
Abstract
Abstract
Objectives:
To analyze the outcomes with mid- to long-term follow-up of laparoscopic ureterolysis (LU) and omental wrapping in retroperitoneal fibrosis (RPF) with obstructive uropathy.
Patients and Methods:
Records of 9 patients with RPF who had obstructive uropathy at presentation and had undergone LU and omental wrapping at our center during January 2004 to June 2012 were collected and analyzed.
Results:
Six females and three males underwent LU for RPF. Underlying causes of RPF could not be found in 8 (89%) cases. Two patients underwent bilateral LU. Mean operative time and estimated blood loss were 213 minutes (range, 180–280 minutes) and 119 mL (range, 70–200 mL), respectively. No case required conversion to open surgery. The only significant intraoperative complication (1/9 [11%]) was ureteral injury, which was easily repaired intraoperatively. The postoperative complication rate was 44% (4/9). Most complications (75% [3/4]) were minor and did not need specific treatment. The mean follow-up period was 46 months (range, 4–72 months). The success rate at last follow-up was 89%.
Conclusions:
Treatment of RPF is still controversial. Any future prospective randomized comparative trials seem unlikely in view of the low incidence of RPF. LU and omental wrapping in the setting of obstructive uropathy are safe and an effective alternative with a high success rate at mid- to long-term follow-up.
Introduction
R
Because of paucity of the cases, no standard treatment has been established.1,7,8 Surgical ureterolysis has been considered the definitive treatment for ureteral obstruction in RPF.2,9,10 This has been classically performed by the open approach, which has a high success rate (90%).2,11,12 However, the open approach has complications like ileus, wound infection, chylous ascites, urinary leaks, and intestinal obstruction.11,13 Laparoscopic ureterolysis (LU) and intraperitonealization of ureters with or without omental wrapping have been used to reduce significant morbidity related to the open approach. So far, no prospective study has reported on the treatment outcomes specifically in patients having RPF with obstructive uropathy. Herein, we present our single-center, single-surgeon's 8 years of experience of LU and omental wrapping to treat obstructive uropathy due to RPF.
Patients and Methods
We retrospectively analyzed the records of patients who underwent LU for newly diagnosed RPF at our center during the period of February 2004–June 2012. Records of all patients who presented with ureteral obstruction (either bilateral or unilateral in the case of a unilateral functioning kidney) and obstructive uropathy (raised serum creatinine level) and were subjected to LU were included in the analysis. Patients without obstructive uropathy, already taking medical therapy, those with RPF secondary to malignancy, and those who underwent open ureterolysis were excluded from the study. Six females and 3 males fulfilled the inclusion criteria. Workup included magnetic resonance urography or computerized tomography scan, radionuclide scan, and retrograde pyelography. With the working diagnosis of RPF with obstructive uropathy, ureteral obstruction was relieved preoperatively (double-J stent or percutaneous nephrostomy [PCN]) in all patients. After baseline nadir serum creatinine levels were attained, all patients underwent LU and omental wrapping as definitive treatment. Postoperatively, medical therapy comprising prednisone (0.75 mg/kg/day for 3 months, 0.5 mg/kg/day for the next 3 months, followed by 0.25 mg/kg/day for the next 6 months) and tamoxifen (10 mg/day) was started at the time of discharge. In the case of tubercular RPF, antitubercular therapy and prednisone were given.
All patients were followed up every month for the first 3 months, after every 3 months until 1 year, and then every 6 months. Clinical examination and serum creatinine were obtained at each visit. Ultrasonography was done every 3 months for the first year and thereafter every 6 months. Imaging (computerized tomography scan, magnetic resonance urography, or radionuclide scan) was done every 6 months or earlier, if indicated. We analyzed demographic and clinical data including preoperative and postoperative serum creatinine levels, preoperative intervention, intraoperative findings, operative time, estimated blood loss, complications, duration of hospital stay, and serum creatinine at the time of last follow-up. Success was defined as absence of symptoms, stent-free status, improved or stable preoperative nadir serum creatinine levels, and radiologically documented relief of ureteral obstruction.
