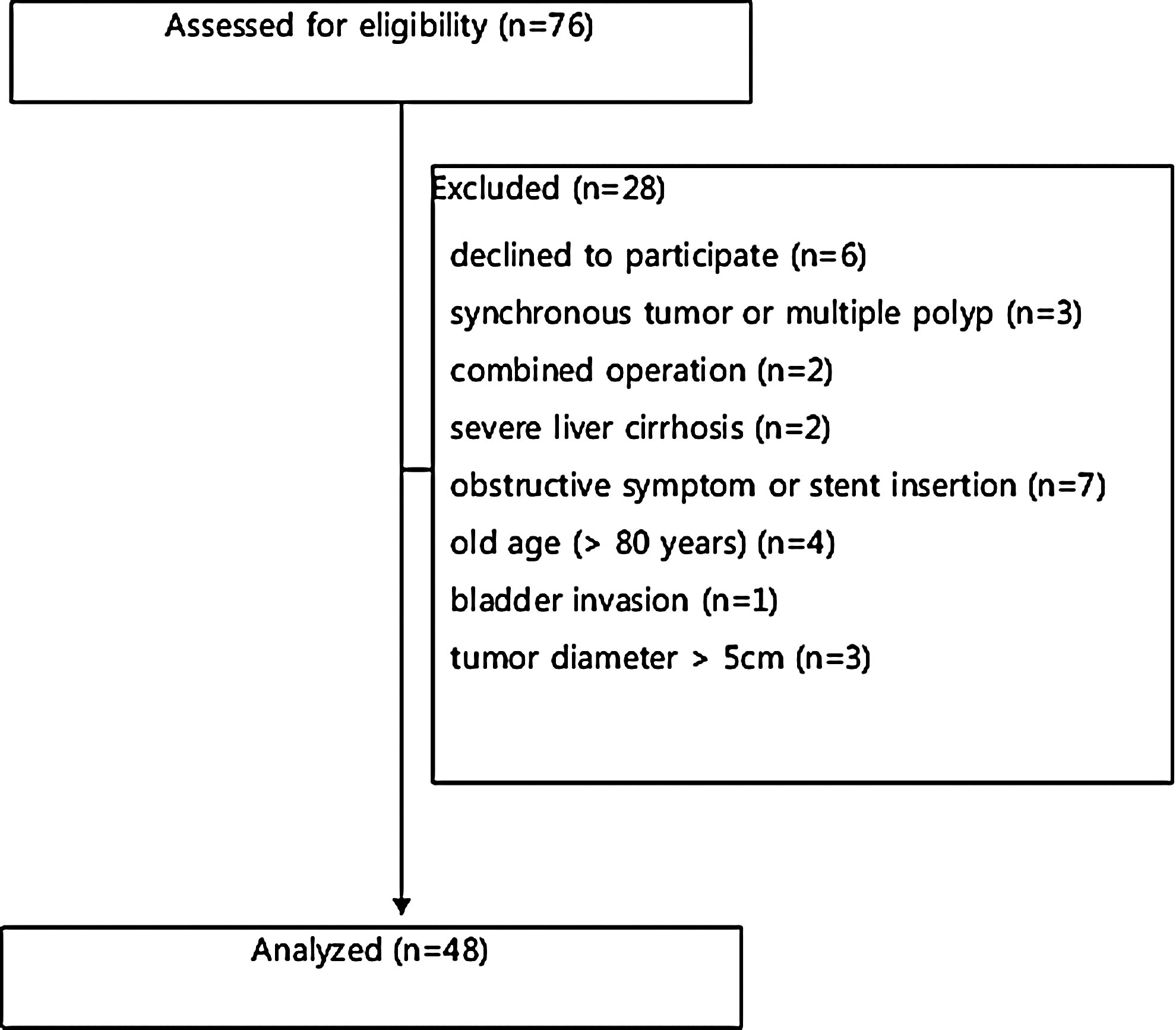
Trial profile.
Table 1 shows the short-term surgical outcomes. As the primary end point, the mean±SD number of retrieved lymph nodes was 21.1±10.0 (95% confidence interval, 18.1–23.99). The median incision length was 4 cm. The mean operating time was 168.2 minutes. The average amount of blood lost during the operation was 76.6 mL, and no transfusion was required during the perioperative course. The total conversion rate was 14.6% (laparoscopic conversion, 5 cases; open conversion, 2 cases). The reasons for conversion were small bowel injury, adhesion of tumor to the abdominal wall, a bulky tumor, and ambiguous anatomy. The two intraoperative events were injuries of the inferior mesenteric and sigmoidal arteries. These bleeds were controlled by a single-port approach without conversion.
Data are mean±standard deviation values unless indicated otherwise.
The overall proportion of morbidity was 31.2%. The majority of complications involved wound problems (18.8%), and the mortality rate was 0%. The median postoperative hospital stay was 8 days. The median time from surgery until the first episode of flatus was 3 days (Table 2).
Data are median [interquartile range (range)] values unless indicated otherwise.
Mean±standard deviation.
Over the time course of VAS and PPI scores, repeated-measures analysis of variance revealed that their changes with time were significant (df=2.3, F=43.13, P<.0001 and df=2.4, F=17.04, P<.0001, respectively). Both VAS and PPI scores peaked 1 and 2 days after surgery and significantly decreased at postoperative Day 3, compared with postoperative Days 1 and 2 (Fig. 3).

