
Abstract
Abstract
The definition accepted for the largely controversial and multiple criteria condition known as long-gap esophageal atresia (LGEA) is “inability to achieve primary end-to-end anastomosis,” particularly in the presence of a tracheo-esophageal fistula. In this article we report our technique of laparoscopic transhiatal esophagectomy and gastric pull-up (TEGPUL) in LGEA, based on the open approach of Spitz. Differences between TEGPUL and the original technique are the absence of a pyloromyotomy, the peel-away technique, the gastric pull-up through the distal esophagus, and its extracorporeal section. We performed the technique in 10 patients: 6 girls and 4 boys. Six had esophageal atresia type III (60%), three had esophageal atresia type I (30%) and one had esophageal atresia type II (10%). Mean time in surgery was 4.43 hours (range, 3.3–7 hours). Average stay in the pediatric intensive care unit was 5.9 days (range, 3–25 days). Average time under mechanical ventilation was 4.6 days (range, 2–8 days). Average total hospital stay was 19.4 days (range, 11–40 days). Oral feeding began at 15.6 days (range, 5–30 days). We believe these steps and the early realization of the technique will reduce the morbidity and mortality among these patients and decrease the number of contraindications to gastric pull-up. Nevertheless, a valid conclusion will require more studies with a larger number of patients and longer follow-up.
Introduction
The definition finally accepted for the largely controversial and multiple criteria condition known as long-gap EA (LGEA) is “impossibility to achieve primary end-to-end anastomosis,” particularly in the presence of a tracheo-esophageal fistula.2,7 However, we believe that achieving or not the primary anastomosis also depends on the surgeon's experience and skills. Therefore, we define LGEA as congenital (those where anastomosis is obviously impossible) or acquired (those where a primary anastomosis is initially achieved and then lost because of complications requiring a very high number of second surgeries, among them an esophagostomy and/or gastrostomy).
In the recent past and for multiple reasons, we have seen a larger number of acquired LGEAs in our country. As a consequence there has been an increase in the number of patients requiring surgery for esophageal replacement. Although the ideal surgical procedure to bridge LGEA remains unsolved 8 and satisfactory results have been reported with all techniques, the one that is the most safest and more anatomic and with fewest long-term complications, at our discretion, is the gastric pull-up (GPU); nonetheless, more follow-up studies are required.7,9,10
GPU was first described in 1922, and yet in 1998 it was contraindicated in patients with extensive scarring from previous surgery or mediastinal inflammation. 11 Reports of laparoscopic GPU only appeared in the 21st century with the first case reported in 2003, even though—at the time—60% of pediatric surgeries in specialized centers were laparoscopic-assisted. 10
In this article we report our technique of laparoscopic transhiatal esophagectomy and GPU (TEGPUL) in LGEA, based on the open approach of Spitz.
Patients and Methods
In the last 2 years, we have used the TEGPUL procedure in 10 LGEA patients at the Hospital de Clínicas Caracas, Caracas, Venezuela. The presence of EA, types I, II, and III, indicated the need for surgery.
Technique
The TEGPUL was done in 9 cases by a single surgeon and in 10 cases, with the same surgical team, with the patient under balanced general anesthesia and in the supine position. The patient's body was placed over a support, placing a leveler under the chest to keep it higher than the abdomen and thus permitting easy entry of instruments into the mediastinum. With the Hasson technique, a 5-mm umbilical trocar was placed to permit introduction of the camera and production of a 10–12 mm Hg pneumoperitoneum. A 12-mm trocar was placed in the left iliac fossa, and a 5-mm trocar was placed in the right iliac fossa. A Nathanson separator was introduced at the epigastrium level to separate the liver, placing a 3-mm trocar at the gastrostomy incision to retract the stomach. With the LigaSure™ bipolar clamp device (Covidien, Mansfield, MA) and 45-mm Echelon® blue cartridges (Ethicon EndoSurgery, Cincinnati, OH), the gastrostomy was detached from the abdominal wall. Then, the stomach was moved using the same cauterizing instrument, starting with the gastrohepatic ligament and the lesser curvature, and cutting the left gastric vessels. Dissection of the esophagus began through the hiatus, separating it from all adjacent structures of the mediastinum. Once transfer of the esophagus into the abdomen was achieved, a procedure to partially release the greater curvature was begun, cutting the first short vessels, mostly those in contact with the spleen, while preserving the gastroepiploic arcade.
