
Abstract
Abstract
Background:
Laparoscopic gastrectomy (LG) is being increasingly used to treat gastric cancer. However, there are still several technical disadvantages limiting its use. Robotic gastrectomy (RG) is an emerging minimally invasive technique that overcomes some of these limitations. This study compares RG with LG in the treatment of gastric cancer by performing a systematic review and meta-analysis of all published literature.
Materials and Methods:
Comparative studies published between January 1991 and April 2013 in the major databases were systematically searched. Evaluated end points were operative, postoperative, and oncological outcomes. Pooled odds ratios and weighted mean differences with 95% confidence intervals were calculated using either the fixed-effects model or random-effects model.
Results:
Nine nonrandomized comparative studies with 2495 patients were included, of which 736 procedures were robotic and 1759 were laparoscopic. RG was associated with a lower intraoperative blood loss and a shorter time to oral intake compared with LG. However, it was associated with a significantly longer operative time and shorter distal resection margin. In addition, there was no significant difference in the number of retrieved lymph nodes, proximal resection margin, rate of conversion to open surgery, overall morbidity, anastomotic leakage, anastomotic stenosis, intestinal obstruction, time to first flatus, length of hospital stay, and perioperative mortality rates between the two groups.
Conclusions:
RG is comparable to LG, with respect to safety, technical feasibility, and oncological effectiveness in the treatment of gastric cancer. However, there is a need for well-designed prospective randomized controlled studies comparing the two procedures with long-term follow-up, to inform future practice.
Introduction
G
Compared with open surgery, laparoscopic gastrectomy (LG) has been reported to be associated with smaller surgical incisions, lesser pain, earlier time to flatus, walking, and oral intake, milder morbidity, and quicker recovery with a shorter hospital.3–5 According to the guidelines of the Japanese Gastric Cancer Association, LG is a valid alternative to open surgery for early gastric cancer. 6 Since first described in the early 1990s, 7 it has been rapidly adopted in the Far East, especially in Japan and Korea, particularly for the treatment of early gastric cancers. 8 However, the use of LG in the treatment of advanced gastric cancer is open to debate and may be a reason for LG not being used routinely for such treatment worldwide. 9
To overcome some of the limitations of laparoscopic surgery, robotic surgery has emerged as a newer minimally invasive technique. 10 Following the first robot-assisted surgery for a cholecystectomy, this technique has been applied to various surgeries. 11 The first successful robotic gastrectomy (RG) for gastric cancer was reported by Hashizume and Sugimachi 12 in 2003. This was followed by a few small series that showed relatively good short-term results for RG, which were comparable to those obtained with laparoscopic or conventional open surgery in the treatment of patients with gastric cancer in experienced centers.13–18 Robotic surgery offers the surgeon the benefit of superior three-dimensional visualization of the operating field, tremble-filtered control of the four robotic arms, and an EndoWrist® (Intuitive Surgical, Inc., Sunnyvale, CA) function that allows seven degrees of freedom mimicking the movements and dexterity of the human wrist and hand.11,19 These features minimize surgical trauma and facilitate precision control of intraabdominal bleeding during technically challenging tasks such as lymph node dissection, intracorporeal anastomosis, and the application of ligatures in a closed cavity.13,20 Robotic surgery also enables the utilization of the expertise of a specialized surgeon to complete the operation in a place away from the patient.
As a result of its numerous advantages over conventional laparoscopic surgery, robotic surgery for gastric cancer is rapidly gaining in popularity. 21 However, experience in RG is limited, and few studies have demonstrated the technical feasibility, effectiveness, and safety of RG based on analyses of clinical outcomes. We sought to compare RG with LG in the treatment of gastric cancer, with respect to short-term clinical outcomes, by performing a systematic review and meta-analysis of all published literature.
Materials and Methods
Literature search
A comprehensive literature search in Medline (PubMed), Embase, Science Citation Index Expanded, and the Cochrane Central Register of Controlled Trials (CENTRAL) in The Cochrane Library between January 1991 and April 2013 was carried out for comparing LG and RG in patients with gastric cancer. The following search terms were used: “robot-assisted,” “robotic,” “robotic-assisted gastrectomy,” “robotic gastrectomy,” “laparoscopic,” “laparoscopic-assisted gastrectomy,” “laparoscopic gastrectomy,” “minimally invasive surgery,” and “gastric cancer.” Reference lists of selected articles were also examined to find relevant studies that were not identified in the database searches. Investigators and experts in the field of gastrointestinal surgery were contacted to ensure that all relevant studies were identified. Only comparative clinical trials with full-text descriptions were included. Final inclusion of articles was determined by consensus (C.L.T. and Q.M.N.); when this failed, a third author adjudicated (J.J.X.).
