
Abstract
Abstract
Complete tubular colonic duplication is a rare and complex anomaly. We present a new technique consisting of anterior sagittal anorectoplasty and fenestration of the duplicated colon using a hybrid method, involving single-incisional laparoscope-assisted and endoscopic procedures, for a case of complete tubular colonic duplication associated with anovestibular and anocutaneous fistulas.
Introduction
C
Case Report
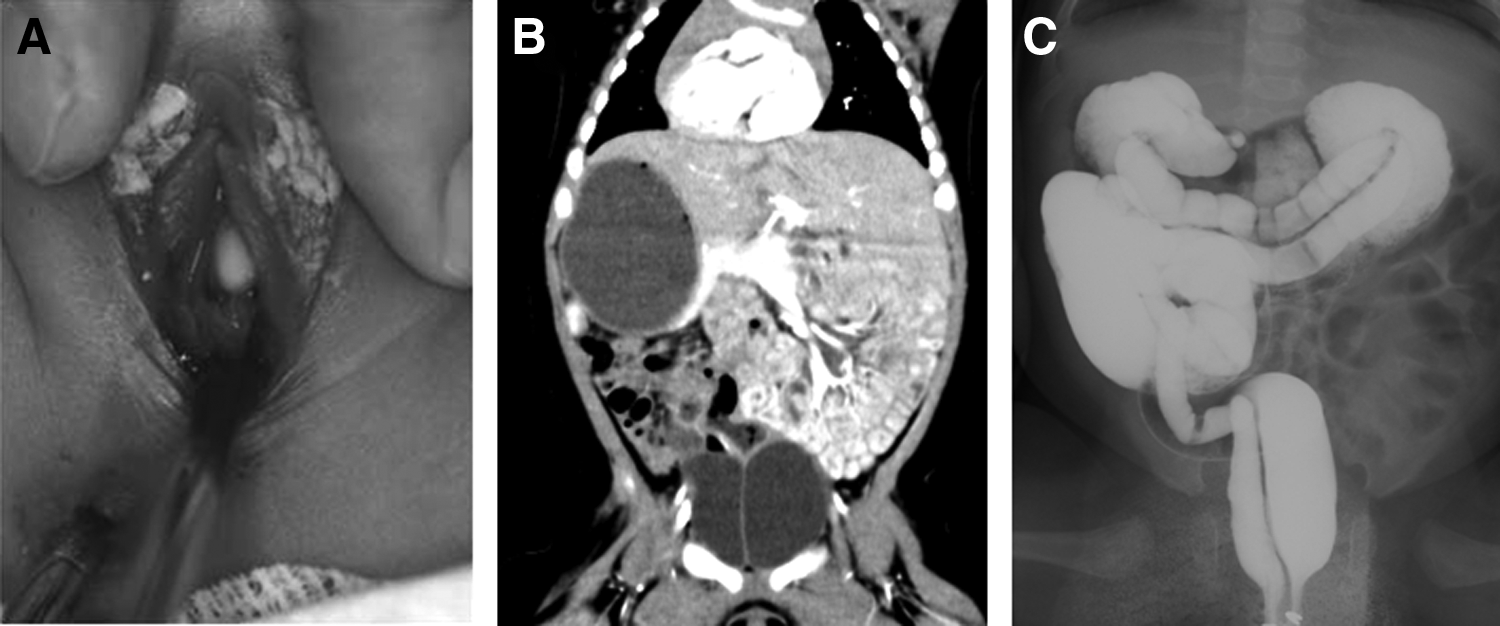
A 3030-g female baby presented with an anocutaneous fistula and anovestibular fistula through which fecal discharge was observed (Fig. 1A). Radiological evaluations revealed tubular duplication of the entire colon associated with dextrocardia with situs inversus and duplication of bladder, urethra, and vagina without a vertebral anomaly (Fig. 1B and C).