The mediastinum was dissected with particular care to avoid pleural punctures or injuries to the pericardium and/or the pulmonary artery trunk, among others, and always advancing above the aorta.
Dissection of a cervical esophagostomy or a proximal esophagus (in cases without esophagostomy) through a cervicotomy
Digital communication, under direct vision, between the neck and the mediastinum was achieved. A Foley bag was placed from the neck to the abdomen, to permit dilation of the cervical–mediastinal tract followed by use of our peel-away technique. The tract was dilated with Hegar bougies up to 18 or 20 in number, depending on the patient's age. A 12-mm cervical–mediastinal trocar was placed inside the above-mentioned Foley bag, followed by the peel-away technique (Fig. 1), which consists of breaking the bag with a technique similar to that used for the placement of central venous catheters, opening it in half and taking it out gradually without permitting an exit of the trocar. Doing it this way, we avoid the formation of false cervical–mediastinal tracts, and a gradual dilation of the tract that permits the GPU to be done through the specially prepared space.
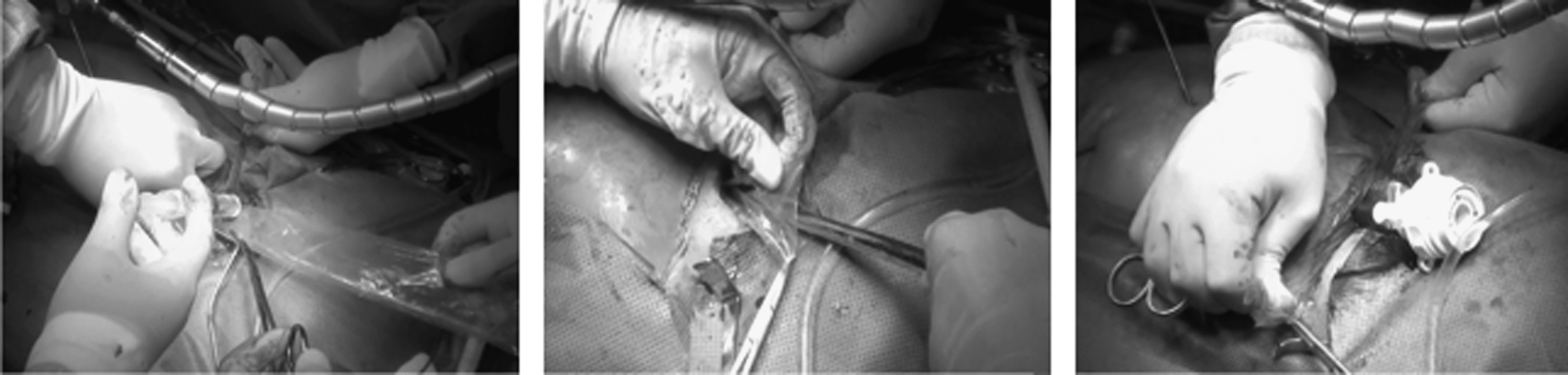
Steps of the peel-away technique.
Then a forceps was introduced through the cervical–mediastinal trocar to pull-up the esophagus and stomach while checking laparoscopically the appropriate orientation of both. Once the distal esophagus was completely outside the neck, we exteriorized the gastric fundus, until it can be seen through the cervicotomy, without returning to the chest. Extracorporeal section of the distal esophagus was achieved with a linear cutting machine and a 45-mm blue cartridge (Fig. 2), followed by the esophagus fundus anastomosis in a plane with 4-0 Vicryl™ (Ethicon). Appropriate location of the stomach in its entry to the mediastinum through the hiatus was verified. No stitches were placed between the hiatus and the gastric antrum. Extramucosal pyloromyotomy with electrocautery was done in only 3 cases. In some cases, a Dobhoff nasojejunal tube was placed under laparoscopy, and in others a jejunostomy with location of the second jejunal loop was done; both procedures are for early enteral nutrition (Fig. 3). If there was no pleural injury and/or evidence of pneumothorax, no chest drain was left in place. In all cases, a latex drain was left on the level with the cervicotomy. A nasogastric tube that reached the GPU site was placed for the purposes of decompression.

