
Abstract
Abstract
Objective:
To conduct a meta-analysis of studies that compared transperitoneal (TP) and extraperitoneal (EP) robot-assisted radical prostatectomy (RARP).
Materials and Methods:
PubMed, the Cochrane Library, and EMBASE online databases were searched for studies released prior to June 2012. References were manually reviewed, and two researchers independently extracted the data. To assess the quality of the studies, the Scottish Intercollegiate Guidelines Network Methodology Checklist for case-control and cohort studies was applied.
Results:
One randomized controlled trial and five case-control studies were identified that met the inclusion criteria. Within these studies, 530 patients underwent EP-RARP, and 312 patients underwent TP-RARP. Operating room (OR) time for EP was shorter than for TP (mean difference, −25.551; 95% confidence interval [CI] −41.668 to −9.434; P=.002). For estimated blood loss, there was no significant difference between EP and TP (mean difference, −12.111; 95% CI −44.087 to 19.865; P=.458). There was a statistical difference in length of stay (LOS) between EP and TP patients (mean difference, −0.488; 95% CI −0.964 to −0.012; P=.044). There was no significant difference in margin positivity between EP and TP (odds ratio=1.023; 95% CI 0.656–1.573; P=.918). In complications including grade 2 or more than 2, there was also no difference between EP and TP (odds ratio=0.610; 95% CI 0.341–1.089; P=.094).
Conclusions:
This meta-analysis suggests that perioperative parameters, including OR time and LOS, may be more favorable for EP-RARP than for TP-RARP. However, the oncologic outcome of margin positivity did not demonstrate a significant difference between the EP and TP approaches.
Introduction
Gettman et al. 5 reported the first clinical cases of extraperitoneal (EP) RARP (EP-RARP) in 2003, and several studies have compared the oncological outcomes and complications of transperitoneal (TP) RARP (TP-RARP) versus EP-RARP. Atug et al. 6 showed that EP-RARP is comparable to TP-RARP and also produces favorable outcomes. Madi et al. 7 also reported that EP-RARP offers similar clinical outcomes to TP-RARP but that EP-RARP avoids potential bowel injury or complications related to an intraperitoneal urine leak. Lee et al. 8 suggested that EP-RARP may be the best alternative in robotic radical prostatectomy, considering the potential risk of bowel injury with TP-RARP and the reduced peritoneal irritation with EP-RARP. Recently, Davis et al. 9 suggested that potential indications for EP-RARP may be patients with histories of previous abdominal surgery, symptomatic inguinal hernia needing mesh repair, or cardiac disease with inserted drug-eluting stents.
Some studies have reported that EP-RARP may be similar or superior to TP-RARP in terms of perioperative outcomes 10 ; however, a systematic review or meta-analysis comparing EP-RARP and TP-RARP has not been published. Thus, we conducted a meta-analysis of studies that compared the TP versus the EP approach in RARP.
Materials and Methods
Inclusion criteria
Randomized controlled trials (RCTs) or case-control trials that met the following criteria were included: (1) a study design that included comparison of the TP and EP approaches in RARP for prostate cancer; (2) the study provided accurate perioperative data that could be analyzed, including the total number of subjects and the values of each index; and (3) the full text of the study could be accessed.
Search strategy
A comprehensive computer literature search for abstracts was performed to identify articles that compared the TP versus the EP approach in RARP. A systematic review of original articles that analyzed perioperative outcomes between TP- and EP-RARP and were published between 2001 and June 2012 was conducted. A literature search of PubMed, the Cochrane Library, and EMBASE online databases was performed using the key words “prostatectomy,” “robot,” and “extraperitoneal.” The searches were restricted to English language publications.
Data extraction
One researcher (J.Y.L.) screened the titles and abstracts identified by the search strategy. The other two researchers (K.S.C. and R.R.D.) independently assessed the full text of the articles for meeting of the inclusion criteria. The database was designed to ensure the most relevant data with respect to author, year of publication, demographics of the patients, tumor characteristics, geographic location, period of recruitment, study design, and inclusion of a reference standard. The data extracted from articles included perioperative data presented as the mean value with P values, including operating room (OR) time and estimated blood loss (EBL), and standard deviations were obtained according to the method of the Cochrane Handbook for Systematic Reviews of Interventions (http://handbook.cochrane.org/). 11 Complications in each study were recategorized according to the Clavien–Dindo classification. 12 Disagreements were resolved by discussion until a consensus was arrived at, or by arbitration using another researcher (Y.D.C.).
