
Abstract
Abstract
Objective:
To evaluate the safety and effects on health-related quality of life (HRQOL) of radical excision of deeply infiltrating endometriosis (DIE) in the cul-de-sac.
Patients and Methods:
This study included 390 patients with pathologically proven DIE in the cul-de-sac who underwent laparoscopic surgery between January 2000 and December 2011. The preoperative and postoperative visual analog scale (VAS) pain scores and HRQOL data from the 36-item Short Form (SF-36) questionnaire were recorded in 343 patients. Surgical outcomes, complications, and HRQOL were compared between patients who underwent hysterectomy and those who did not. Data were analyzed using the paired t test, Student's t test, and Pearson's correlation analysis.
Results:
In the group overall, the VAS pain score and all SF-36 scales improved after surgery. In patients who underwent hysterectomy, all SF-36 scales improved except physical functioning, role-physical, general health, and vitality. In patients who did not undergo hysterectomy, all SF-36 scales improved except general health. There were significant associations between gonadotropin-releasing hormone agonist therapy and SF-36 mental health, SF-36 mental component summary, and oral medication use. The VAS pain score and SF-36 body pain score showed the greatest improvement, and the SF-36 general health score showed the least improvement. Patients who underwent hysterectomy had more severe disease and poorer surgical outcomes than those who did not undergo hysterectomy.
Conclusions:
Laparoscopic radical excision of DIE in the cul-de-sac is safe and significantly improves HRQOL, especially in terms of pain. The severity of endometriosis may affect the degree of improvement in HRQOL scores.
Introduction
E
As deeply infiltrating endometriosis (DIE) cannot be completely resolved with medical treatment, complete resection of the lesions is necessary. The goals of surgery are to reduce pelvic pain, increase quality of life (QOL), prevent recurrence, and increase the pregnancy rate. 4 To accomplish these goals, the distorted pelvic anatomy must be restored to normal.
In patients with DIE in the cul-de-sac, Douglasectomy with radical excision is the only definitive procedure for restoration of the normal anatomy of the pelvic floor and effective reduction of pelvic pain. This procedure should only be performed by experienced gynecologists because of the high risk of injury to adjacent organs. The effects of this procedure on QOL are still debated.
This study evaluated the safety and effects on health-related QOL (HRQOL) of laparoscopic Douglasectomy with radical excision for DIE in the cul-de-sac and compared postoperative HRQOL between patients who underwent laparoscopic Douglasectomy with hysterectomy and those who did without.
Patients and Methods
This study included 390 patients with pathologically proven DIE in the cul-de-sac who underwent laparoscopic Douglasectomy between January 2000 and December 2011 at Kyungpook National University Hospital or Medical Center (Daegu, South Korea). The medical records were reviewed to extract patient age, body mass index, previous operation history, type of surgical procedure, operation time, estimated blood loss, change in hemoglobin concentration, change in serum cancer antigen 125 (CA-125) level, and complications. The preoperative and postoperative visual analog scale (VAS) pain scores and HRQOL data from the 36-item Short Form (SF-36) questionnaire were recorded. Picture archives and communication system images of the 390 patients were reviewed. Surgical outcomes, complications, and HRQOL were compared between patients who underwent laparoscopic Douglasectomy with hysterectomy and those who did without.
Douglasectomy was performed together with other surgical procedures including hysterectomy, myomectomy, oophorectomy, cystectomy, and incidental appendectomy. At our institute, Douglasectomy with radical excision for DIE is performed as follows. First, the surgeon bluntly dissects the dense adhesions in the cul-de-sac between the bowel and the uterus and adnexae using a uterine manipulator and laparoscopic chisel. The ureter is identified where it crosses the iliac vessels and is dissected caudally until it enters the ureteral tunnel roofed by the vesicouterine ligament. Bilateral pararectal spaces are formed. Thick uterosacral liagament and the endometriotic lesions in the cul-de-sac are removed. The posterior vaginal wall and anterior rectal serosa are separated using a rectal probe (Fig. 1). Further procedures are then performed depending on the extent of endometriotic lesions, including hysterectomy, myomectomy, and cystectomy. If hysterectomy is needed, this is performed after complete dissection of the ureter to the ureteral tunnel, to avoid ureteric injury. Invasion into the rectal serosa is removed by a shaving technique using scissors. Invasion into the rectal muscle or mucosa is removed by low anterior resection, with the resected colon removed through the vagina, and colorectal anastomosis is performed using a circular stapler (Fig. 2).