Extracorporeal esophagectomy.
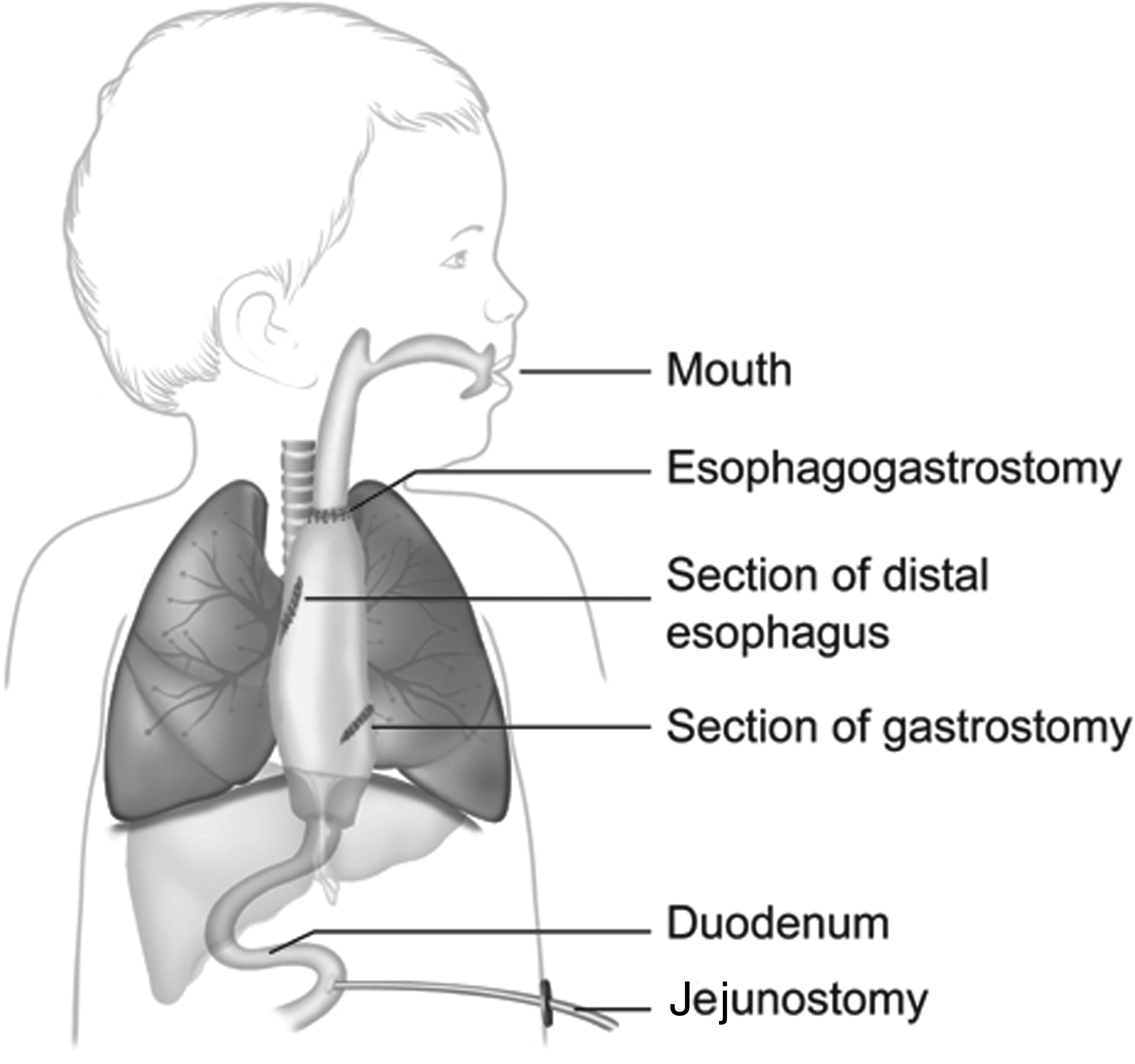
Transhiatal esophagectomy and gastric pull-up.