Study quality assessment
Once the final group of articles was agreed upon, two researchers (J.Y.L. and R.R.D.) independently examined the quality of each article using the Scottish Intercollegiate Guidelines Network (SIGN) as a quality assessment tool for observational studies. 13 This system is internationally accepted and is used by guideline developers. Flay et al. 14 for the Society for Prevention Research and Kumpfer and Alvarado 15 have published similar rating scales, which require an even higher level of evidence (when such evidence comes from RCTs or case-control trials performed by multiple independent research groups) and stricter criteria for assessing the quality of the research. 16 For quality assessment, four categories were used to categorize the design quality of a study: “low” (score of 0–14); “modest” (score of 14.5–19); “good” (score of 19.5–24); or “very good” (score of 24.5–30).
Heterogeneity test
Heterogeneity among the studies was explored using the Q statistic and Higgins' I2 statistic.17,18 Higgins' I2 measures across studies for the percentage of total variation due to heterogeneity rather than chance. Higgins' I2 is calculated as follows:
where Q is Cochran's heterogeneity statistic and df is the statistical degrees of freedom.
An I2 of >50% is considered to represent substantial heterogeneity. For the Q statistic, heterogeneity was deemed to be significant for P<.10. 19 When there was evidence of heterogeneity, data were analyzed using a random-effects model to obtain a summary estimate for the test sensitivity with 95% confidence intervals (CIs) after the secondary examination of heterogeneity in the random-effects model using a radial plot. 20 Studies in which positive results were confirmed were conducted using a pooled specificity with 95% CIs.
Statistical analyses
When a significant Q test indicated heterogeneity across studies (P<.10 or I2>50%), the random-effects model was used for the meta-analysis; otherwise, the fixed-effects model was used. 21 The data for heterogeneity were verified again using the radial plot by the method of Galbraith 20 after selection of each model for parameters. The Begg–Mazumdar rank-correlation test and Egger's regression intercept test were used to provide evidence of publication bias,22,23 which was shown as a funnel plot (P<.05 was considered a significant publication bias). The meta-analysis of comparable data was carried out using R software (R version 2.15.3; R Foundation for Statistical Computing, Vienna, Austria) (www.r-project.org) and its metafor package for meta-analyses.
Results
Eligible studies and quality assessment
The database search found 45 articles that could potentially have been included in the meta-analysis. Based on the inclusion and exclusion criteria, 39 articles were excluded after a simple reading of the titles and abstracts of the articles, including two that lacked a full text version. In total, six articles were included in the analysis (Fig. 1).6,7,24–27 The six eligible studies included 530 patients who had undergone EP-RARP and 312 who had undergone TP-RARP. The publication year of the studies ranged from 2006 to 2012. Four studies were conducted in the United States,6,7,24,26 one was conducted in Korea, 25 and one was conducted in Switzerland. 27 Only one RCT 24 and five case-control trials were selected (Table 1). Of the six enrolled articles, the final assessment results quality was deemed to be “low” in two articles6,7 and “modest” in four articles,24–27 according to the SIGN checklists.

Flow diagram of the study selection.
BMI, body mass index; EBL, estimated blood loss; LOS, length of stay; NA, not available; OR, operating room; PSA, prostate-specific antigen; RARP, robot-assisted radical prostatectomy; SMR, surgical margin rate.
Heterogeneity assessment
A heterogeneity test of OR time, EBL, hospitalization length of stay (LOS), complication rate, and surgical margin rate (SMR) showed the following: for OR time, chi-squared=13.468 with 5 df (P=.013) and I2=65.44%; for EBL, chi-squared=11.083 with 5 df (P=.050) and I2=54.89%; for LOS, chi-squared=16.001 with 3 df (P=.001) and I2=81.25%; for SMR, chi-squared=1.234 with 4 df (P=.872) and I2=0%; and for rate of complications including grade 2 or more than 2, chi-squared=0.550 with 3 df (P=0.908) and I2=0%. Notable heterogeneities were detected in OR time, EBL, and LOS; thus random-effect models were used to further assess these three variables. In radial plots, no variable demonstrated heterogeneity after selection of effect models for each variable (Fig. 2).
