
Abstract
Abstract
Background:
Optimal surgical treatment of infants with esophageal atresia (EA) and tracheoesophageal fistula (TEF) remains controversial. In order to better understand variability in management, we surveyed the International Pediatric Endosurgery Group (IPEG) membership.
Materials and Methods:
An online-based survey, conducted in 2012, was sent to all IPEG members.
Results:
The survey was completed by 170 surgeons from 31 countries. A majority of respondents practiced in academic/university settings (86%) and performed one to three EA/TEF repairs annually (67%). Those practicing for over 15 years made up 39% of the study group, followed by those practicing 6–10 years (24%), 0–5 years (22%), and 11–15 years (15%). Utilization of a thoracoscopic approach was reported by half of the respondents with a frequency of 1–3 cases (76%), 4–6 cases (17%), and greater than 7 cases (7%) per year. Low birth weight, congenital heart disease, long gap length, and compromised physiologic status were identified as the most common exclusion criteria for thoracoscopic repair. The thoracoscopic repair was almost uniformly performed via an intrapleural approach (96%), in contrast with the open repair that was done extrapleurally in 89%. Preoperative bronchoscopy was routinely performed by 60%. Size 4-0 to 5-0 absorbable suture predominated for EA repair. Postoperative chest tube/drain and transanastomotic tube placement were used by 83%. A normal esophagram was required by 85% to initiate oral feeding. Sixty-six percent initiated transanastomotic feeds prior to obtaining an esophagram. Postoperative antibiotic use was common (76%) and varied from less than 1 to greater than 14 days. Acid suppression medication was used by 76% with duration ranging from 7 days to lifelong. For long gap EA, spiral myotomies were rarely performed (10%), and gastric transposition was the favored method for esophageal replacement (66%).
Conclusions:
Considerable variability existed among the IPEG membership in treatment of patients with EA/TEF. The identification of variance is the first step in creating future studies to identify best practices.
Introduction
In addition to operative approach, there appears to be variability in the technical aspects of the operation as well as the postoperative management of these patients. However, the degree of variability in the surgical care of EA and EA/TEF patients worldwide is unknown. In order to clarify the distribution of current practice patterns, we surveyed the International Pediatric Endosurgery Group (IPEG) membership. The primary goal of this study was to identify practice options and variation in the management of patients with EA/TEF.
Materials and Methods
An online-based survey was conducted in 2012 and sent to all IPEG members. The survey was composed of demographics, operative approach, operative techniques, postoperative management, long gap maneuvers, and management of strictures. After development, the survey was circulated among the IPEG Research Committee for further development. The survey was sent via e-mail to all current IPEG members in three rounds of deployment.