Technique
In patients with a PCN tube in situ (i.e., those who could not be stented preoperatively because of tight narrowing of the ureter), RGP was performed just before the start of LU. Surgery was then performed. On completion of LU, a double-J stent was inserted. This was possible in all such cases. Patients with a double-J stent already in situ straightaway underwent surgery, and the same stent was kept after completion of LU.
LU was done by the transperitoneal approach in the 45° flank position in all cases. First, a 12-mm port (camera port) was placed by the open technique at the level of the umbilicus about two fingers width toward the side to be operated on. The peritoneal cavity was inspected with a 30° telescope followed by placement of two other ports: a 10-mm port in the midclavicular line in the iliac fossa (on the side to be operated on) and a 5-mm port between the xiphoid and the umbilicus (Fig. 1). In cases of bilateral ureteral obstruction (2 cases), the 12-mm and 5-mm ports were common for both sides; only the 10-mm port was inserted separately on both sides.
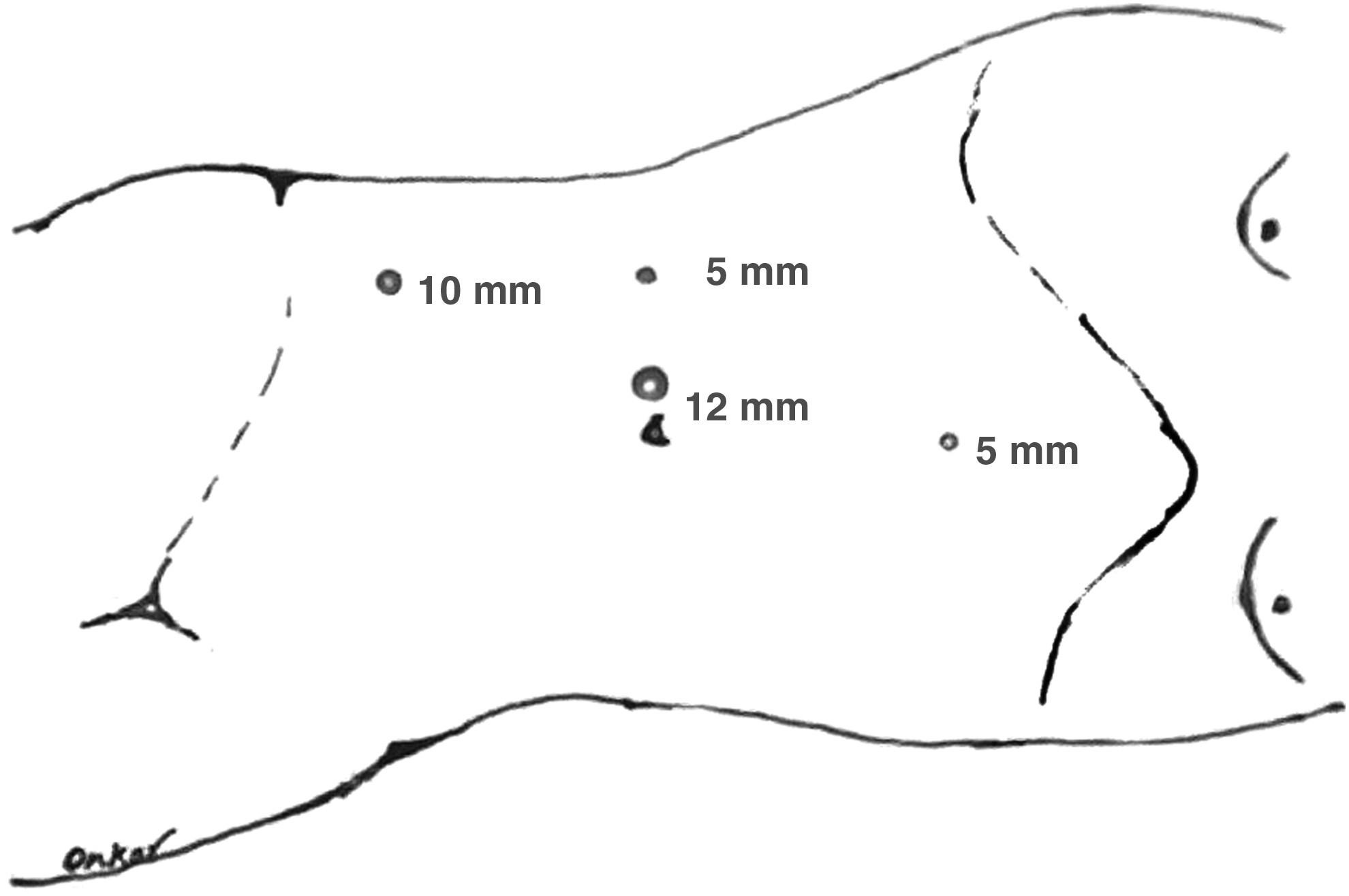
Port placement for right-sided laparoscopic ureterolysis with the patient in the 45° flank position.
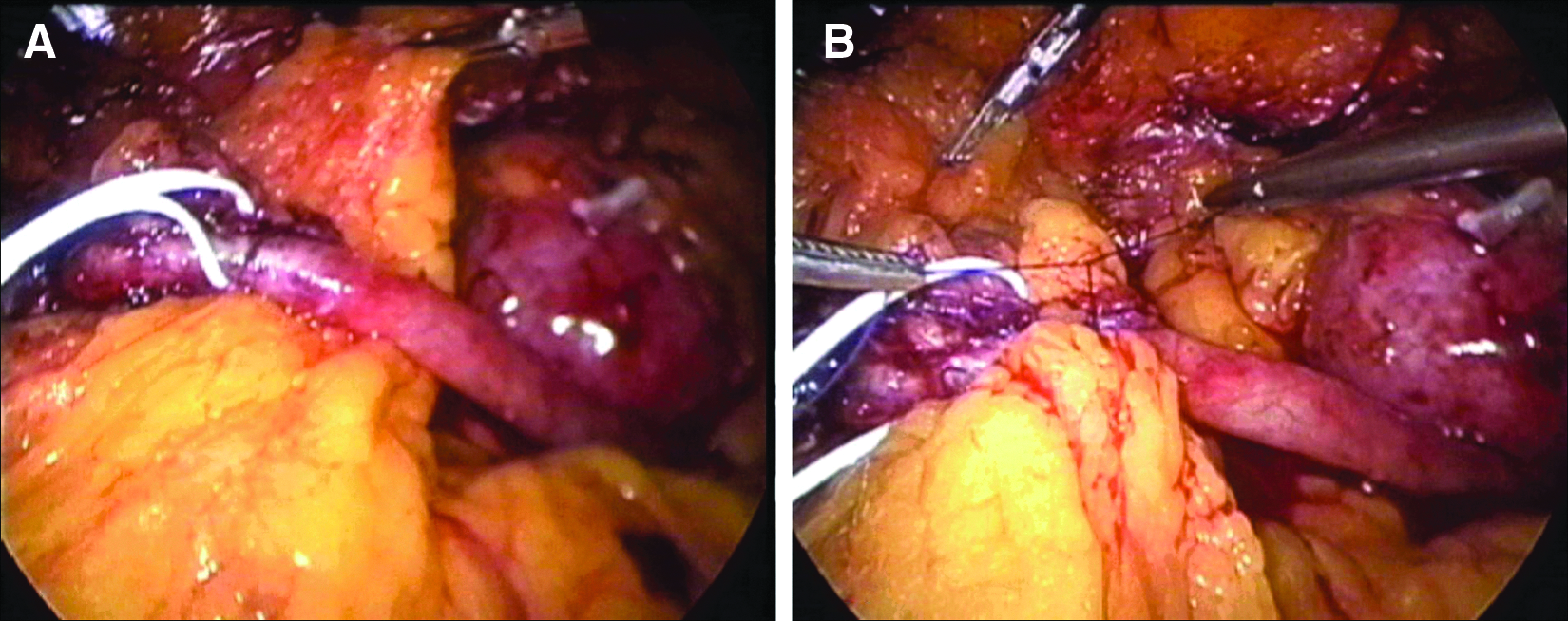
As severe fibrotic encasement makes identification of the ureter difficult, the ureter was identified in its proximal and distal segment, which was relatively less encased by fibrotic plaque. Distally, the ureter was identified at the level of its crossing over the