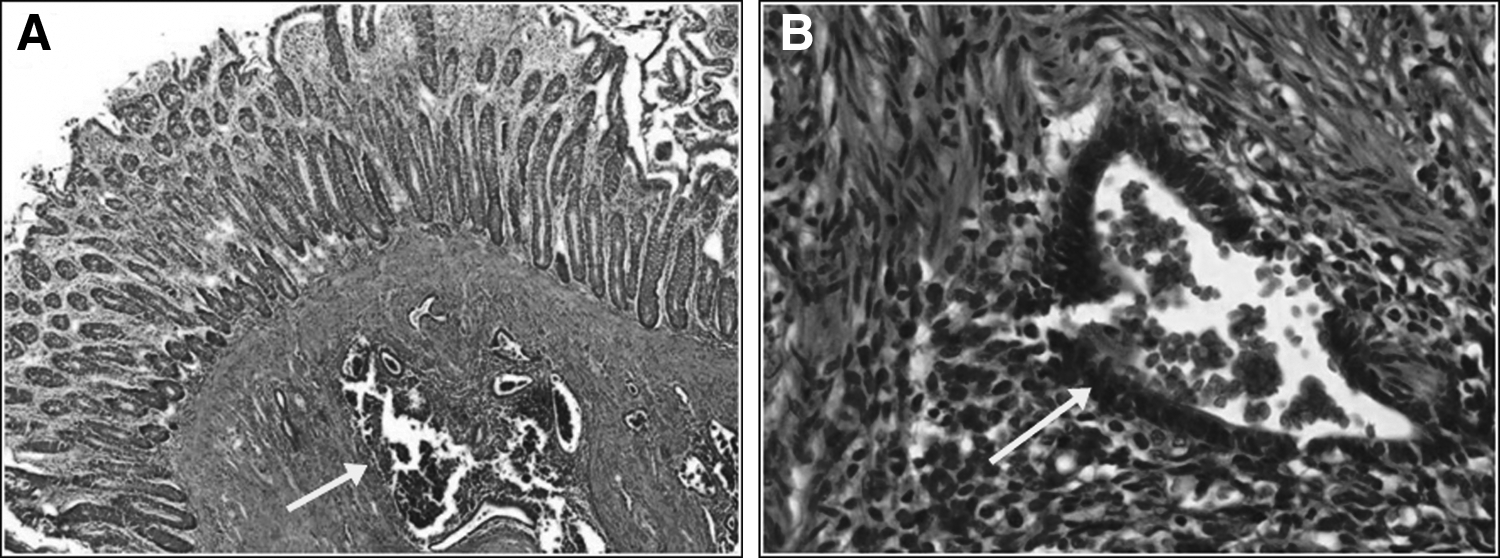
Hematoxylin and eosin stain of the colon muscular layer.
VAS pain score and SF-36 data were available for 343 of the 390 patients, including 56 who underwent hysterectomy (hysterectomy group) and 287 who did not undergo hysterectomy (nonhysterectomy group). The SF-36 is a multipurpose health survey with 36 questions that provides results in eight scales: the physical functioning (PF), role-physical (RP), and body pain (BP) scales contribute to the physical component summary (PCS); the mental health (MH), role-emotional (RE), and social functioning (SF) scales contribute to the mental component summary (MCS); and the vitality (VT) and general health (GH) scales contribute to both PCS and MCS. The preoperative and 9-month postoperative VAS pain scores and SF-36 data were compared. Norm-based scoring of the SF-36 is based on scores in the general population. Scores can be transformed so that they range from 0 to 100, and scores above or below 50 can be interpreted as being above or below the norm for the general population. As the standard deviation for each scale is set at 10, it is easy to determine how far above or below the norm any score lies. A score beyond 1.96 standard deviations (20 points) above or below the norm indicates with 95% confidence that the sample is more or less healthy, respectively, than the general population. 5
Based on the distribution of VAS pain scores in postoperative patients who described their postoperative pain intensity as none, mild, moderate, or severe, the following cutoff points on a VAS of 0–100 mm are recommended: no pain, 0–4 mm; mild pain, 5–44 mm; moderate pain, 45–74 mm; and severe pain, 75–100 mm. 6
Statistical analyses were performed using Statistical Package for Social Sciences software (SPSS, Inc., Chicago, IL). Patient characteristics and surgical outcomes were compared between the hysterectomy and nonhysterectomy groups using Student's t test. The relationships between patient characteristics and the VAS pain score and SF-36 scales were analyzed using Pearson's correlation analysis. The postoperative changes in VAS pain score and SF-36 scales, clinical outcomes, and surgical outcomes were compared between the hysterectomy and nonhysterectomy groups using the paired t test. A value of P<.05 was considered statistically significant. The Institutional Review Board of Kyungpook National University Medical Center approved the study protocol. Written informed consent for treatment and inclusion in this study was obtained from each subject.