Results
Demographics
The survey was sent to the 579 registered e-mail addresses, with responses from 170 surgeons from 31 countries. The continental distribution of responses is shown in Figure 1. The large majority (86%) reported they practiced in an academic or university setting; 10% practiced in an urban community practice, with the remainder in a rural or other type of environment. Pediatric surgery practice experience ranged from over 16 years (39%), 10–15 years (15%), 5–9 years (24%), and less than 5 years (22%).
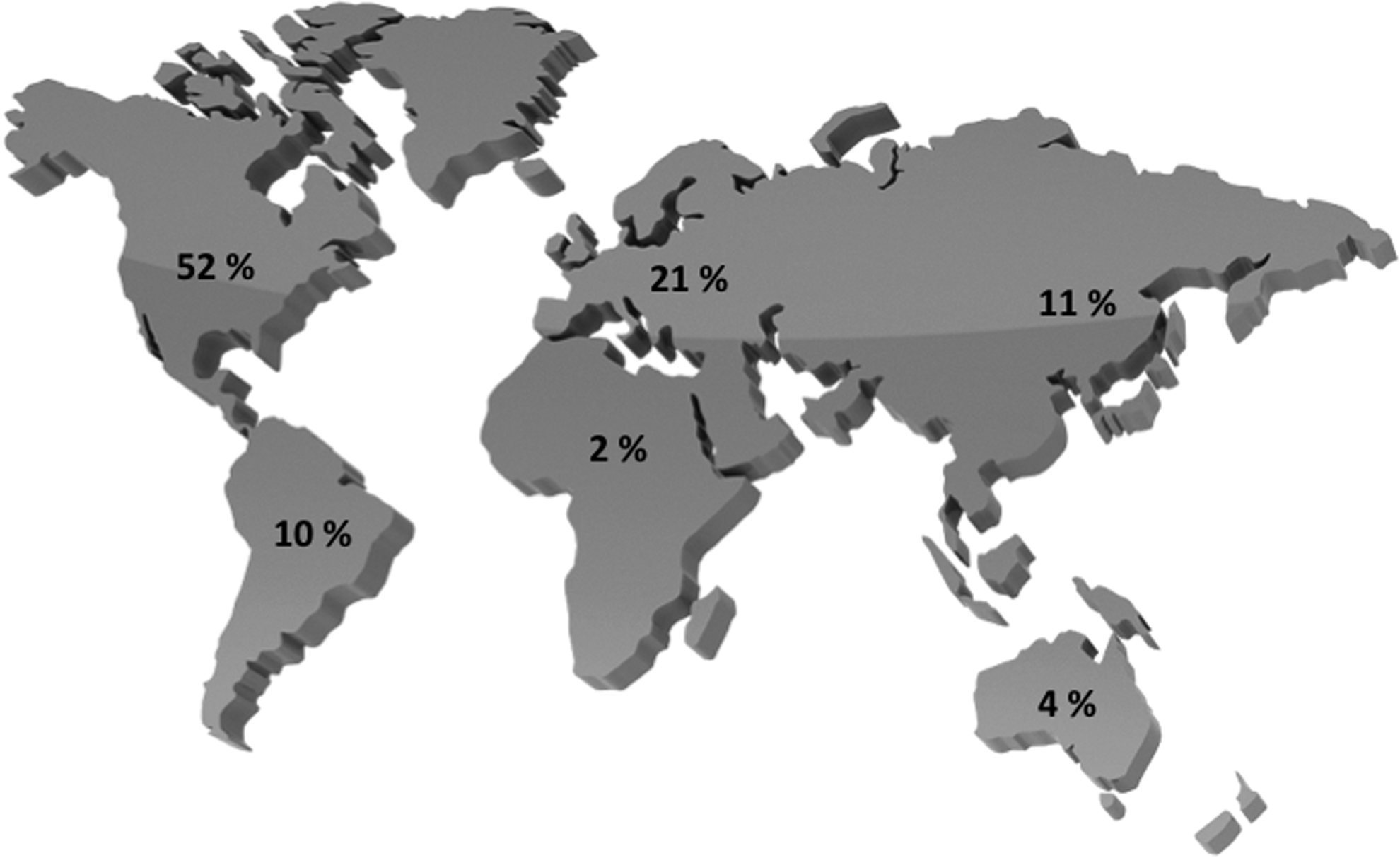
Global distribution of respondents by continent.
Operative management
The volume of EAs personally repaired per year was most frequently 1–3 cases (67%), followed by 4–7 cases (24%), and greater than 7 cases (8%). One-half of the respondents reported using the thoracoscopic approach. Of those, the volume of thoracoscopic cases was 1–3 (76%), 4–7 (17%) and 7 or more (7%). Currently the majority of surgeons (65%) learned the thoracoscopic technique after completing fellowship training.
One-third of the surgeons who used the thoracoscopic approach attempted all cases thoracoscopically without exclusion criteria. Of the remainder with exclusion criteria, small size, poor physiologic status, long gap length, and congenital heart disease were the most common reasons to start with an open approach. The weight cutoff ranged from 1.5 to 3.0 kg. Regardless of approach, preoperative bronchoscopy was routinely performed by 60%, selectively by 13%, and never in the remaining cases.
Thoracoscopic repair was almost uniformly performed via an intrapleural approach (96%), in contrast to the open repair, in which 89% perform the operation extrapleurally. The initial knot during thoracoscopic repair was secured intracorporeally by 71% of respondents compared with 29% who used an extracorporeally tied knot. Most surgeons used absorbable suture, with the most common sizes being 5-0 and 4-0. The data on suture type and size are outlined in Table 1. After completing the repair, regardless of approach, 30% attempted to put tissue between the esophagus and trachea, most commonly pleura followed by azygous vein. There were 12% who reported reinforcing the anastomosis with tissue sealant and 5% who placed synthetic material between esophagus and trachea. A chest tube was left by 83%, and a transansastomotic stent was left by 84%.
During excessive tension, 10% of respondents used spiral myotomies to reduce tension. In the face of a long gap, 32% would still attempt the repair thoracoscopically. If there was a long gap, 60% of respondents believed in progressive esophageal lengthening techniques. Of these, 62% used operative suture placement with tension to narrow the gap, whereas the remainder used gastric bolus feeds, natural growth, or dilators.