Inclusion criteria
Studies included the following: (1) English language articles published in peer-reviewed journals; (2) human studies; (3) studies with at least one of the outcomes mentioned; (4) clear documentation of the operative techniques as “laparoscopic” or “robotic”; and (5) where multiple studies came from the same institute and/or authors, either the higher-quality study or the more recent publication was included in the analysis.
Exclusion criteria
Excluded studies were as follows: (1) abstracts, letters, editorials, expert opinions, case reports, reviews, and studies lacking control groups; (2) studies for benign lesions and gastrointestinal stromal tumor; (3) studies comparing two robotic systems; (4) studies only comparing open and robot-assisted gastrectomy; and (5) repeated reports between authors, centers, and patient community.
Outcomes of interests
Operative outcomes included operative time, intraoperative blood loss, and conversion to open surgery. Postoperative outcomes comprised morbidity, anastomotic leakage, anastomotic stenosis, intestinal obstruction, time to oral intake, time to first flatus, mortality, and hospital stay. Oncological outcomes included number of retrieved lymph nodes and proximal and distal resection margins.
Data extraction and quality assessment
Data were extracted by two independent observers (Y.H.C. and N.W.K.) using standardized forms. The recorded data included patient and study characteristics, perioperative outcomes, postoperative outcomes, and oncological outcomes.
The quality of studies was assessed using the modified Newcastle–Ottawa Scale with changes made to reflect the needs of this study.22,23 The maximum number of stars in the selection, comparability, and outcome categories were 3, 4, and 2, respectively. Studies achieving 6 or more stars were considered to be of a high quality. 24
Statistical analysis
Meta-analysis was performed by using Review Manager version 5.0 software (The Cochrane Collaboration, Oxford, United Kingdom). For continuous variables, treatment effects were expressed as weighted mean difference (WMD) with corresponding 95% confidence interval (CI). For categorical variables, treatment effects were expressed as odds ratio (OR) with corresponding 95% CI. Heterogeneity was evaluated using the chi-squared test, and a value of P<0.1 was considered significant. 25 The fixed-effects model was initially calculated for all outcomes, 26 but if the test rejected the assumption of homogeneity of studies, then the random-effects analysis was performed. 27 Sensitivity analyses were performed by removing individual studies from the dataset and analyzing the effect on the overall results to identify sources of significant heterogeneity. Subgroup analyses were also undertaken by including high-quality studies to present cumulative evidence. Funnel plots based on the overall morbidity were constructed to evaluate potential publication bias. 28
Results
Description of included trials in the meta-analysis
The search strategy generated 74 relevant clinical studies, among which 15 full text articles were identified for investigating details.2,13–18,29–36 Of these, six studies2,13,29–31,36 were excluded for various reasons: one study 29 only compared two robotic systems, one study 30 only compared open with robot-assisted gastrectomy, and four repeated reports.2,13,31,36 Finally, nine studies14–18,32–35 were identified for inclusion, out of which one was a prospective nonrandomized study 17 and the rest were retrospective studies. Figure 1 shows the process of selecting comparative studies included in our meta-analysis.
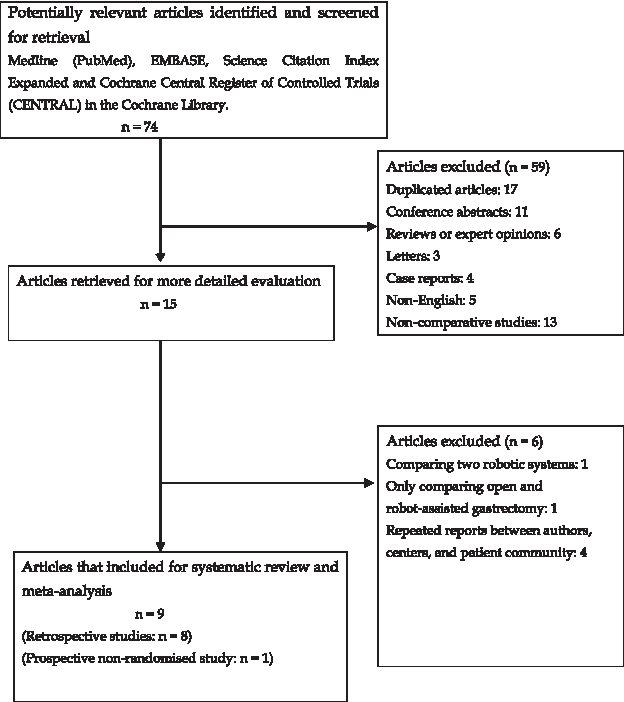
Flow diagram depicting the process of identification and inclusion of selected studies.