Patients were taken to the pediatric intensive care unit, where they remained with mechanical ventilation about 48 hours. Enteral nutrition was started via the nasojejunal tube or a jejunostomy at 24 hours postoperatively, if patients were in stable conditions. Upon their discharge from the pediatric intensive care unit, they were treated as long as necessary in the hospitalization area. Evaluation in outpatient clinics, by the same surgeon and regularly, establishes a long-term follow-up, which would be useful in a later publication of results.
Results
The patients were six girls and four boys, with a mean age of 52 months (range, 8–96 months). Six had EA type III (60%), three had EA type I (30%), and one had EA type II (10%). Results are summarized in Table 1. In all cases TEGPUL was laparoscopic, and no one required a change of procedure. Mean time in surgery was 4.43 hours (range, 3.3–7 hours). Eight patients had left esophagostomy. One of the remaining two patients, the EA type II carrier, had been subjected, a week before, to an esophagoesophagostomy via thoracoscopy, at which time the proximal fistula was detected and ligated; therefore exteriorization of the proximal esophagus during the TEGPUL procedure was not complicated. In the other one, an EA type III carrier, the proximal esophagus was firmly attached to the mediastinum, and there was evidence of non-reabsorbable sutures throughout (Fig. 4). It is noteworthy that both patients were treated at home without esophagostomies: 1 through the use of an oroesophageal tube for gravity drainage and the other by voluntarily spitting saliva. 12 Extramucosal pyloromyotomy was only done for the first 3 patients. A nasojejunal feeding tube was placed in 5 patients, and 5 patients had a jejunostomy. Average stay in the pediatric intensive care unit was 5.9 days (range, 3–25 days). Average time under mechanical ventilation was 4.6 days (range, 2–8 days). Average total hospital stay was 19.4 days (range, 11–40 days). Only 1 patient died, 12 days postoperatively, after being discharged from the pediatric intensive care unit; death was caused by cardiorespiratory failure that did not respond to cardiopulmonary resuscitation measures, even though the patient had no cardiopathy. On average, oral feeding began after 15.6 days (range, 5–30 days). Four patients had leaks in their esophagus–fundus anastomosis that healed spontaneously in an average of 18 days (range, 9–26 days). No surgery was required, just nothing by mouth, with enteral nutrition and oral suction of saliva.
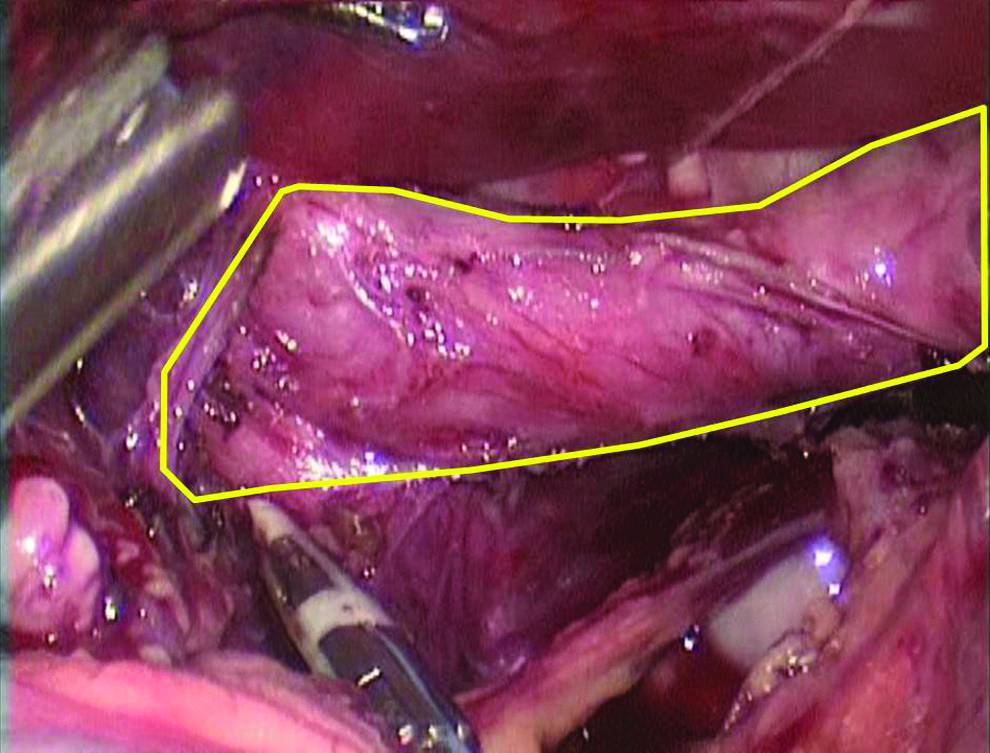
Distal esophagus (outlined).