In dealing with strictures, 80% of respondent stated the surgeon handles the dilations, the gastroenterologist in 11%, the interventional radiologist in 8%, and the otolaryngologist in the remainder. Dilations would start as early as 2 weeks after repair, whereas 5% would wait until after 10 weeks. The interval from repair to dilation that surgeons reported is depicted in Figure 2. The preferred type of dilator used is currently the balloon dilator (74%). Most (77%) suggested no established maximum number of dilations before giving up on a stricture, whereas the others would try three dilations prior to operative management. Seventy-two percent would resect a stricture and redo the anastomosis if able, whereas the remainder would go straight to replacement with a recalcitrant stricture. Of those, 30% would initiate the redo operation thoracoscopically. Steroids or mitomycin was reported to be used on the stricture by 54 respondents, which were fairly evenly distributed with 57% mitomycin and 43% steroids.
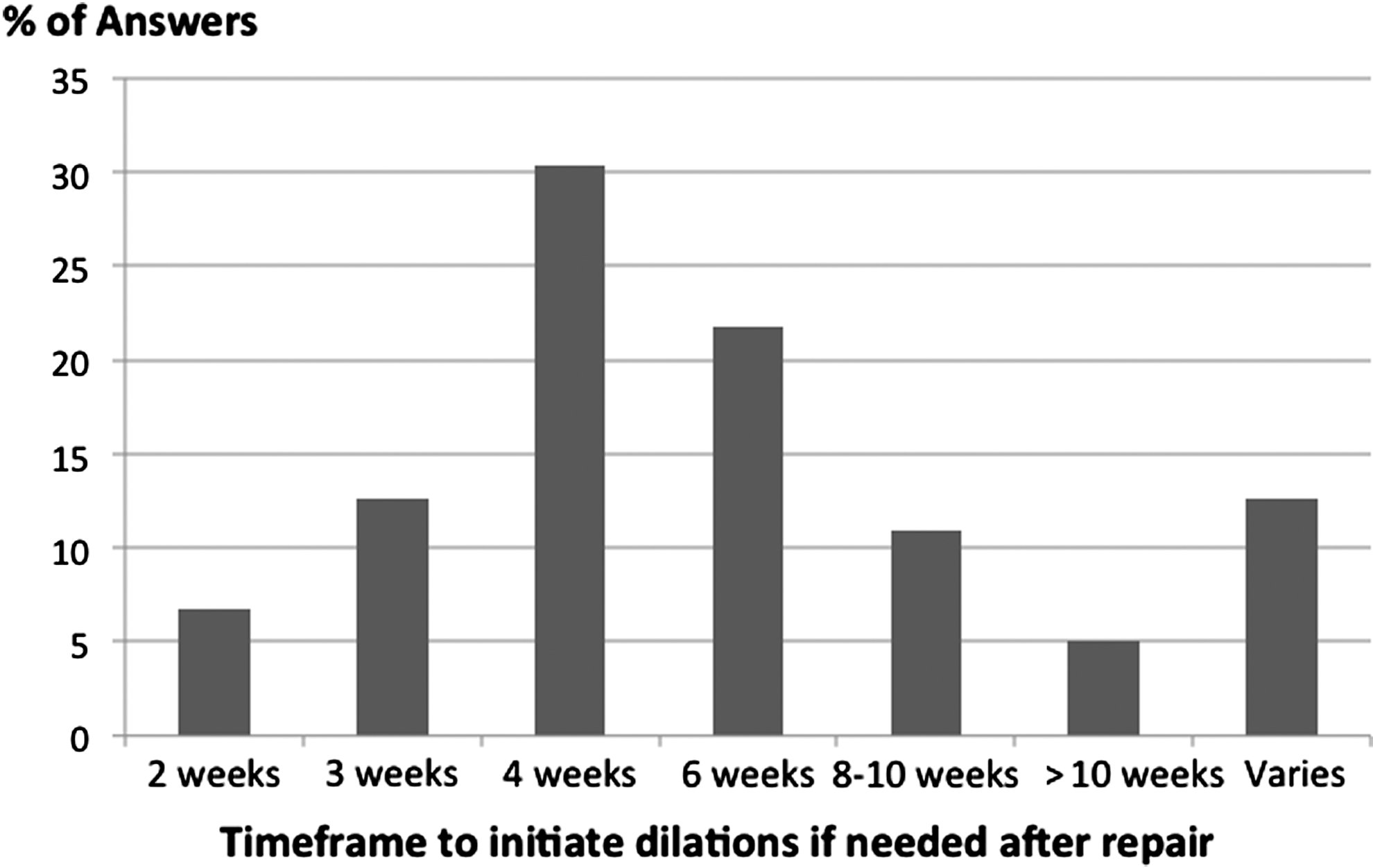
Distribution of answers by percentage of respondents on time from repair to initiate dilations.