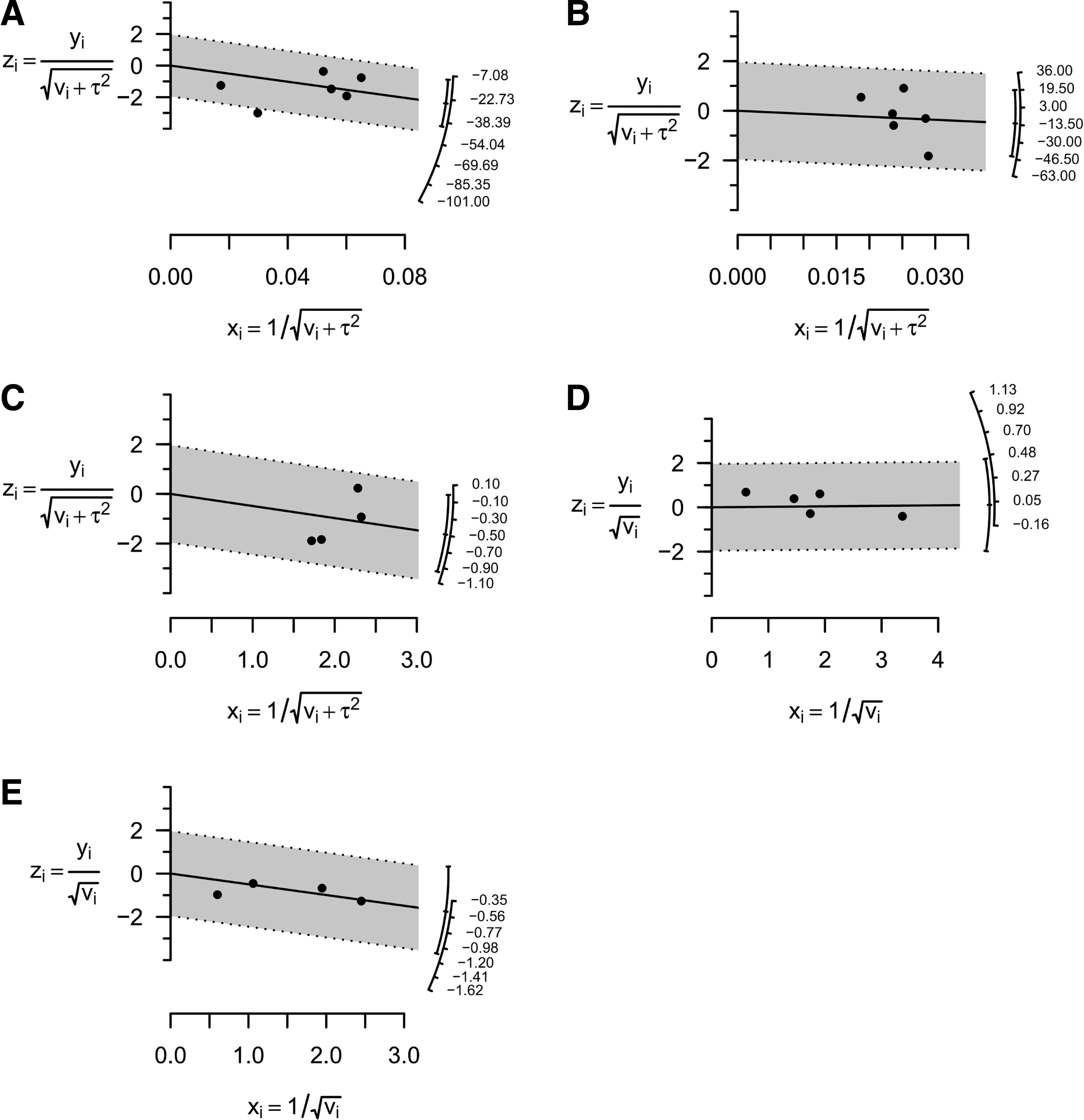
Radial plots demonstrated that no variable demonstrated heterogeneity after selection of effect models:
Publication bias assessment
The Begg–Mazumdar rank-correlation test showed no evidence of publication bias in the present meta-analysis for OR time (P=.452), EBL (P=0.452), LOS (P=1.000), SMR (P=.221), and complication rate (P=.750). Egger's regression intercept test also revealed no evidence of publication bias in OR time (P=.614), EBL (P=.352), LOS (P=.861), SMR (P=.112), and complication rate (P=.960). Funnel plots detailing these results, including OR time, EBL, LOS, SMR, and complication rate, are shown in Figure 3.