EA, esophageal atresia; F, female; HPS, hypertophic pyloric stenosis; IBP, inflammatory bronchial pathology; m, month; M, male; PICU, pediatric intensive care unit; RTA, renal tubular acidosis; VACTERL syndrome, vertebrae (V), anus (A), cardiovascular tree (C), trachea (T), esophagus (E), renal system (R), and limb buds (L) syndrome abnormalities; y, year(s).
Early complications (first 7 days) are described in Table 2.
Was the only patient operated on by another surgeon.
Feeding of all living children is achieved orally without the need for tubes. The surviving babies are gradually gaining weight, and their parents are satisfied with the surgery results.
Discussion
Several published trials have shown a trend favoring GPU as the technique of choice for esophageal replacements. In fact, 94% of the surgeons involved in those procedures in children are satisfied with the results obtained with the technique. 7 Even though for years preservation of the native esophagus has been considered the best option, such preservation is not always possible at a reasonable cost. 7
Our patients, as is the case in reports of many series, 9 come to our center from other cities where they probably have undergone previous surgeries (cases 1–5), surgeries that were not only aimed at preserving their native esophagus, but rather intended to control the closure leaks of a tracheo-esophageal fistula or the closure of the distal and/or proximal esophagus.
None of the patients in our series had been treated by our team in their neonatal stages. 13 What came to our attention while doing the TEGPUL, a technique that we had previously discussed and jointly chosen with the parents on the basis of cost-benefit considerations, is that we did not find in any of the patients a purely intraabdominal esophagus and that the greatest length of a distal esophagus was 6 cm (Fig. 4). Sixty percent of the EAs were type III.
Maksoud-Filho et al. 14 pointed out that in 75% of delay-repair cases, primary resolution of the LGEA is delayed for a 12-week period, and the child's weight increases twofold; this esophagoesophagostomy is both possible and successful. 2 This opinion is sustained by the study of those patients who do not undergo an esophagostomy, even though the growth possibility of the esophagus is around 30%—based on a measurement of the esophageal ends using two endoscopes in order to come as close as possible to the distance that would be obtained with a careful surgical dissection. 6 However, in our series only 2 patients did not have an esophagostomy. In the first one (EA type II), when the esophageal ends were measured with only one endoscope, the distance measured was three vertebral bodies. In spite of this, we attempted a primary anastomosis that failed because of a severe leak that was detected 1 week after the thoracoscopy. In the case of the second patient (type III EA), the distance was greater than three vertebral bodies. In view of this we performed a TEGPUL without any problems in both cases. 14 Nevertheless, along with other authors, we believe that there is no adequate method for measuring the esophageal ends that takes into account the distance between both ends as related to age, weight, and the technique used. 14 On account of this, we suggest the algorithm for managing EA that is illustrated in Figure 5.