Study and patient characteristics
In total, 2495 patients, 736 patients from the RG group and 1759 patients from the LG group, were included in the study. All the included studies comprised patients with early and advanced gastric cancer. Operative procedures included subtotal gastrectomy in four studies,14,15,17,32 total gastrectomy in one study, 18 and a mixture of the two in the remaining studies.16,33–35 D2 lymph node dissection was performed in most studies.14–16,18,32,34,35 The study characteristics (Table 1), quality assessment scoring (Table 2), and perioperative outcomes (Table 3) of the included studies and the results of the meta-analysis (Table 4) have been summarized appropriately.
Stage 0/I/II/III.
Median (range).
Stage Ia.
AGC, advanced gastric cancer; BMI, body mass index; EGC, early gastric cancer; F, female; LG, laparoscopic gastrectomy; LND, lymph node dissection; M, male; NA, not available; PNR, prospective nonrandomized; Retro, retrospective; RG, robotic gastrectomy; SD, standard deviation.
Scoring is based on the Newcastle–Ottowa Scale with a maximum of 3 stars for selection, 4 stars for comparability, and two stars for outcome.
Comparability variables are (1) age, (2) sex, (3) body mass index, (4) comorbidity, (5) tumor stage, (6) tumor location, and (7) tumor size. Groups were assessed as comparable for variables 1–3 or 4–7 (if yes, two stars; one star if one of these three characteristics was not reported even if there were no other differences between the two groups and other characteristics had been controlled; no points were assigned if the two groups differed).
Data are mean±standard deviation values unless indicated otherwise.
Median or median (range).
AL, anastomosis leakage; AS, anastomosis stenosis; IO, intestinal obstruction; LG, laparoscopic gastrectomy; NA, not available; RG, robotic gastrectomy.
CI, confidence interval; HG, heterogeneity; OR, odds ratio; WMD, weighted mean difference.
Operative outcomes
“Operation time” was reported in all studies; however, data from only seven studies14–16,18,32–34 could be used to obtain a mean and standard deviation. The analysis included 2242 patients and showed that the RG group had a significantly longer operation time compared with the LG group (WMD=48.64 minutes; 95% CI 29.79, 67.50 minutes; P<.0001), albeit with a significant heterogeneity (I 2 =87%). Similarly, data from only six studies14–16,32–34 were pooled together to obtain the mean intraoperative blood loss in the two groups. RG was found to be associated with a significantly lower intraoperative blood loss compared with LG (WMD=−33.56 mL; 95% CI −59.82, −7.30 mL; P=.01), with a significant heterogeneity (I 2 =93%). However, as blood transfusion was reported by only one study, 32 this important outcome was not compared. Six studies14–17,32–34 reported “conversion” to an open procedure. This was described in three studies in the LG group and two studies in the RG group. There was no significant difference in the rate of conversion between the two groups (OR=2.14; 95% CI 0.32, 14.14; P=.43). Forest plots for operative outcomes are depicted in Figure 2.

Forest plots illustrating results of operative outcomes in the form of meta-analysis comparing robotic gastrectomy (RG) with laparoscopic gastrectomy (LG):
Postoperative outcomes
All the studies reported overall morbidity; however, there was no difference in this outcome between the two groups (OR=1.13; 95% CI 0.86, 1.47; P=.38). Also, there was no difference in the rate of anastomotic leakage (OR=1.06; 95% CI 0.60, 1.89; P=.83), anastomotic stenosis (OR=0.67; 95% CI 0.18, 2.50; P=.55), intestinal obstruction (OR=1.04; 95% CI 0.43, 2.53; P=.92), time to first flatus (WMD=−0.44 days; 95% CI −1.15, 0.27 days; P=.22), mortality (OR=1.66; 95% CI 0.44, 6.24; P=.45), and hospital stay (WMD=−1.16 days; 95% CI −2.42, 0.10 days; P=.07) between the two techniques. However, a pooled analysis of three studies14,32,33 suggests that patients in the RG group had a significantly shorter time to oral intake compared with the LG group (WMD=−0.28 days; 95% CI −0.46, −0.09 days; P=.004). Forest plots for postoperative outcomes are depicted in Figure 3.