Results
There were significant differences between the hysterectomy and nonhysterectomy groups in age (P<.01) and body mass index (P=.02). Incidental appendectomy was performed in 59% of patients in the hysterectomy group and 62% of patients in the nonhysterectomy group. Bowel resection to remove invasion by endometriosis was performed in 6 patients in the hysterectomy group only. The hysterectomy group had a significantly longer operation time (P<.01) and larger volume of estimated blood loss (P<.01) than the nonhysterectomy group. There were no significant differences between the two groups in the change in hemoglobin concentration (P=.72) or change in serum CA-125 level (P=.46).
In the hysterectomy group, perioperative complications occurred in 5 patients (6.6%), including moderate hydronephrosis (n=1) that required postoperative double-J catheter insertion, pelvic abscess (n=1), vaginal stump suture site bleeding (n=2), and bowel leakage that required reoperation (n=1). In the nonhysterectomy group, there were no severe perioperative complications, and perioperative complications occurred in 10 patients (3.1%), including mild hydronephrosis (n=1), rectal serosal injuries that were repaired intraoperatively (n=2), pelvic abscess (n=2), postoperative fever (n=2), vaginal wall suture site disruption (n=1), significant intraoperative venous bleeding that was controlled by coagulation (n=1), and significant intraoperative arterial bleeding (caused by injury to the left internal iliac artery) that was controlled by coagulation (n=1) (Table 1).
Data are mean±SD values or number (%). Statistical significance was analyzed with Student's t test.
BMI, body mass index; CA-125, cancer antigen 125; DJ, double-J catheter; Hb, hemoglobin.
In the group overall, the VAS pain score and all SF-36 scales improved after surgery. In the hysterectomy group, all SF-36 scales improved after surgery except for PF (P=.17), RP (P=.19), GH (P=.09), and VT (P=.06). In the nonhysterectomy group, all SF-36 scales improved after surgery except for GH (P=.6) (Table 2).
These data were analyzed for statistical significant with the paired t test.
P>.05 is not considered statistically significant.
BP, body pain; GH, general health; MCS, mental component summary; MH, mental health; PCS, physical component summary; PF, physical functioning; RE, role-emotional; RP, role-physical; SF, social functioning; SF-36, 36-item Short Form; VAS, visual analog scale; VT, vitality.
The relationships between patient characteristics and the VAS pain score and the eight SF-36 scales are shown in Table 3. There were significant associations between gonadotropin-releasing hormone agonist (GnRH-a) therapy and the SF-36 MCS score (coefficient, 0.47; P=.04) and between oral medication use and the SF-36 MH score (coefficient, −0.46; P=.04).
Data are correlation coefficient (CE) and statistical significance (P). These data were analyzed with Pearson's correlation analysis.
P<.05 is considered statistically significant.
BMI, body mass index; BP, body pain; CA-125, cancer antigen 125; GH, general health; GnRH, gonadotropin-releasing hormone; Hb, hemoglobin; MCS, mental component summary; MH, mental health; PCS, physical component summary; PF, physical functioning; RE, role-emotional; RP, role-physical; SF, social functioning; VAS, visual analog scale; VT, vitality.
The data are complicated, and it is difficult to understand the changes in HRQOL. Figure 3 makes the results easier for the reader to understand. The graph shows the changes in the VAS pain score and SF-36 scales after surgery, especially the BP and GH scores. Figure 3 shows that the VAS pain score decreased and all SF-36 scales increased after surgery. Decrease in VAS pain score and increase in SF-36 scales mean improvement in QOL. The VAS pain score and SF-36 BP score showed the greatest improvement, and the SF-36 GH score showed the least improvement. In both groups, the slope of the SF-36 BP score was steeper than that of the SF-36 GH score. The SF-36 RH, RP, VT, SF, RE, and MH scores showed similar changes in both groups.