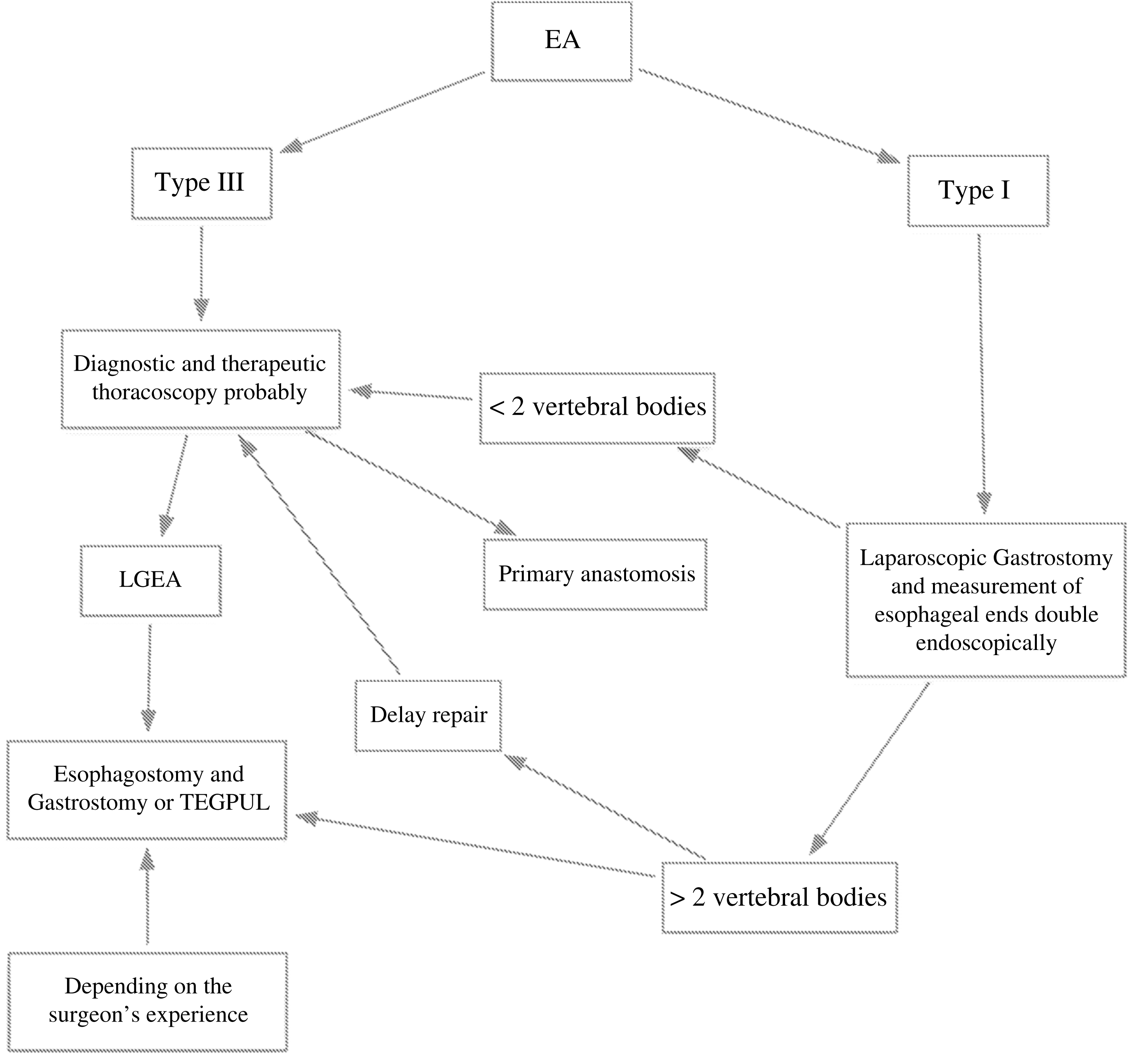
Algorithm for managing esophageal atresia (EA). LGEA, long-gap EA; TEGPUL, transhiatal esophagectomy and gastric pull-up.