iliac vessels. Proximally, the right ureter was identified on the right lateral border of the inferior vena cava and medial to the lower pole of the right kidney, and the left ureter was identified near the left gonadal vein and medial to the lower pole of the left kidney. Vascular loops were then passed around the proximal and distal unencased ureteral segments. An additional 5-mm port was inserted in the anterior axillary line at the level of the umbilicus, and using vascular loops as slings the ureter was lifted proximally and distally by the assistant. This provided countertraction for gentle blunt and sharp dissection to easily free the ureter completely. We took multiple biopsy specimens from the fibrous tissue. If the ureter was accidentally opened, it was closed using polyglactin 910 (Vicryl™; Ethicon, Somerville, NJ) 4-0 sutures. Finally, the omentum was wrapped around the whole of the dissected segment of the ureter and fixed with Vicryl 4-0 sutures, taking two or three bites (Fig. 2). We did not make or prepare the omental wrap. A portion of the omentum that could be easily pulled and wrapped circumferentially around the involved abdominal segment of the ureter was used. For bilateral cases, the patient was turned to the opposite side for surgery.
Results
The data regarding demographic characteristics, clinical parameters, preoperative intervention, intraoperative findings, complications, and follow-up are shown in Table 1. The patients included 6 females and 3 males. Mean age was 43.5 years (range, 35–57 years), and