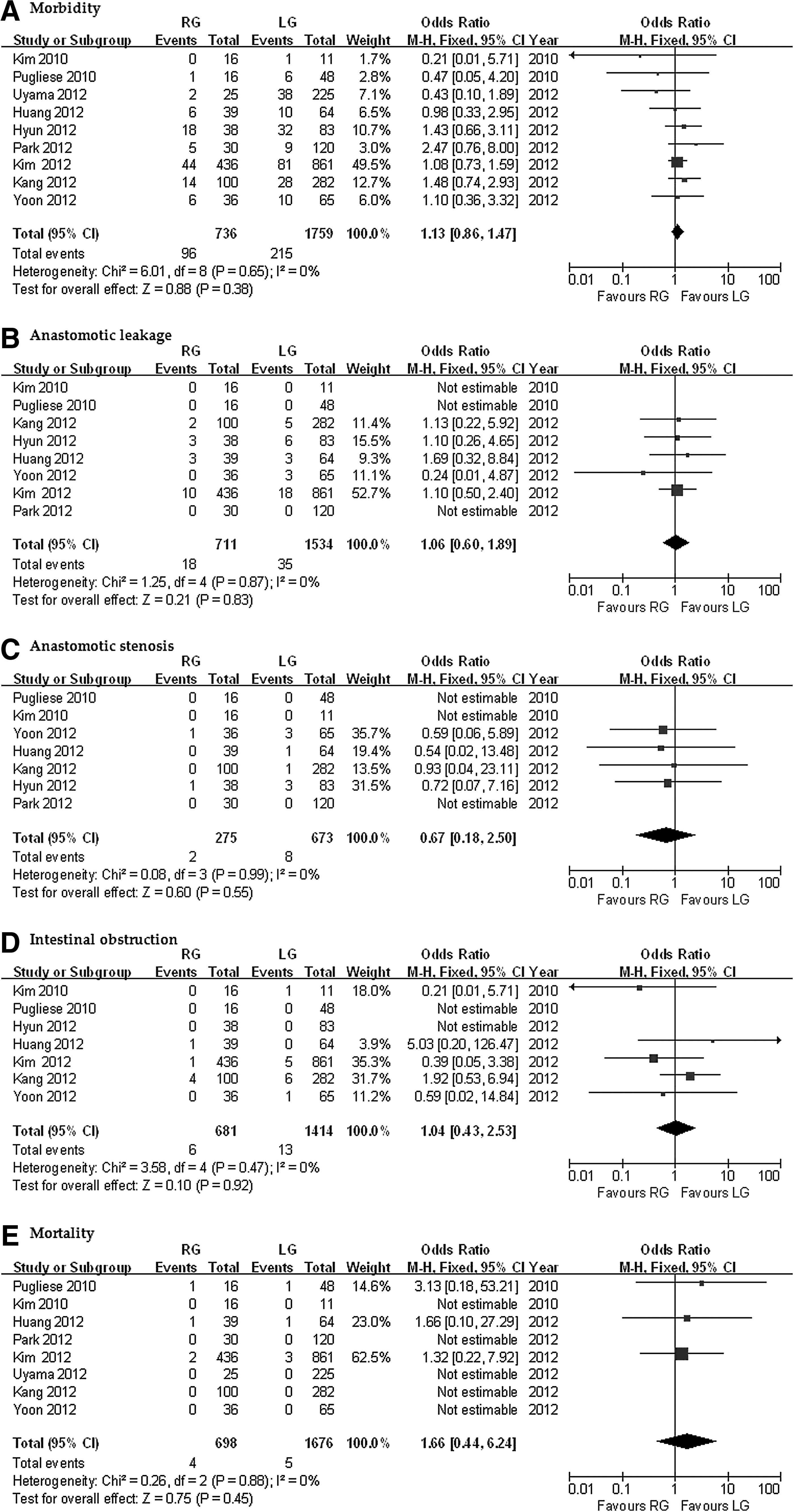
Forest plots illustrating results of postoperative outcomes in the form of meta-analysis comparing robotic gastrectomy (RG) with laparoscopic gastrectomy (LG):
Oncological outcomes
Of the eight studies that reported the number of retrieved lymph nodes, data from only seven studies14–16,18,32,33,35 could be extracted; the analysis included a total of 1963 patients with no significant difference in the number of retrieved lymph nodes (WMD=1.28; 95% CI −2.19, 4.76; P=.47) and a significant heterogeneity in the result (I 2 =78%). There was also no significant difference in the proximal resection margins (WMD=0.11; 95% CI −0.16, 0.39; P=.42) between the two groups when data from three studies16,18,33 were pooled. However, pooled data from the same three studies suggested that the RG group had a significantly shorter distal resection margin (WMD=1.13; 95% CI 0.67, 1.60; P<.00001). Forest plots for oncological outcomes have been included in Figure 4.