The old blind approach to the posterior mediastinum—described in 1984 and 1995 by Spitz 11 in the open surgery GPU—is no longer necessary when the procedure is done with laparoscopic surgery, in which dissection is carried out under direct view of the posterior mediastinum. 9 Some trials report that such digitally made cervical mediastinal dissection is inadequate because it is blind. However, in the case of our adapted Spitz technique, which is based on a laparoscopic approach, we are able to view almost 95% of that area's dissection. As a result of this, we believe that we reduce both the risks and the lesions that the area could suffer. Besides, we also use our peel-away technique for this purpose (Fig. 1).13,15,16
From the early days of laparoscopic GPU, back in 2003, the Spitz technique has been performed—unlike the TEGPUL technique—following these steps: intracorporeal section of the distal esophagus, pull-up of the stomach through the fundus, and a pyloromyotomy.10,13
In our case, we instead perform an extracorporeal section of the distal esophagus in order to use it for the pull-up, thus protecting the fundus from any possible damage. We believe that when other methods are used for the GPU, the risk of rupture of the fundus is greater. There is also a greater risk of ischemia and of multiple failures when attempting the pull-up due to the weight of the stomach and because the tissue where the anastomosis will be performed is at risk.
As is the case for other authors, we do not regularly perform pyloromyotomies in our patients. 17 We believe it is not necessary in every case based on the results of postoperative endoscopic controls in areas where we thought a pyloromyotomy had been performed; such results showed that even though the area dissected did not correspond to the pylorus, the patients had a satisfactory evolution. On account of those findings, we did not perform pyloromyotomies in the final 7 patients, but all evidenced a similar evolution. Some trials have reported that despite the pyloromyotomy 8 performed in GPU patients, there is a delay in gastric emptying; other trials have reported that there is no significant difference between the types of pyloric procedures performed and gastric emptying in patients who have had a GPU. 18
Ever since the first case of a laparoscopic GPU was reported, the need for performing a pyloroplasty in these patients has been questioned. 10 There is a need for reports on a greater number of cases without pyloroplasty in order to study the evolution of such patients. In our cases, supported by evidence-based medicine, it would seem that pyloroplasty is not necessary because it seems to prevent at any rate gastroduodenal reflux, which could be more harmful than gastroesophageal reflux.
Spitz 15 described the open GPU with a jejunostomy as a feeding route in those patients without an esophagostomy who have not been trained in oral feeding techniques. We decided to use a nasojejunal feeding tube in our first 5 cases (50%), to avoid the morbidity of a jejunostomy, 15 a decision that could not be sustained because the high costs for reinserting the feeding tube when it was accidentally dislodged, hindering enteral feeding at different stages of the postoperative period. We currently believe that in well-selected cases, the nasojejunal feeding tube can be an appropriate enteral feeding route, mostly after the surgeon has completed the learning curve. For the remaining 50% (5/10) we did a jejunostomy, and the subsequent morbidity was similar to that reported in the literature. 15
Our causes of death are more or less similar to the most frequent causes reported by Spitz et al., 9 namely, respiratory failures and prior surgeries. The same occurs with the esophagus–fundus anastomosis leaks: we have four (40%), which would not be comparable to the 12% reported by Spitz et al. 9 Coincidentally, the patients who had a leak were those who were under sedation for a shorter period of time (<4 days) and who were older than 1 year of age. Nevertheless, we still believe that early esophageal replacement would decrease many of such complications.9,13
The pulmonary condition of patients in pre- and postsurgery is essential for the management and follow-up of LGEA patients—with or without a fistula—regardless of the scarcity of reports in the literature.6,10
Conclusions
In their large series, Spitz et al. 9 have reported that GPU is one of the best options for esophageal replacement; consequently laparoscopic GPU should have a similar or even better evolution on a long-term basis.3,9
This study also ratifies that laparoscopic GPU is a reliable and easy procedure, 7 as described by Spitz et al., 9 when the surgeon is skilled in advanced pediatric laparoscopic surgery. 10
Differences between TEGPUL and the original Spitz technique are the absence of a pyloromyotomy, the already-mentioned peel-away technique, the GPU through the distal esophagus, and its extracorporeal section. We believe these steps and the early realization of the technique reduce the morbidity and mortality in these patients and decrease the number of contraindications for GPU. Nevertheless, a valid conclusion will require more studies with a larger number of patients and a longer follow-up.
Footnotes
Disclosure Statement
No competing financial interests exist.