
Abstract
Abstract
Purpose:
We aimed to evaluate a new single-operator mini-endoscope for its performance, feasibility, and safety in the management of biliary and pancreatic diseases.
Patients and Methods:
A retrospective analysis was conducted of 47 patients (19 men; mean age, 50.3 years) who underwent cholangioscopy with the Polydiagnost (Pfaffenhofen, Germany) Polyscope device via various approaches for diagnosis and treatment of biliary and pancreatic diseases between January 2011 and July 2012.
Results:
Biliary pancreatic duct endoscopy was performed through a cystic duct, common bile duct, peroral, or sinus tract approach in 21, 9, 11, and 6 patients, respectively. Thirty-two cases with bile duct stones were treated by basket extraction or complete stone fragmentation, 3 cases with tumor were treated by tissue ablation, and 4 cases with stricture were treated by stenting. Seven patients who were diagnosed with suspected stones preoperatively were excluded. No complications and morbidity associated with the use of biliary and pancreatic endoscopy was observed in this study.
Conclusions:
Cholangioscopy using the Polyscope system is a safe and effective technique for diagnosing or excluding biliary and pancreatic diseases (stone, strictures, or tumor).
Introduction
S
With developments of the technique, the SpyGlass® direct visualization system (Boston Scientific Corp., Natick, MA) was introduced in 2006, in which a dedicated miniforceps biopsy can be inserted through the working channel of the cholangioscope to obtain forceps biopsy specimens under direct vision. 2 According to recent reports, the SpyGlass system seems to overcome some of the above disadvantages and exhibits the clinical benefit for assessment of indeterminate intraductal lesions, guidance of stone therapy, and targeted tissue sampling for diagnosing biliary strictures and tumors.3–5 However, it is still necessary to perform an endoscopic sphincterotomy first in order to reach the bile duct.4,5
Recent studies have proposed a new type of cholangioscope, the Polyscope (Polydiagnost, Pfaffenhofen, Germany), a single-operator multilumen cholangioscopic catheter.6,7 The Polyscope system consists of a detachable flexible endoscope system available in a diameter of 8 Fr with separate optical, working/irrigation (3.5 Fr), illumination, and steering channels, with a deflection section 10 cm in length and with a deflection of 180°, resulting in easy access into the biliary tract. As expected, Cennamo et al. 8 have reported that the Polyscope is able to achieve bile duct cannulation without a previous endoscopic sphincterotomy and to pass through all the strictures without any previous dilation. Thus, cholangioscopy using a Polyscope is suggested to be a safe and effective procedure for diagnosing bile duct lesions.
In this study, we aimed to further evaluate the performance, feasibility, and safety of cholangioscopy using a new generation of Polyscope, with an outer diameter of 8 Fr (2.67 mm), a working channel of 3.6 Fr (1.2 mm), and a tip deflection of 270°, and using the model PD-LS-0220 xenon endoscopic light source (PolyDiagnost) as the light source (Fig. 1A–C), for management of pancreaticobiliary diseases.
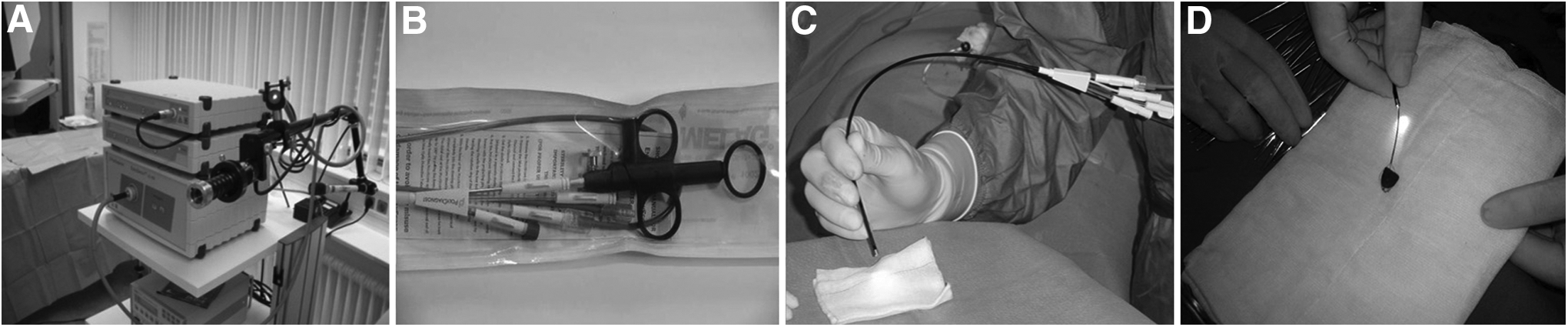
The endoscopic equipment:
Subjects and Methods
We retrospectively analyzed 47 patients (19 males, 28 females; mean age, 50.3 years) who underwent an intraductal biliary and pancreatic endoscopy for treatment and diagnosis of biliary and pancreatic diseases in our hospital. Written informed consent was obtained from all patients, and the study protocol was approved by our institutional review board. Thirty-one cases were diagnosed with intra- and extrahepatic bile duct stones by B ultrasound and imaging examination, but suspicious stones were observed in 10 cases. Preoperative examination indicated intrahepatic bile duct or duodenal papillary stricture in 4 cases and suspicious tumor in 2 cases (Table 1).