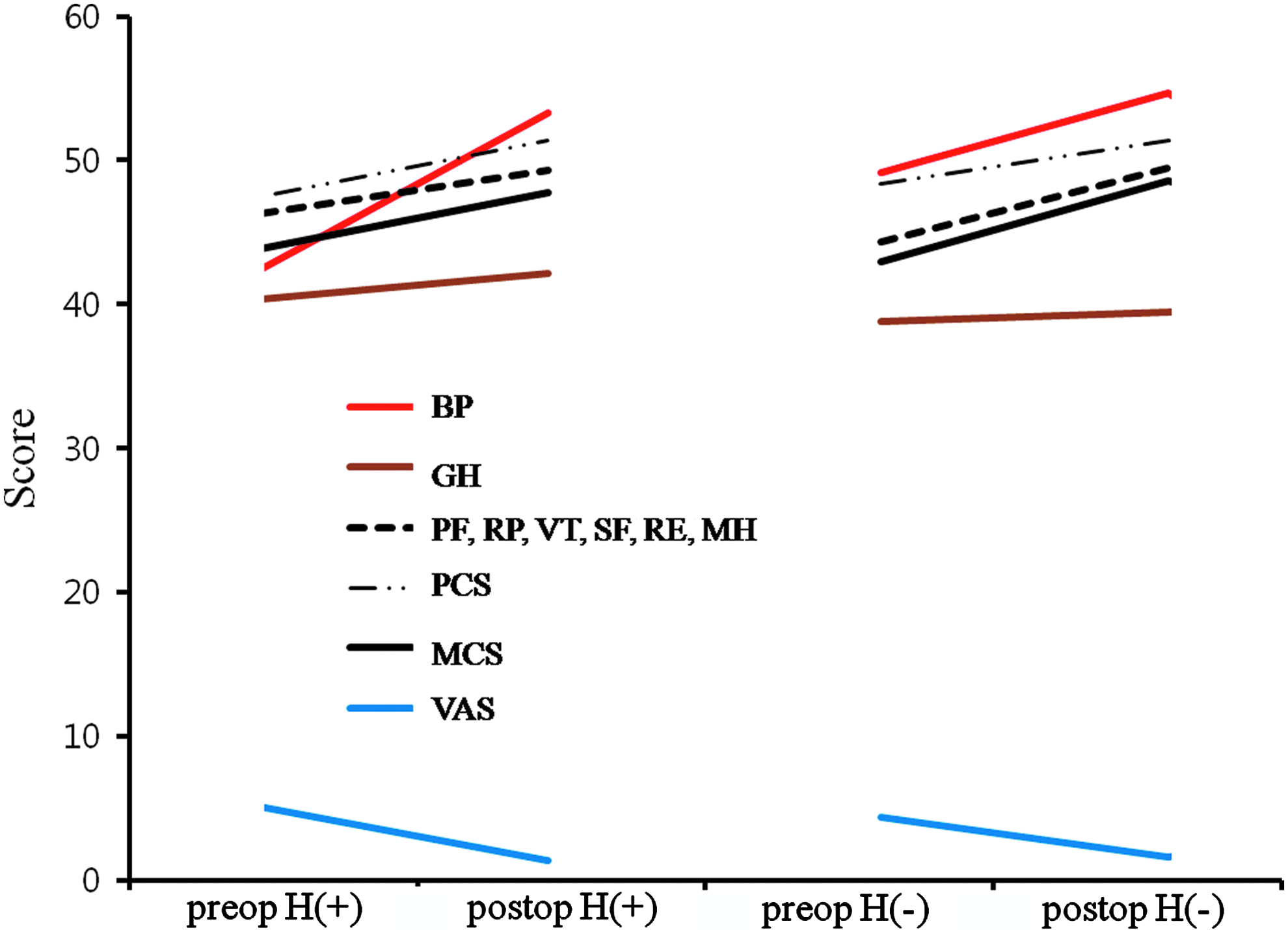
Interval changes in preoperative or postoperative scores of the 36-item Short Form and visual analog scale (VAS) in the hysterectomy [H(+)] and nonhysterectomy group [H(−)]. The physical functioning (PF), role-physical (RP), vitality (VT), social functioning (SF), role-emotional (RE), and mental health (MH) scales display similar interval changes. BP, body pain; GH, general health; MCS, mental component summary; PCS, physical component summary.
