
Abstract
Abstract
Background:
Laparoscopic liver resection (LLR) is proposed as an alternative to open liver resection (OLR) for treatment of liver tumors. The aim of this study was to compare the surgical and oncological outcomes of LLR versus OLR in benign and malignant solid liver tumors.
Study Design:
In this case-matched study, charts of 497 patients with liver lesions who had LLR or OLR in our center were retrospectively reviewed. Among them, 54 consecutive patients with benign or malignant solid liver tumors who had LLR were matched with a similar number of patients with OLR based on the pathology and extent of liver resection. Additionally, the surgical and oncological outcomes such as operating room time, amount of blood transfusion requirement, free resection margin rate, length of hospital stay, complication rate, perioperative mortality, and survival were compared between the two groups.
Results:
Demographics, pathological characteristics of the tumor, and extent of liver resection were similar between the two groups. Twenty-nine (54%) patients in each group had malignant lesions. There were no statistically significant differences between the two groups in terms of operating room time, amount of blood transfusion requirement, free resection margin, or postoperative complication rate or survival. However, hospital stay was significantly shorter in the laparoscopic group (5.9 versus 9 days, P=.006). Although no perioperative mortality was observed in patients with benign tumors, among the patients with malignant tumors, 2 died perioperatively in each group.
Conclusions:
Our results in accordance with previous studies demonstrated that although the oncological outcomes of LLR and OLR were comparable, LLR patients had a shorter hospital stay.
Introduction
Subjects and Methods
Patient selection and data
This study was approved by the Institutional Review Board of Louisiana State University Health Sciences Center–Shreveport. In this case-matched study, charts of 497 patients who had liver resection (108 [22%] with LLR and 389 [78%] with OLR) at our center for malignant or benign liver tumors from 1993 to 2012 were retrospectively reviewed. Among the patients with LLR, 54 consecutive patients who had solid malignant or benign liver tumors were enrolled as cases in this study. Among the patients with OLR, 54 patients with solid malignant or benign liver tumors were matched to the LLR cases in a 1:1 fashion based on the pathology of liver tumor and then the extent of liver resection. During the matching process, the investigators were blinded to the surgical and oncological outcomes of the patients.
Patients' baseline data, including demographics, tumor pathology, number, location, and size of tumor lesions, and extent of liver resection, were extracted retrospectively from the institutional electronic patient record and operative database. The data related to surgical and oncological outcomes including operative time from incision to closure, amount of perioperative blood transfusion requirement, length of hospital stay, complication and free resection margin rates, perioperative mortality, and survival were also extracted and compared between the two groups. The free resection margin rate was calculated only for patients with malignant tumors as well as those with adenoma. Survival was calculated only for those with malignant tumors.
The Clavien–Dindo classification was used for the assessment of the severity of the complications. 9 Perioperative mortality was defined as any death, regardless of cause, occurring within 30 days after surgery whether in or out of the hospital and after 30 days during the same hospitalization subsequent to the operation. 10
Statistical analysis
Statistical analyses were performed using the SPSS Base 15 statistical software package (SPSS Inc., Chicago, IL). Continuous data were compared between the two groups using the independent-sample t test; categorical data were compared using the chi-squared or Fisher's exact test. Survival of the patients in the two groups was compared using the log rank test and Kaplan–Meier survival curves.
Results
As demonstrated in Table 1, baseline characteristics of the patients, including demographics, tumor pathology, number, location, and size of tumor lesions, and extent of liver resection, were similar between the two groups. Twenty-nine (54%) patients in each group had malignant lesions. As demonstrated in Table 2, surgical and oncological outcomes of patients in the two groups were similar except for the significantly shorter hospital stay (5.93±4.43 days versus 8.98±6.93 days [P=.006] in the LLR group compared with the OLR group. No case in the LLR group was converted to an open surgery.
Continuous data are expressed as mean±standard deviation values; categorical data are expressed as number (percentage).
CRC, colorectal carcinoma; FNH, focal nodular hyperplasia; HCC, hepatocellular carcinoma.
Continuous data are expressed as mean±standard deviation; categorical data are expressed as number (percentage).