A primary esophageal replacement would be considered by 40% for a very long gap. There were 128 (75%) who reported a preferred type of esophageal replacement, as outlined in Table 2.
Postoperative management
Patients are routinely left intubated/paralyzed by 25% for an interval of 0–4 days (76%), 5–7 days, (13%) and longer (11%). A normal esophagram was required by 85% to initiate oral feeding, with 93% of those performing the esophagram on postoperative Day 5–10. Of those who do not obtain an esophagram, feeds are started between Days 1 and 3 in 38% and Days 4 and 6 in 31%, with a range of 1–10 days. For those who obtain an esophagram postoperatively, 48% are done on Days 7–10, and 46% are done on Days 5–7, with the remaining 6% done prior to Day 5. If a leak is noticed, 11% repeat the study in 5–7 days, 78% in 7–10 days, and 9% at a longer interval. Sixty-six percent initiated transanastomotic feeds prior to obtaining an esophagram. Postoperative antibiotic use was common (76%) and varied from less than 1 day to greater than 14 days. Acid suppression medication was used by 76%, with a duration ranging from 7 days to lifelong.
Discussion
Worldwide, the prevalence of thoracoscopic repair of EA and EA/TEF is increasing, as evidenced by this study. Half of the respondents performed thoracoscopic repair routinely. This high percentage does not likely represent the prevalence of thoracoscopic repair for EA and EA/TEF within the general pediatric surgery community. Our data are biased by virtue of the survey targeting the IPEG membership, who have a keen interest in minimally invasive techniques and the disproportionate number of academic surgeons. Regardless, with the small number of cases (1–3) being completed by individual practitioners in any given year, there is a need for multi-institutional studies with large patient numbers to achieve data that can lead to best practices and reduction in healthcare costs.
This is the first study to examine the worldwide variability in surgical management of patients with EA and EA/TEF, and we discovered that practice variation is immense. Several of these findings should be topics for future investigation. For example, postoperative antibiotic use ranged from <1 to >14 days. Similarly, acid suppression treatment ranged from none to lifelong. These topics would be feasible and relatively simple to study, with high impact given the unintended sequela associated with antibiotics and long-term acid suppression. Determining the ideal postoperative feeding regimen would be important because it may limit duration of hospitalization, which has a tremendous impact on charges. Another variable that has a heavy influence on resource utilization is the use of paralysis and mechanical ventilation after the operation. Although this was historically favored, there appears to be little rationale currently, as 25% of respondents still used this strategy. The difference in outcomes-based approach, either open or thoracoscopic, would likewise be a very important contribution. IPEG members, who are technical experts with both approaches, are the group who should lead by conducting well-designed multicenter trials. Although there is large variability in suture size and material, this has been previously shown to be unlikely to have a substantial influence on outcomes.
Fortune 500 companies have long recognized that variability in process and performance are inversely related to quality of products. 7 The healthcare field has recently adopted this thinking and has sought to reduce variability in an effort to contain costs and improve quality.7–10 Variability in patient care is not unique to the surgical management of EA and EA/TEF. Landrigan et al. 10 reported substantial variation in the treatment of even the most common pediatric conditions by pediatric hospitalists. They found that variation was significantly higher in disease processes that did not have strong evidence-based therapies. In order to improve quality of care, minimize over- or underutilization of therapies, and decrease undesirable variation, the authors stress the importance of multicenter research efforts to establish evidence-based care guidelines. However, just the establishment of evidence-based practices may be insufficient in eliminating treatment variability. Conway and Keren 8 evaluated the variability in care of children with urinary tract infections treated at children's hospitals. They found that despite established evidence-based treatment guidelines, variability in care remained. The authors advocated the implementation of clinical practice guidelines and best practices with benchmarking to reduce such variability. Benchmarking can allow individual hospitals and practitioners to gauge their compliance with evidence-based guidelines and compare them with local, regional, and national hospitals and practitioners.7,11 This concept is the basis behind the American College of Surgeons' National Surgical Quality Improvement Program. The recently released National Surgical Quality Improvement Program Pediatric allows interinstitutional comparisons and benchmarking in an effort to decrease variability and improve care. 12
The first step in reducing variability in the care of patients with EA and EA/TEF would be to conduct prospective and randomized trials in order to define best practices. IPEG is a society that is well suited to organize and conduct these trials. With a large international membership, IPEG could accrue patients in meaningful numbers to answer these much-needed questions regarding the care of patients with EA and EA/TEF. Once best practices and clinical guidelines are defined, benchmarking could be used to ensure compliance with an ultimate goal of more efficient healthcare delivery, improved patient outcomes, and reduced healthcare costs.
Footnotes
Disclosure Statement
No competing financial interests exist.