Forest plots illustrating results of oncologic outcomes in the form of meta-analysis comparing robotic gastrectomy (RG) with laparoscopic gastrectomy (LG):
Sensitivity and subgroup analysis
Sensitivity analyses were performed by removing individual studies from the data and analyzing the effect on the overall results to identify sources of significant heterogeneity. These exclusions did not alter the results obtained from the cumulative analyses. Subgroup analyses were undertaken for all outcome measures by including only high-quality studies. Analysis of the high-quality studies showed that there was no significant difference in operation time (WMD=38.29 minutes; 95% CI −2.36, 78.93 minutes; P=.06) and distal resection margin (WMD=0.55; 95% CI −0.92, 2.01; P=.46) between the RG and LG groups. However, other outcomes did not change. These are summarized in Table 4.
Publication bias
The funnel plot based on the overall morbidity is shown in Figure 5. There was no broad evidence of publication bias as the lay of none of the studies is shown as outside the 95% CI limits. However, there was a somewhat asymmetric distribution around the vertical axis with an absence of smaller studies favoring LG.

Funnel plot of overall morbidity in all included observational clinical studies. OR, odds ratio.
Discussion
Minimally invasive approaches including LG and RG are gaining increasing acceptance in the treatment of gastric cancer. However, clinical reports on RG and well-designed studies comparing RG and LG are scarce. We compared the short-term clinical outcomes of LG and RG through a meta-analysis. Our study showed that RG was associated with a lower blood loss, a shorter time to oral intake, and a longer operation time compared with LG for gastric cancer. Oncologic outcomes, postoperative complications, time to first flatus, and hospital stay were comparable in both groups.
Robotic surgery has been previously shown to be associated with a prolonged operation time for complex invasive procedures compared with laparoscopic surgery.37,38 Similarly, in our study, the pooled analysis indicated that the operation time was significantly longer in the RG group compared with the LG group. There may be a few reasons for this. First, the learning curve for RG affects the operation time. Once surgeons gained sufficient experience, the stabilized operation time was shorter. 13 Also, the learning curve for robotic surgery has been shown to be shorter than in laparoscopic surgery.35,39,40 This has important implications in training of surgeons and the propagation of robotic surgery as a routine minimally invasive technique. Once the learning curve for RG is overcome and surgeons become proficient in RG, there is unlikely to be a significant difference in the operation times between the RG and LG. 36 Second, the docking time in robotic surgery may contribute to the longer operation time. The operation time in robotic surgery is divided into the “docking time” to connect the robotic cart and trocars, the “console time” for robotic surgery, and the “assisted time” for the post-robotic period.19,41,42 However, once surgeons become more proficient in RG, docking time may be shortened. 43
Our review has shown that RG was associated with a lower blood loss and a significantly shorter time to oral intake compared with LG. Regarding intraoperative blood loss, some studies showed no difference between robotic and laparoscopic surgery, whereas others found that blood loss was lower in RG in the hands of experienced surgeons. 13 Blood loss in minimally invasive gastrectomy occurs mainly during lymph node dissection and is caused by microvascular damage. The limits of motion and sight in LG make bleeding more likely, especially during the dissection of lymph nodes 6, 14, 7, 8, and 9. 15 The EndoWrist, tremor filtration, and three-dimensional visualization of the operating field in RG contribute to the performance of more precise surgery and lymph node dissection with less bleeding.15,35 Moreover, in robotic surgery, steady pressure can be applied to the bleeding site with the robotic arms fixed in position; this frees the surgeon and assistant. 41 It would be relevant to bear in mind that although the difference in blood loss of 33.56 mL in our study was statistically significant, this volume is clinically insignificant. Robotic surgery may have significant merits in reducing operative stress with patients ambulating earlier, feeling less postoperative pain, gastrointestinal motility returning earlier, and being discharged from hospital earlier.15,36 In our study, we were not able to validate some of these outcomes. In our pooled analysis, there was no significant difference in time to first flatus (gastrointestinal motility) and hospital stay, although the time to oral intake was shorter in the RG group. This would suggest a near equivalence between RG and LG in reducing operative stress.