Free resection margin rate was only calculated for patients with malignant lesions as well as those with hepatic adenoma.
CDC, Clavien–Dindo classification.
Two patients in each group died perioperatively. In the LLR group, a 58-year-old white man with hepatocellular carcinoma (HCC) and cirrhosis due to hepatitis C, uncontrolled type 1 diabetes mellitus, coronary artery disease, and hypertension underwent bisegmentectomy (segments 4 and 5) and died on postoperative Day 25 because of hepatic decompensation, encephalopathy, atrial fibrillation, pulseless electrical activity, and cardiorespiratory arrest. Moreover, in this group, an 84-year-old white man with HCC, chronic obstructive pulmonary disease, coronary artery disease, and tongue cancer underwent right lobectomy and died on postoperative Day 4 because of aspiration of gastric contents followed by cardiorespiratory arrest. In the OLR group, a 58-year-old African American man with HCC and cirrhosis underwent bisegmentectomy (segments 7 and 8) and died on postoperative Day 27 because of hepatic decompensation, encephalopathy, and cardiorespiratory arrest. Moreover, in this group a 59-year-old white man with type 2 diabetes mellitus and liver cirrhosis and HCC due to chronic alcohol abuse and hepatitis C underwent left lateral segmentectomy and was discharged on postoperative Day 5 in stable condition with no complications. The patient died on postoperative Day 11 at home; the cause of death is unknown.
As demonstrated in Figure 1, the Kaplan–Meier survival curves of patients with malignant tumors were also similar between the two groups.
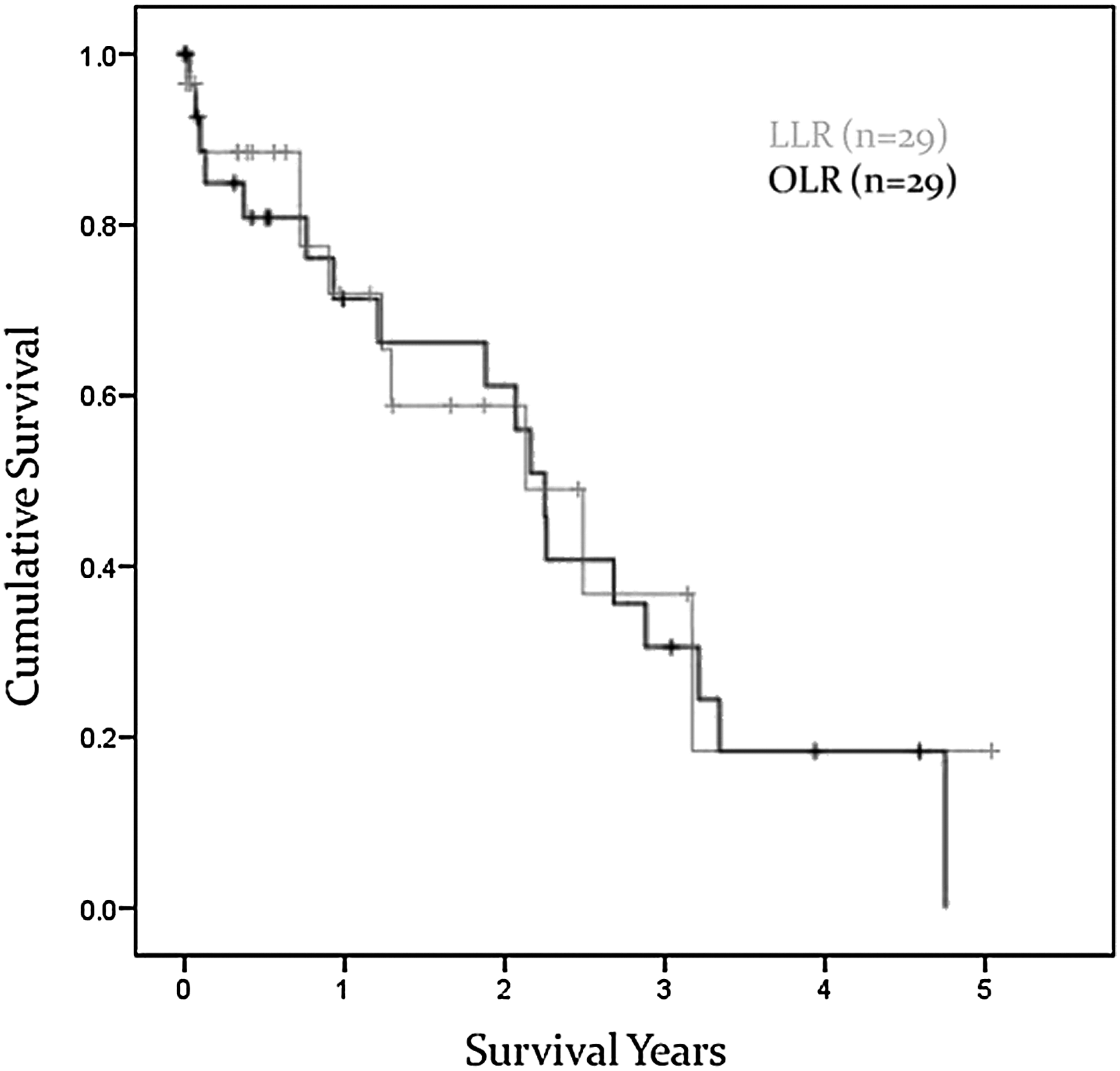
Overall survival of patients with malignant tumors in the two groups. LLR, laparoscopic liver resection; OLR, open liver resection.
Discussion
Our results demonstrate that although the duration of hospital stay was significantly shorter in patients with solid malignant or benign liver tumors who underwent LLR compared with those with OLR, other surgical and oncological outcomes were comparable between the two groups.
Short-term intraoperative and postoperative advantages of LLR have been demonstrated in several studies so far. Compared with OLR, LLR has been shown to result in shorter duration of intravenous narcotic use, hospital stay, and time to oral feeding as well as lower intraoperative blood loss.3,5,7,11–14 Moreover, postoperative complications and adverse events rates were reported to be comparable or even more favorable in LLR patients compared with OLR patients.3,5,7,11–14 Likewise, in our study, we demonstrated that LLR of solid malignant and benign liver tumors is associated with a significantly shorter hospital stay compared with OLR, although the incidence and severity of postoperative complications are similar.