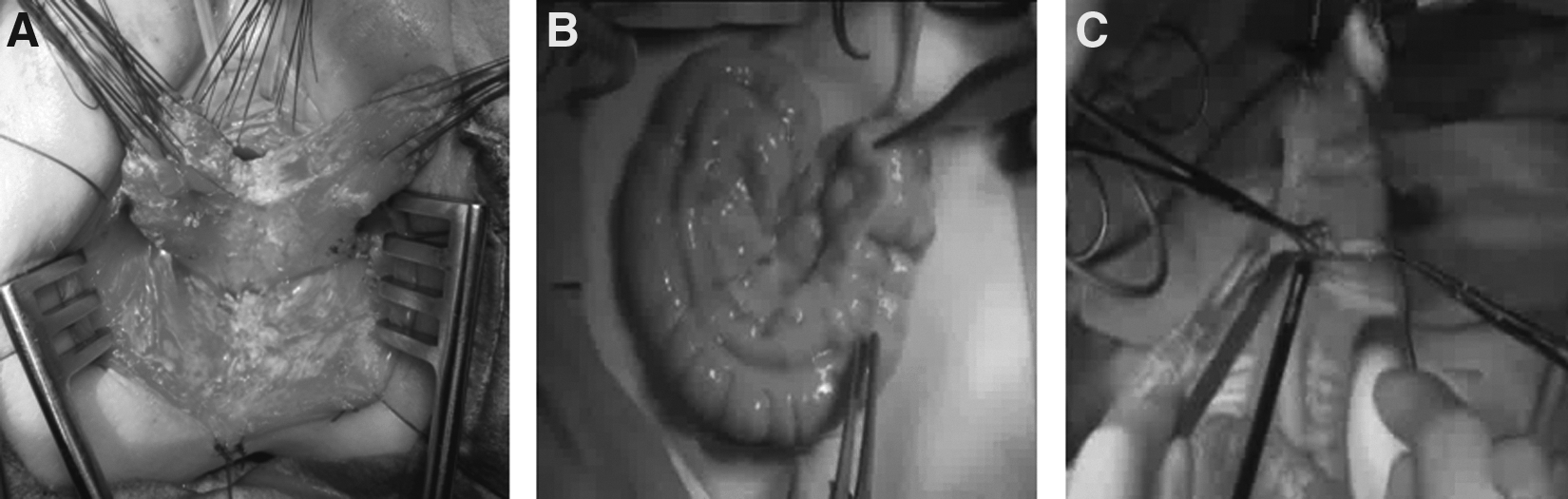
She underwent surgical repair at 9 months of age when she could undergo an endoscopic procedure. She was placed in the lithotomy position to facilitate both laparoscopic and perineal procedures. An anterior sagittal incision was made from the vestibule of the vagina to the center of the anal complex, and both 1.5-cm-long both fistulae were excised while preserving the puborectal muscle (Fig. 2A). The duplicated anus was reconstructed into a single lumen with division of the common septum using a tissue-sealing system (EnSeaL®; Ethicon, Tokyo, Japan). A semicircular umbilical incision was successively made. Single-port laparoscopic surgery revealed mesenterium commune associated with no fixation of the entire colon. The terminal ileum and colon were exteriorized through the umbilical wound. Complete tubular colonic duplication supplied by a single leaf of a mesentery was confirmed (Fig. 2B). The duplicated colon was on the mesenteric aspect of the main colon. After appendectomy for mesenteric commune, a small transverse colotomy was placed in the ascending colon, and a common septum of duplication was fenestrated using the tissue-sealing system (Fig. 2C). Additional small transverse colotomies were placed, and small spatulas were inserted into each colonic lumen to extend the septum for the prevention of thermal injury of the colonic wall due to the tissue-sealing system (Fig. 3). A linear stapling device was used to divide the septum of the stenotic sigmoid duplication. After the colostomies were closed, the sigmoid colon was clamped by the intestinal forceps, and a colonoscope was inserted through the anus. The residual anorectal duplication was divided endoscopically using a monopolar endoscopic device (SB knife Jr™; Sumitomo Bakelite, Tokyo) that had 3.5-mm-long blades (Fig. 4). Although the septum was thick, a monopolar endoscopic device divided the septum into three parts: the bilateral mucosal layers and the mid-muscular layer. It took more than 1 hour to divide the 20-cm-long septum. The reconstructed rectum was mobilized to the neoanus, and anorectoplasty was performed.
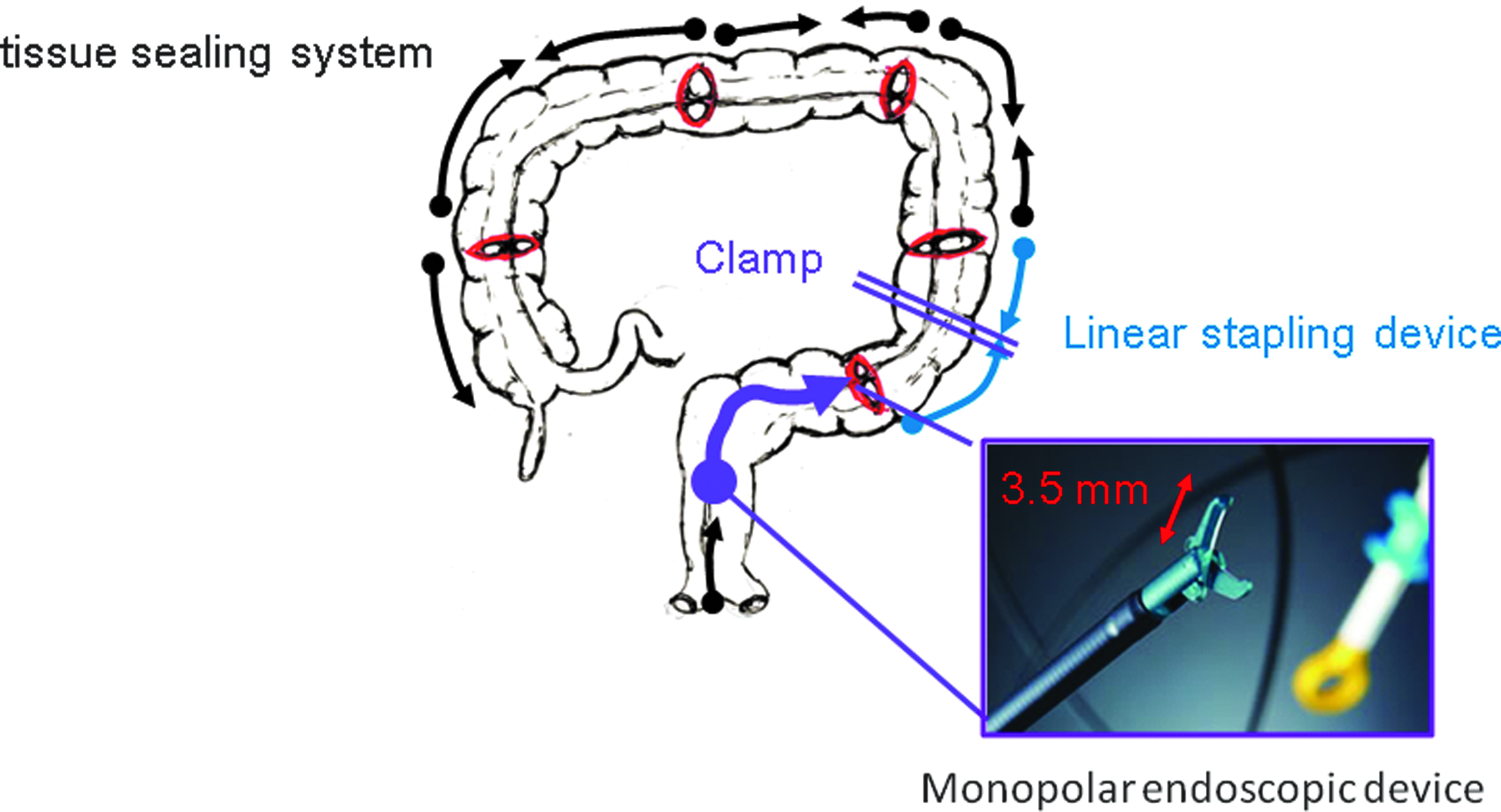
Five small transverse colotomies (red ovals) were placed. The tissue-sealing system (black arrows) and a linear stapling device (blue arrows) were used to divide the septum of the colonic duplication. The residual anorectal duplication was divided endoscopically using a monopolar endoscopic device (purple arrow).

The postoperative course was uneventful. At the 1-year follow-up, normal defecation and urination were observed. Colonoscopy revealed that the divided septum was completely healed and covered normal colonic mucosa.
Discussion