Forty-seven patients finished the baseline survey on quality of life, compared with 46 (95.8%) and 29 (60.4%) patients who completed the survey 3 weeks and 3 months, respectively, after surgery. In most QLQ-C30 scales, no statistically significant changes were observed, except in nausea and vomiting. The symptom scores of nausea and vomiting showed an increase as time progressed (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/lap). Among QLQ-CR38 scales, sexual function improved from 3 weeks after surgery. The scores on chemotherapy side effects increased at 3 months after the operation. In the symptom scale of weight loss, the symptom scores peaked at 3 weeks and returned to baseline levels at 3 months after treatment. The other scales were not significantly different over time (Supplementary Fig. S2).
Discussion
Advanced technology and accumulated experience in laparoscopic surgery have prompted surgeons to find less invasive methods than multiport laparoscopic surgery. Single-port laparoscopic surgery gained attention due to its reduced trocar numbers, better cosmesis, and, theoretically, its subsequently decreased rates of trocar-related complications and postoperative pain. Since single port laparoscopic surgery was first described by Remzi et al. 13 and Bucher et al. 14 in colorectal surgery in 2008, several retrospective case-comparison series and case series have reported its feasibility in patients with colorectal cancer. However, evidence from randomized studies has been limited to date,15,16 and even data from randomized studies were heterogeneous, covering both malignant and benign colorectal disease at different sites.
The present prospective Phase II trial showed that single-port laparoscopic colectomy for sigmoid colon cancer could be performed with the retrieval of an adequate number of lymph nodes (mean number of 21.1) and sufficient margins corresponding to oncologic principles and without significant intraoperative events. Although postoperative complications occurred in 15 patients (31.2%), most of them were wound complications; no major complications arose.
Wound complication was the most common morbidity in the present study (18.8%, 9/48). The obtained wound infection rate was higher than that of conventional laparoscopic colorectal surgery, according to our previous data (1.2%, 12/984). 17 We incised the abdomen in the manner described by Casciola et al. 8 during the first half of the study period. Using this method, we were able to obtain a larger space in the skin and subcutaneous layers, which often has limited the extraction of specimens, but the dead space between the cutaneous flap and the fascia seemed to cause frequent wound problems. After we changed from cutaneous incisions to 2-cm vertical transumbilical incisions, the wound problems decreased.
In the present study, the overall conversion rate was 14.6% (7/48); this outcome seems higher than that of previous studies for single-port surgery.18,19 However, because the previous results primarily came from small case series or case-comparison studies that were subject to significant bias in terms of patient selection and self-reporting of results, conclusions should be drawn cautiously. Among our conversion cases, 5 cases involved the simple placement of an additional trocar, and open conversions were only required in 2 cases (4.2%). In single-port laparoscopic surgery, the surgical instruments were parallel to one another, and freedom of motion was limited; these were among the usual comments on obstacles to single-port surgery. 20 Although we used articulated or curved laparoscopic instruments21,22 and crossover hand maneuvers22,23 to overcome these limitations, instrument crowding still caused the restriction of a specific range of motion and operative field. Tissue manipulation and fine dissection with properly sustained tension were easily obtained with one additional port in 5 cases. The development of optimal instruments for single-port laparoscopic surgery is considered to be necessary before its application is widely utilized. However, because the benefits of laparoscopic surgery were maintained even after the placement of additional ports, surgeons should not hesitate to insert an additional port to sustain definite operative planes for oncologic safety. Other possible reasons included that this could be related to the learning curve for single-port laparoscopic surgery. Even though all of the surgeons who participated in this trial had extensive experience with laparoscopic colorectal surgery, they had been exposed to fewer than 10 cases of single-port laparoscopic surgery before the study. Therefore, their conversion rates to conventional laparoscopic surgery might change after further experience.
This prospective study did not have a control group, which, according to previous retrospective comparative studies, would typically have been a conventional laparoscopic group; therefore, it is impossible to directly compare single-port laparoscopic surgery with conventional laparoscopic surgery. We designed the study to determine whether single-port surgery could be performed safely in colectomy for sigmoid colon cancer, and we showed that single-port laparoscopic colectomy was both oncologically and surgically feasible in malignant disease in experienced hands. However, further large multicenter randomized trials are needed to establish the actual benefits of this procedure over conventional laparoscopic surgery, such as reduced postoperative pain, a lower risk of hernia or intraperitoneal organ injury, and better cosmesis as well as to determine its clear value over conventional laparoscopic surgery. Compared with conventional laparoscopic surgery, single-port surgery has merit in reducing manpower resources.
Regarding quality of life, most scales did not change after single-port surgery except for nausea and vomiting, chemotherapy side effects, weight loss, and sexual function. Worsened symptoms, including nausea, vomiting, and chemotherapy side effects, may be related to the adjuvant chemotherapy. Indeed, sexual function improved 3 weeks after the operation. In this study, quality of life was not worsened by single-port surgery.
Thus single-port colectomy for sigmoid colon cancer is safe and oncologically feasible. The results of this study warrant a Phase III randomized trial comparing conventional laparoscopic and single-port colectomy for sigmoid colon cancer.
Footnotes
Acknowledgments
This study was supported by a grant from the National Cancer Center (NCC-1210170).
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.