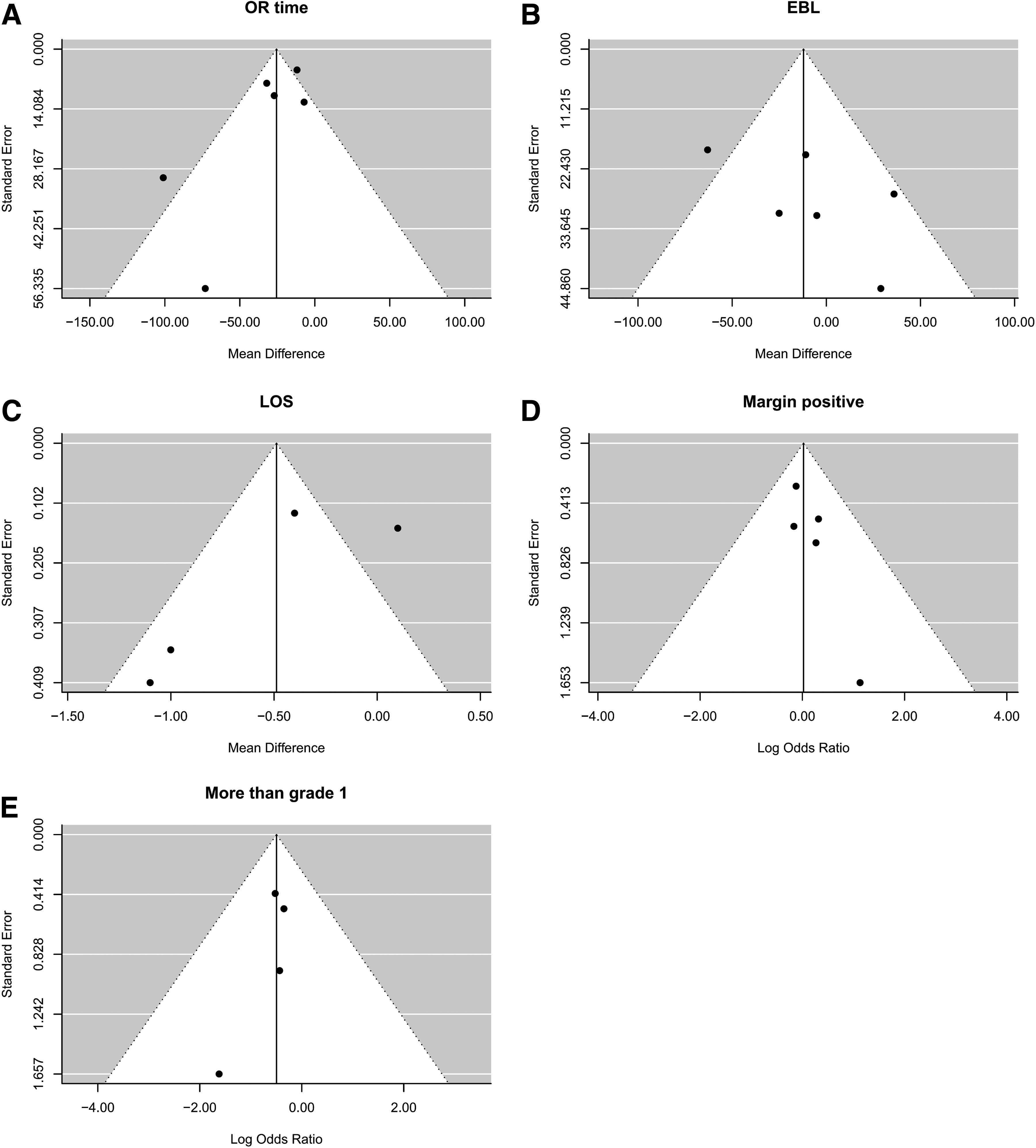
Funnel plots for publication bias for
Comparison of TP and EP approaches in RARP
Forest plots for OR time, EBL, LOS, SMR, and complications rate are given in Figure 4. OR time for EP was relatively shorter than for TP (mean difference, −25.551; 95% CI −41.668 to −9.434; P=.002; Fig. 4A). For EBL, there was no significant difference between EP and TP (mean difference, −12.111; 95% CI −44.087 to 19.865; P=.458; Fig. 4B). LOS for EP was also relatively shorter than for TP (mean difference, −0.488; 95% CI −0.964 to −0.012; P=.044; Fig. 4C). For SMR, the meta-analysis revealed an odds ratio of 1.023 (95% CI 0.656–1.573; P=.918; Fig. 4D). In rate of complications including grade 2 or more than 2, there was also no difference between EP and TP (odds ratio=0.610; 95% CI=0.341–1.089; P=.094; Fig. 4E).

Meta-analysis forest map of risk ratio between the extraperitoneal and transperitoneal approaches in robot-assisted radical prostatectomy for
Discussion
The use of RARP has increased substantially in both the United States and Europe, and it is estimated that more than 75% of radical prostatectomies are performed using the da Vinci® Surgical System platform (Intuitive Surgical Inc., Sunnyvale, CA).28,29 RARP is generally superior to RRP with regard to functional outcomes. 30 Advantages of RARP include the 10 times magnified binocular, three-dimensional visualization, motion scaling with tremor filtration, improved surgical ergonomics, and miniature articulating instruments with seven degrees of freedom. These capabilities provide improved precision and comfort versus manual approaches and thus facilitate dissection of tissue planes and meticulous suturing.