mean body mass index was 27.5 kg/m2 (range, 20–37 kg/m2). Mean serum creatinine level at presentation was 4.1 mg/dL (range, 2.3–5.4 mg/dL). Mean nadir serum creatinine level before LU was 1.6 mg/dL (range, 1.1–2.0 mg/dL). The most frequent clinical presentation was flank pain with uremic symptoms. One patient presented with anuria for the last 24 hours (Case 7, with primary tubercular RPF). A possible etiology of RPF could be identified only in 1 (11%) case (Table 1).
ATT, antitubercular therapy; B/L, bilateral; DJ, double-J; DVT, deep venous thrombosis; LU, laparoscopic ureterolysis; Lt, left; NFK, nonfunctioning kidney; PCN, percutaneous nephrostomy; RPF, retroperitoneal fibrosis; Rt, right; U/L, unilateral.
Preoperative intervention was in the form of either PCN in 5 cases or double-J stenting in 6 cases. In total, all 11 cases (9 patients) underwent LU and omental wrapping (Table 1). None of the cases required conversion to open surgery. Mean operative time was 198 minutes (range, 180–280 minutes) for unilateral and 275 minutes (range, 270–280 minutes) for bilateral LU. Estimated blood loss was about 119 mL (range, 70–200 mL). The longer duration of operation in bilateral cases was mainly attributed to the dissection part of the procedure. The classical finding of a grayish-white fibrous tissue plaque encasing the abdominal ureter that showed fibroblast proliferation, lymphocytes, plasma cells, and macrophages on histopathologic examination was present in all except 1 case (Case 7, with primary tubercular RPF).