Analysis of the pooled data of the included studies revealed that there was no significant difference in the conversion rate to open surgery between the two groups. There was no significant difference in overall morbidity and mortality. It is important that there was no difference in the occurrence of anastomotic leakage, anastomotic stenosis, and intestinal obstruction. This may be attributed to the use of staplers 44 and the advances in surgical anastomotic technology. 45 These results indicate that the RG and LG are both safe surgical procedures. In gastric cancer surgery, oncologic outcome is particularly important. Analysis of the pooled data revealed that the number of harvested lymph nodes did not differ significantly between the two groups in the meta-analysis. LG had longer distal resection margin compared with RG. However, there was no significant difference in the proximal resection margins between the two groups. The length of the resection margins depends on the location of the tumor. 13 It is still too early to evaluate the long-term oncologic efficacy of robotic surgery in terms of recurrence and survival. To date, there is only one published article reporting intermediate survival. 14
Currently, total and subtotal gastrectomies with D2 lymph node dissection are recommended for most resectable gastric cancers. 46 Laparoscopic gastric surgery is limited to Stage IA and Stage IB as there are some limitations to laparoscopic lymphadenectomy compared with conventional open surgery.6,47 An adequate D2 lymph node dissection in LG is hard to accomplish without the possibility of injury to the splenic vessels, spleen, and pancreas.48–50 Laparoscopic dissection of the lymph nodes around the superior mesenteric vein, celiac axis, and splenic artery is the most frequent source of intraoperative bleeding because of the anatomic complexity of the vascular structures, the limited range of instrument movement, unintentional tremor, and poor field of vision.51,52 Laparoscopic treatment of advanced gastric cancer is limited to only a few centers because of concerns about oncologic adequacy and technical complexity of laparoscopic procedures. 53 Thus, although LG for cancer is a safe and feasible technique, there is insufficient evidence to prove its oncologic equivalence to open surgery, and it cannot be recommended as a routine approach for all gastric cancer patients.
In contrast, some of the technical advantages that robotic surgery offers such as the steady three-dimensional magnified view, tremor filtering, and fine robotic arm would facilitate an adequate D2 lymph node dissection around the portal vein, common hepatic artery, celiac trunk, and splenic artery with less blood loss.49,54 Robotic surgery may present simpler way of expanding the indications of minimally invasive surgery so as to include the advanced gastric cancer.49,55 As the use of robotic surgery becomes more widespread and surgeons become more proficient, this may become a reality. Our study has shown that RG with lymphadenectomy for treatment of gastric cancer is safe and technically feasible with oncologic outcomes comparable to those of laparoscopic surgery and a lower intraoperative blood loss. However, wider acceptance of RG as an alternative to the laparoscopic approach for gastric cancer will remain a contentious issue as there is little high-level evidence based at the moment on long-term outcome and oncologic outcome of RG as a treatment for cancer.
We acknowledge some of the limitations of our study. All the included studies were nonrandomized, mainly because of a lack of availability of randomized studies. There may be a selection bias for outcomes because early experience with robotic surgery usually involved younger, healthier, and lower-stage patients. It was also not possible to match all patient groups for tumor grade, stage, and adjuvant treatment, all of which are known to affect outcome for patients with gastric cancer. Also, a significant heterogeneity was observed between the included studies with regard to the operative time, intraoperative blood loss, hospital stay, and lymph nodes harvested. These could be explained by several factors such as different surgeon skill levels, different gastric resections, different style of reconstruction, different extent of lymph node dissection, nonblinded assessment of outcomes, and different protocols for discharge of patients at different hospitals. When statistically significant heterogeneity was detected, we used the random-effects model to address this. In addition, when we pooled only the high-quality studies, there was no significant difference between the two groups in some outcomes such as the operation time. This is probably because once surgeons gained sufficiently experienced in RG, operation times stabilized and got shorter.
Conclusions
In conclusion, our study shows that RG is comparable to LG, in terms of safety, technical feasibility, and oncological effectiveness, in the treatment of gastric cancer. However, there is a need to undertake well-designed prospective multicenter, randomized controlled studies with long-term follow-up, to investigate these two procedures. This would go a long way in informing future practice.
Footnotes
Disclosure Statement
No competing financial interests exist.