Complete tubular colonic duplication is a rare and complex anomaly. Tubular colonic duplication shares the same mesenteric vasculature and does not involve ectopic gastric mucosa. Yousefzadeh et al. 2 analyzed 57 patients with tubular colonic duplication, and 80% of these patients had associated urogenital anomalies, most notably genital and bladder duplication. Fifty percent of patients had some form of fistula. The present case showed total colonic duplication with two fistulas without proximal communication between the main and duplicated colon and that were associated with duplication of the urogenital system.
Patients who have a blind ending or a fistula or those with obstruction and constipation require surgical repair in the presence of complete tubular colonic duplication. Several surgical techniques have been described for the management of complete tubular colonic duplication. It is important not to leave the stenotic or obstructive lesion to avoid the occurrence of fecal impaction, constipation, or recurrence. Total fenestration between the main and duplicated colon is warranted to prevent defecation problems caused by a fecal mass at the stenotic segment.3,4 A colotomy and excision of the common septum to create an anastomosis between the main and duplicated colon using a linear stapling device have been successfully performed. 4 Total fenestration using a linear stapling device may have an adverse effect on the normal growth and peristalsis of the colon. In place of a linear stapling device, we used a tissue-sealing system to divide the septum. The tissue-sealing system facilitated hemostasis. However, considerable care was required to prevent thermal injury of the colonic wall. The presence of a stenotic lesion (stenotic sigmoid duplication in the present case) necessitates a linear stapling device to divide the septum.
Division of the anorectal septum is difficult. It is important to divide the septum as low as possible from the distal portion of the duplication to avoid the occurrence of fecal impaction, constipation, or a recurrent fistula.3,5 A posterior sagittal anorectal plasty may be performed together with either resection of the duplication, mucosectomy of the distal part of the duplicated colon, or anastomosis between the main and duplicated colon. Although the present case had anovestibular and anocutaneous fistulas, anterior instead of posterior sagittal anorectoplasty was performed to achieve fecal continence while preserving the puborectal muscle. 6
Less invasive surgery is desired for pediatric surgical cases. This is the first case of tubular colonic duplication involving an endoscopic procedure to divide the anorectal septum. Division of anorectal septum was performed using a monopolar endoscopic device that facilitated hemostasis. Total endoscopic division of the septum could be performed, but it takes a long time to complete. Moreover, intestinal clamp use was mandatory to provide adequate insufflation for endoscopic division.
The present hybrid method, involving single incisional laparoscope-assisted and endoscopic procedures, is minimally invasive and does not interfere with bowel movement and growth.
Footnotes
Disclosure Statement
No competing financial interests exist.