Pancreaticobiliary diseases were diagnosed and treated using the Polyscope system via the cystic duct, common bile duct, peroral, cutaneous sinus tract, or T-tube sinus tract approach. All procedures were performed by an experienced biliary endoscopist with the patients under monitored anesthesia.
Cystic duct approach
After the gallbladder was routinely resected, the cystic duct at more than 0.5 cm away from the common bile duct was pulled by the mosquito clamp and gently dilated by the hemostatic forceps. For those patients with a thinner cystic duct, a biliary bougie dilator was used. The biliary–pancreatic duct endoscope was then inserted via the cystic duct to perform bile duct exploration. First, the intrahepatic bile duct was explored upward, inserting into the hepatic ducts at three or four levels of the left and right liver to investigate stenosis, tumors, and stones (Fig. 2A). Second, the common bile duct was explored downward, observing whether there were incarcerated gallstones (Fig. 2B), stenosis, and tumor in the duodenal papilla. Basket extraction or complete stone fragmentation was performed according to the intraoperative stone size, followed by washing. After the stones were removed, the cystic duct was sutured at 0.3–0.5 cm away from the common bile duct. If a hyperplastic polyp or tumor was detected intraoperatively, biopsy forceps were used to obtain tissues from the lesion.
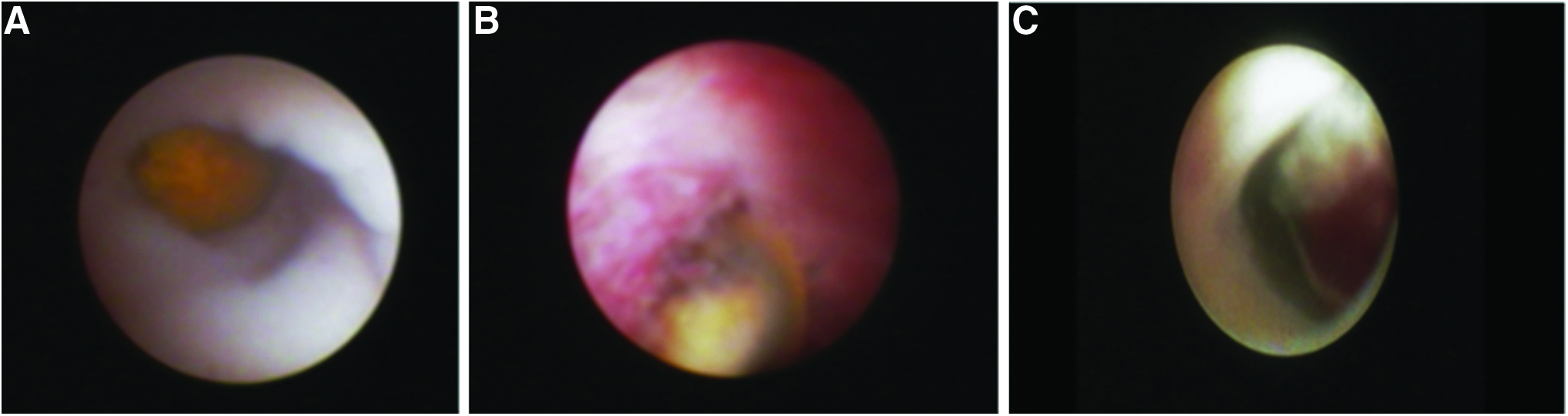
Endoscopic imaging of bile duct diseases:
Common bile duct approach
Common bile duct exploration was carried out for intrahepatic bile duct disease combined with common bile duct stones because the stone is larger and would be processed with difficulty through the cystic duct. Conventional choledochoscopic exploration was done first and then biliary–pancreatic duct endoscopy to prevent the endoscopy from being blocked in the hepatic duct at the second level because of the thicker mirror body. Stenosis, occupying lesions (Fig. 2C), and stones were explored in the biliary ducts at three or four levels of the left and right liver, the distal common bile duct, and the duodenal papilla.