The only significant intraoperative complication (1/9 [11%]) was ureteric injury that occurred during a difficult ureteric dissection in 1 case of tubercular RPF. The ureteral tear was repaired using fine interrupted sutures. Minor bleeding during surgery occurred in 2 cases from multiple small vessels around the perifibrotic tissue in 1 case and from small vessels around renal hilum in another case. Bleeding was successfully controlled in both cases by packing and application of vascular clips, bipolar cautery, and Surgicel® (Ethicon). Postoperatively, deep venous thrombosis developed in 1 case and prolonged the hospital stay. Other minor postoperative complications that were managed without need of any specific therapy included prolonged drainage from operative area (2 cases) and prolonged ileus (1 case). Oral feeding was started 24–36 hours after the procedure. The mean duration of hospital stay was 5 days (range, 3–12 days). The rest of the details of patients in our series are summarized in Table 1.
Mean follow-up was 46 months (range, 4–72 months). Mean postoperative timing of removal of stents was 6 weeks (range, 4–8 weeks). At last follow-up, 8 of the 9 patients were symptom-free, had improved or stable preoperative nadir serum creatinine levels without stents, and had radiologically documented relief of ureteral obstruction (success rate, 89%). None of the patients experienced drug treatment-related toxic effects requiring stopping of drugs. One patient in whom ureteral obstruction recurred after 4 months of LU is being managed with stenting and drugs.
Discussion
RPF is an uncommon but severe disease that may result in obstructive uropathy and renal loss. Prompt diagnosis and appropriate treatment may prevent such urologic complications. Despite the possibility of severe renal functional damage, there is no standardized treatment of RPF. Medical management (with or without stents) consisting of corticosteroids, 14 azathioprine, cyclophosphamide, 15 and tamoxifen 16 has been used, but optimum doses and duration of drugs are not well established. 14 Open ureterolysis or LU with or without adjuvant corticosteroids has also been reported with good outcomes.8,17–27 However, there have been no prospective randomized trials comparing different approaches.
Because of varied symptoms of RPF, patients are often first seen by medical specialities and later referred to the urology department. 28 Ureteral involvement with hydronephrosis occurs in 80%–100% cases, and in about one-fourth to three-fourths of patients at least one kidney is irreversibly damaged.1,6,28 However, the exact incidence of obstructive uropathy due to RPF is not clear in the literature, 28 and no prospective study so far has reported on treatment outcomes (medical/surgical), particularly in patients of RPF with obstructive uropathy. In our series 7 of the 9 patients (77.7%) lost the use of one kidney, another 2 had bilateral ureteral obstruction, and all had obstructive uropathy at presentation (Table 1). Furthermore, in spite of evolving obstructive uropathy in RPF, renal function may initially remain normal for a long period, and symptoms are vague, making early diagnosis difficult. Thus, diagnosis is usually delayed until ureteral obstruction and/or obstructive uropathy ensues. 6 In other words, the presence of obstructive uropathy with loss of one kidney probably indicates advanced disease. Corticosteroids are usually effective in the early stage of RPF (but may not work in all cases); later stages are less likely to be responsive to medical treatment. 29
In RPF with obstructive uropathy there are two options for treatment: first, relief of obstruction by stents or PCN followed by drugs (corticosteroid alone or with azathioprine, mycophenolate mofetil, or tamoxifen); and second, relief of obstruction by surgical ureterolysis with or without adjuvant corticosteroid therapy.1,6,17,30–32 Both options have been tried with almost comparable results. Considering the first option, neither the type, dose, and duration of drugs nor the duration of urinary drainage (stents or PCN) is clear.32,33 Recently, Fry et al. 33 reported successful treatment of 24 patients with prednisone and stents only. Twenty-three of the 24 patients had obstructive uropathy at presentation, but only 7 (29%) had a solitary functioning kidney. Average stent duration was 13.7 months (range, 2–50 months), and steroid therapy was administered for a mean period of 34 months. Success rate in their series was 75%. In another series, Ilie et al. 32 treated 28 patients (25 had obstructive uropathy) with stent(s) or PCN with