Oncological safety of LLR has been always a matter of debate in the surgical community. Although initially there were concerns about the ability to achieve negative resection margin or long-term survival of patients undergoing LLR, recent studies have reported similar, if not better, oncological outcomes like rate of negative resection margin, tumor recurrence rate, or all-cause mortality with LLR compared with OLR.3,7,13,14 Similarly, our findings demonstrated that the rates of negative resection margin and all-cause mortality in the LLR and OLR groups were comparable. However, it should be noted that because of the small sample size of our study and variable chemotherapeutic regimens that our patients with malignant lesions received, type and duration of chemotherapy were not considered in comparison of all-cause mortality rates between the two groups.
The strengths of our study are the good matching of the patients with respect to tumor characteristics and the fact that all our patients had solid liver tumors, which are surgically more challenging than cystic liver lesions. On the other hand, the main limitation of our study is its retrospective design. Although our patients were matched, as in the other studies with matching, there could always be factors not accounted for in the matching process that might impact the decision on choosing the type of surgery or the surgical and oncological outcomes of the patients. 3 Therefore, the best study design to compare LLR versus OLR is a randomized controlled trial where randomization could omit the selection bias we face in the retrospective studies. 4 The small sample size and lack of long-term follow-up in some of the enrolled patients are other limitations of this study.
In conclusion, our results demonstrated that although the treatment of solid liver tumors with LLR or OLR has comparable oncological outcomes, LLR may have advantages over OLR like shorter hospital stay. The possible pros and cons of LLR versus OLR in the treatment of solid liver tumors should be further evaluated in randomized controlled trials with larger sample sizes and longer durations of follow-up.
Footnotes
Acknowledgments
The source of funding for this study is the Donnie and Gail Juneau Chair in Surgery.
Disclosure Statement
No competing financial interests exist.