Peroral approach
After ERCP was performed via duodenal endoscopy, the biliary–pancreatic duct endoscopy was placed under the guidance of the guide wire followed by adjusting the angle of the biliary–pancreatic duct endoscope to locate the visual field in the middle of the lumen. Intra- and extrahepatic bile ducts and pancreatic ducts were then explored comprehensively. This approach can directly visualize those biliary and pancreatic ducts lesions that are evaluated with difficulty by ERCP.
Cutaneous sinus tract (T-tube sinus tract) approach
For those patients undergoing percutaneous transhepatic cholangiography drainage (PTCD) operation for a week, the sinus tract was dilated, and then bile duct endoscopy was used to explore the interhepatic bile ducts lesions. For some patients who underwent biliary tract exploration but the indwelling T-tube was too thin, the endoscope could be inserted into the bile ducts via the T-tube sinus tract to perform exploration and to remove stones.
Results
Bile duct exploration was performed for 47 patients to diagnose inter- and extrahepatic bile duct diseases by using the Polyscope system. Among these patients, 32 cases showed bile duct stones and then were treated by basket extraction or complete stone fragmentation, 3 cases with tumor were treated by hepatolithiasis or pancreaticoduodenectomy, and 4 cases with stricture were treated by stenting. Seven patients who were diagnosed with suspected stones preoperatively were excluded, 1 patient was diagnosed with tumor, and 2 other patients were diagnosed with, respectively, chronic pancreatitis and pancreatic duct dilatation and liver abscess. The exploration approaches included cystic duct (n=21), common bile duct (n=9), peroral (n=11), cutaneous sinus tract (n=3), and T-tube sinus tract (n=3) (Table 2). There were no complications and morbidity associated with the use of intraductal biliary and pancreatic endoscopy.
PTCD, percutaneous transhepatic cholangiography drainage.
Discussion
Although the flexible Polyscope system has been widely used at a growing number of urologic centers for the management of renal or urinary calculi,9–11 its use for management of bile duct stones, stricture, and tumor has rarely been reported. 8 In this study, we further evaluated the new generation of Polyscope, with an outer diameter of 8 Fr (2.67 mm), a working channel of 3.6 Fr (1.2 mm), and a tip deflection of 270° for diagnosis and treatment of biliary and pancreatic diseases. This Polyscope with an increased maximum angle of deflection beyond standard scope properties (>180°) secures easier access to the biliary tract. 11 The 1.2-mm (3.6 Fr) working channel allows diagnostic tissue sampling and therapeutic interventions, including electrohydraulic shock-wave lithotripsy, tissue ablation, and direct stent placement, thus reducing the additional injuries due to the stepped surgery.8,12 In addition, combined catheter structure is also able to avoid cross-infection complications and expensive maintenance costs. In our series, 47 patients underwent bile duct exploration to diagnose inter- and extrahepatic bile duct diseases by using the Polyscope system. Among them, 32 cases with bile duct stones were treated by basket extraction or complete stone fragmentation, 3 cases with tumor were treated by tissue ablation, and 4 cases with stricture were treated by stenting. Seven patients who were diagnosed with suspected stones preoperatively were excluded. No complications and morbidity associated with the use of biliary and pancreatic endoscopy were observed in this study.
It has been reported that cholangioscopy can be performed by the transcystic duct, 13 peroral, 14 common bile duct, 15 percutaneous transhepatic cholangiography drainage sinus tract, or T-tube sinus tract 16 approach to diagnose and treat biliary and pancreatic diseases. Thus, in this study, we also included the patients who underwent cholangioscopy using a Polyscope system with different approaches. Considering the specific anatomical feature in the cystic duct, a spiral mucosal valve (Heister's valve) 17 that tends to block the passage of a gallstone and affects the insertion of endoscope into the intra- and extrahepatic bile duct, we pulled the cystic duct at 0.5 cm away from the common bile duct using the mosquito clamp and then gently dilated the cystic duct with hemostatic forceps. A biliary bougie dilator was used if necessary. These measures promote smooth insertion of the biliary–pancreatic duct endoscope. The transcystic duct can clear the gallbladder stone and common bile duct calculi for once without the placement of the T-tube drain. Peroral and duodenal endoscopy may be also an important supplement and span for the duodenoscope.
In conclusion, our results show that cholangioscopy using a Polyscope system is a safe and effective technique for diagnosing or excluding biliary and pancreatic diseases (stone, strictures, or tumor). Further refinements in the visual field, the position, and/or the orientation of the tool may be more beneficial to its application in the clinic.
Footnotes
Acknowledgments
This study was supported by Pudong Hospital Scientific Research Project number 201104.
Disclosure Statement
No competing financial interests exist.