or without steroids. The mean stent duration was 19.34 months (range, 2–60 months). Although these authors reported a success rate of 86% at last follow-up, their criteria of successful treatment were symptom-free status and stable serum creatinine level only. After a mean follow-up of 60.9 months (range, 24–110 months), 5 patients were still on stents and steroids, and 8 additional patients were on stents without steroids. Thus, 15 (54%) patients were stent free and off steroids. These data indicate that the efficacy of medical management (with urinary drainage) in patients of RPF with obstructive uropathy is not well documented and that the durations for which stent(s) or PCN are required are usually longer (2–60 months).14,30–33 In RPF patients who are already in obstructive uropathy (many with a solitary functioning kidney), longer durations of stents or PCN along with steroids may place them at more risk of complications related to stents or PCN.34–36 In view of the above data we proceeded with initial LU in our patients of RPF with obstructive uropathy. However, we do institute adjuvant medical management (prednisone and tamoxifen) in order to further reduce the recurrence risk and to relieve systemic manifestations of RPF that are not tackled by surgery. In our patients mean stent duration was only 6 weeks post-LU, and 89% (8/9) patients were stent free and off drugs. In a similar series reported recently, Sinescu et al. 37 reported results for 19 patients with RPF (17 had obstructive uropathy) treated by ureterolysis and omental wrapping without adjuvant steroids. Stent duration was 1 month. After at least 1 year of follow-up 17 of 19 patients were stent free, and 15 of the 17 patients with obstructive uropathy (88%) had normal serum creatinine levels.
Ureterolysis (open or laparoscopic) has been reported to have a success rate as high as 100%.8,12,18,25,26 The open approach for ureterolysis has approximately 9% mortality and 60% morbidity. 18 In an attempt to reduce procedure-related morbidity Kavoussi et al. 19 first described LU in 1992. Since then LU has been used by several investigators (with some modifications) only to demonstrate common advantages of minimal invasiveness of laparoscopy and comparable efficacy to the open approach.18,20–27 Elashry et al. 18 compared the results of six LU procedures with seven open ureterolyses (all unilateral cases) and found the laparoscopic approach to be better in all aspects they considered except mean operative time (255 minutes for laparoscopic versus 232 minutes for the open approach). Our mean operative time for 7 unilateral LU cases was 196 minutes. In a large series of 70 cases of RPF (idiopathic and secondary) comparing LU (36 cases) with the open approach (34 cases), no difference was found in terms of operative time, estimated blood loss, length of hospital stay, complications, transfusion requirements, and postoperative resolution of ureteral obstruction. But, for idiopathic RPF cases treated by LU, hospital stay and transfusion requirement were significantly less than for patients who underwent open ureterolysis. 25 The reported success rate of LU is 83%–100% at 17–36 months of follow-up.8,18,25,26 The reported rate of intraoperative and perioperative complications of LU can be as high as 30%, and such complications include bleeding, urinary leakage, epididymo-orchitis, port-site erythema, urinary retention, and ileus. 22 In our series, apart from minor intraoperative complications the only significant problem was ureteric injury. One patient in whom ureteral obstruction recurred after 4 months of LU was noncompliant and did not follow the postoperative drug regimen.
A debatable point is whether ureterolysis should be combined or not with ureteral intraperitonealization or omental wrapping. Although there is no proven basis for these additional steps, ureterolysis done as an isolated procedure is assumed to have more chance of recurrences. In our experience omental wrapping adds only a few extra minutes to the total operative time.
Drawbacks of this series include its retrospective nature and the small number of cases. However, our results indicate that LU with omental wrapping in patients with RPF and obstructive uropathy can be safe and effective and thus a valid option with a high success rate.
Conclusions
LU with omental wrapping in the setting of obstructive uropathy provides all the advantages of minimal invasiveness and is a safe and effective alternative with a high success rate at mid- to long-term follow-up.
Footnotes
Disclosure Statement
No competing financial interests exist.