Discussion
Our results confirm that Douglasectomy is safe, reduces pelvic pain, and improves HRQOL. Open Douglasectomy was first reported in 1963, 7 and Douglasectomy is now regarded as the only definitive procedure for restoring the normal anatomy of the pelvis in patients with DIE in the cul-de-sac. Donez and Squifflet 8 described the classification, diagnosis, and surgical treatment of rectovaginal endometriosis or adenomyosis of the rectovaginal septum, both of which obliterate the cul-de-sac. They presented experimental evidence that the origin of rectovaginal endometriosis may differ from that of peritoneal endometriosis and suggested that rectovaginal endometriosis is not controlled by steroid therapy such as GnRH-a and should therefore be treated by surgical excision. Laparoscopic radical excision of endometriosis should be performed by appropriately trained surgeons to avoid complications and prevent inadequate treatment.
The complications of surgical treatment for DIE include bowel and urinary tract injuries, especially ureteral injuries. Donez and Squifflet 8 reported a rectal perforation rate during radical excision of rectovaginal endometriosis of 0.5% (10/1942 patients), including 2 patients who underwent repeat surgery to treat rectal perforation. In our study, the rate of rectal serosal injury or bowel leakage was 0.7% (3/390 patients), including 1 patient who underwent repeat surgery to treat bowel leakage after low anterior resection. Although this patient developed postoperative bowel leakage, there was no intraoperative thermal injury, and there were no other intraoperative complications associated with inadequate treatment. Douglasectomy is a safe procedure with a low rate of severe perioperative complications if it is carefully performed by an experienced surgeon.
In this study, patients were divided into hysterectomy and nonhysterectomy groups to compare the effects of surgery type and disease severity on HRQOL. Because of the differences in age and disease severity between the two groups, we compared the impact of surgery type on HRQOL rather than on surgical outcomes.
Radical excision of DIE has been reported to significantly improve QOL. 9 A recent prospective study reported that laparoscopic excision of DIE lesions resulted in significant improvement in all the SF-36 scales. Improved QOL was related to decreased dyspareunia and dysmenorrhea. 4 Complete laparoscopic resection of endometriotic lesions decreased the prevalence and intensity of deep dyspareunia, and improved QOL. 10 In patients with intestinal DIE, the effects of bowel resection on QOL are unclear.11–14 In this study, analysis of outcomes after bowel resection was limited by the small number of patients, but all patients who underwent bowel resection reported an improved HRQOL after surgery. In the group overall, there were significant improvements in the VAS pain score and all SF-36 scales after surgery. In the hysterectomy group, there were no significant improvements in the SF-36 PF, RP, GH, or VT scores after surgery, which differs from previously reported outcomes. In the nonhysterectomy group, there were significant improvements in all SF-36 scales except for GH.
In the hysterectomy group, the most frequent pathological diagnosis was adenomyosis (Stage IV, American Society for Reproductive Medicine Revised Classification of Endometriosis). This severe preoperative disease may have affected the subsequent improvement in HRQOL. The reason for the lack of improvement in the SF-36 GH score is likely to be multifactorial, including the patients' new information regarding their disease, postoperative GnRH-a therapy, and use of oral medications, which might detract from the patient's perceptions of her health status. The SF-36 MCS score was significantly higher in patients receiving GnRH-a therapy, and the SF-36 MH score was significantly lower in patients receiving oral medication. These results may reflect the emotional stress associated with drug therapy. However, it is not possible to reach any definitive conclusions because of the small number of patients and short follow-up period in this study. Mental health is expected to improve after long-term follow-up and cessation of drug therapy.
In conclusion, laparoscopic radical excision of rectovaginal endometriosis is safe if it is carefully performed by an experienced surgeon. This procedure significantly improves HRQOL, especially in terms of pain. Patient-assessed HRQOL may be affected by the severity of endometriosis and related lesions. Further studies are needed to identify other factors that may help to improve QOL.
Footnotes
Acknowledgments
The authors are grateful to the clinical coordinator, Y.J. Kim, and the assistant nurse, S.A. Lee, of the Gynecologic Cancer Center, Kyungpook National University Medical Center, for data collection and processing.
Disclosure Statement
No competing financial interests exist.