Previous studies have shown that EP-RARP and TP-RARP have equal oncological and functional outcomes. Although comparative shortcomings of EP-RARP include limited working space and time-to-port installation, the EP approach may have advantages over TP-RARP, including less OR time and EBL and shorter hospital LOS and recovery times. Our study is the first systematic review and meta-analysis comparing EP- and TP-RARP. Our meta-analysis quantitatively assessed the results of prior studies that had compared the perioperative outcomes of the TP and EP surgical approaches.
We found that OR time was shorter with EP-RARP than with TP-RARP. Despite the slightly longer time-to-port installation with the EP approach, a significantly shorter overall surgical time using EP-RARP was described in the literature and was confirmed by our meta-analysis. This shorter overall surgical time was mainly achieved by a shorter console time in EP-RARP due to the fact that no further mobilization of the peritoneum and the bladder was necessary. 27 In the six studies that were included in our meta-analysis, the skill level of the surgeons performing the TP-RARP and EP-RARP was detailed. Therefore, a possible confounding factor may be the factor of the experience level of the surgeon and/or assistant who performed EP-RARP compared with TP-RARP. For EBL, there was no statistical difference using random-effects models. Only two of the six selected articles showed that EBL in EP-RARP was significantly less than for TP-RARP, and four articles found no difference in EBL between the EP and TP approaches. Data concerning LOS were extracted from four studies: the two studies from the United States6,26 averaged only 1 day, but in one study each from Korea 25 and Switzerland, 27 LOS was longer (range, 5.1–8.8 days).
The complications following EP-RARP and TP-RARP are shown in Table 2 according to the Clavien–Dindo classification. 12 In fact, one of the most important advantages of EP-RARP is using the peritoneum as a natural barrier. The peritoneum during and after the EP procedure still functions as a natural barrier, minimizing the likelihood of persistent ileus occurrence because the bowel is minimally manipulated and there is no leakage of intraperitoneal fluids. 31 Additionally, the EP approach is associated with a reduced number of accidental thermal injuries to the intestines, due to peritoneal sequestering of the bowels outside of the operating field. Moreover, bowel injuries that infrequently occur during trocar insertion and dorsal dissection of the overlying rectum prostatic apex are considered a less severe complication with EP access versus the TP approach because the risk of generalized peritonitis is diminished. 32 However, the studies included in our meta-analysis were assessed as modest or low grade in SIGN checklists and used quite different categories to evaluate complications in each. There were some difficulties in analyzing comparisons of complications between TP and EP. For grade 1 complications, including postoperative ileus, EP may be superior to TP, pointing to one advantage of EP-RARP over TP-RARP. However, grade 2 or more than 2 complications did not demonstrate a significant difference between TP and EP. The complications arising from each procedure showed little difference except for complications that might result from procedural injury or underlying disease.
Data are number of cases.
EP, extraperitoneal; TP, transperitoneal.
Considering surgical margin positivity, there were no significant differences between TP and EP. Previous studies revealed that open and laparoscopic approaches had similar oncological outcomes. 33 Surgical margin positivity is a unique marker of oncologic outcome that can be extracted from previous series. Postsurgical functional analysis should include oncologic outcomes, as well as recovery of continence and potency, when comparing TP and EP approaches in RARP.
There were some limitations in our meta-analysis. Although all cases and controls from each study were well defined with similar inclusion criteria, there may be potential factors that were not taken into account that may have influenced our study selection for inclusion in a meta-analysis. Second, data on oncologic and functional outcomes were not available in the original articles. In particular, pathologic stage, biochemical recurrence, and recovery of potency and of continence were not included, and confounding factors might have introduced bias.
Conclusions
Considering operative outcomes extracted from previous studies, OR time and LOS were relatively shorter and complication rates were lower when EP-RARP was used rather than the TP approach. However, EBL, surgical margin positivity, and complication rate did not show significant differences. Further RCTs comparing the TP and EP approaches should be conducted in larger patient populations to definitively assess potential differences in perioperative parameters and postoperative outcomes.
Footnotes
Acknowledgments
This study was supported by grant A084120 from the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea, and grant CB-2011-04-02 from the Korean Foundation for Cancer Research.
Disclosure Statement
No competing financial interests exist.