
Abstract
Abstract
Background:
Aortopexy is the most effective treatment for severe tracheomalacia associated with esophageal atresia with distal tracheo-esophageal fistula (EA/TOF). In the last few years, the thoracoscopic approach has been proposed, but the number of patients treated is limited. The purpose of this study is to review our initial experience with thoracoscopic aortopexy.
Patients and Methods:
A retrospective review of medical records was performed on EA/TOF patients undergoing thoracoscopic aortopexy at the Great Ormond Street Hospital for Sick Children (London, United Kingdom) from January 2009 to May 2012. Patient demographics, indication, perioperative course, and long-term results when available were noted.
Results:
Four patients underwent a successful thoracoscopic aortopexy, with no operation being converted. No morbidity or mortality was associated with the procedure. Length of postoperative stay ranged from 2 to 4 days. All patients were relieved of their symptoms, and no recurrence was noted.
Conclusions:
Thoracoscopic aortopexy is a feasible and successful treatment for severe tracheomalacia in EA/TOF patients. The complication rate may be lower than after the open procedure and is more satisfactory in terms of cosmetic appearance. However, we need a larger and prospective study with a longer follow-up to confirm these preliminary results.
Introduction
T
Patients and Methods
After local ethics committee approval of study protocol, retrospective chart review was performed for all infants who underwent thoracoscopic aortopexy for severe tracheomalacia after EA/TOF repair between January 2009 and May 2012 at Great Ormond Street Hospital, NHS Foundation Trust (London, United Kingdom). Gender, age, weight at surgery, comorbidities, indication for procedure, perioperative course, and results to date were reviewed. The standard preoperative workup was based on a micro-laryngotracheobronchoscopy with spontaneous breathing to define the severity and extent of tracheomalacia.
In order to exclude esophageal anastomotic stricture, gastroesophageal reflux, and vascular rings, a contrast swallow was performed. The most recent outpatient visit was used to record the outcome and progress after aortopexy. We defined the success of the operation as an abolition of the presenting symptoms (pneumonia and/or acute life-threatening episode).
Operative technique
Under general anesthesia, the infant was positioned supine with the left side elevated at a 20° angle at the edge of the table. The left arm was abducted, and the elbow was flexed. A thoracoscopic 5-mm set with a 0° telescope was used, and three ports were inserted along the anterior axillary line as shown in Figure 1.
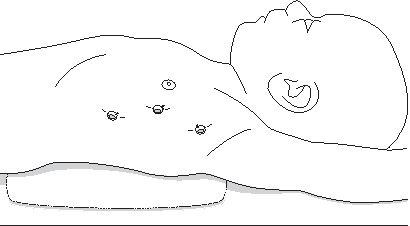
Patient in the supine position with the left side elevated at a 20° angle at the edge of the table. The left arm is turned up toward the head. Three ports are inserted on the anterior axillary line.
Insufflation was commenced in the pressure range 6–10 mm Hg with a low flow rate of 2 L/minute, adapted to the child's cardiopulmonary behavior. The left lobe of the thymus was mobilized, and the isthmus was divided to the innominate vein. The left thymus lobe was pushed to the right side of the mediastinum or resected as necessary (Fig. 2). The pericardium was then opened transversally just below its reflection on the ascending aorta. Three 3/0 polypropylene (Prolene®; Ethicon, Somerville, NJ) sutures were passed through the sternum or intercostal space through stab incisions. These sutures were then passed through the pericardial reflection, the adventitia of the ascending aorta, and then the sternum, to exit through the stab incisions (Fig. 3). These sutures were all tied while the sternum was depressed and held down. The sternum was then released (Fig. 4). The procedure was ended if the ascending aorta was hitched up close to the sternum.
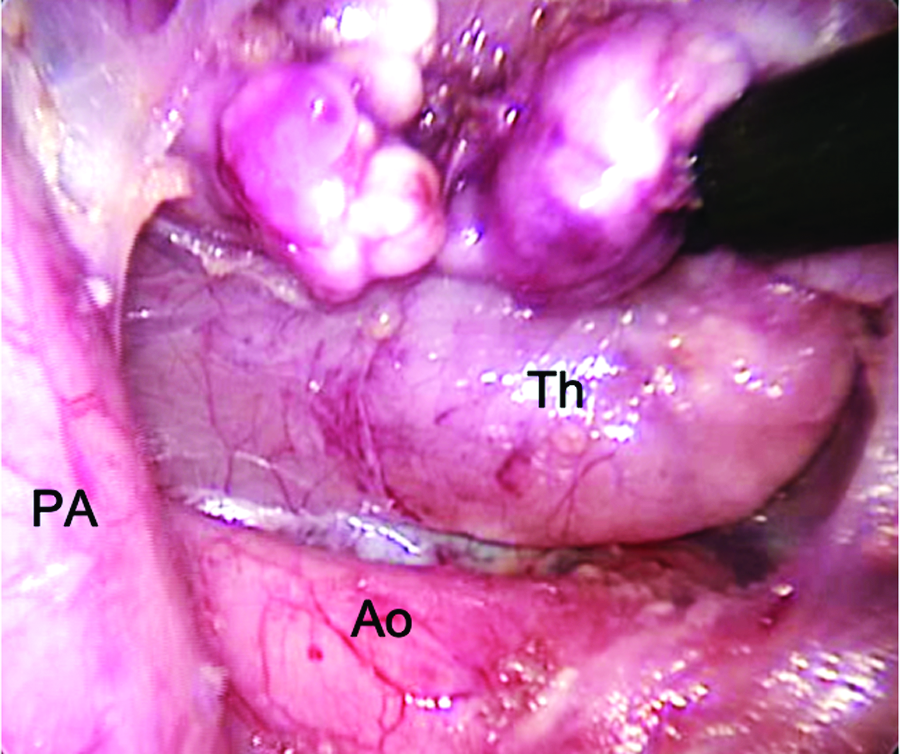
Thoracoscopic view following resection of the left thymus lobe. Ao, ascending aorta; Th, right thymus lobe; PA, pulmonary artery.
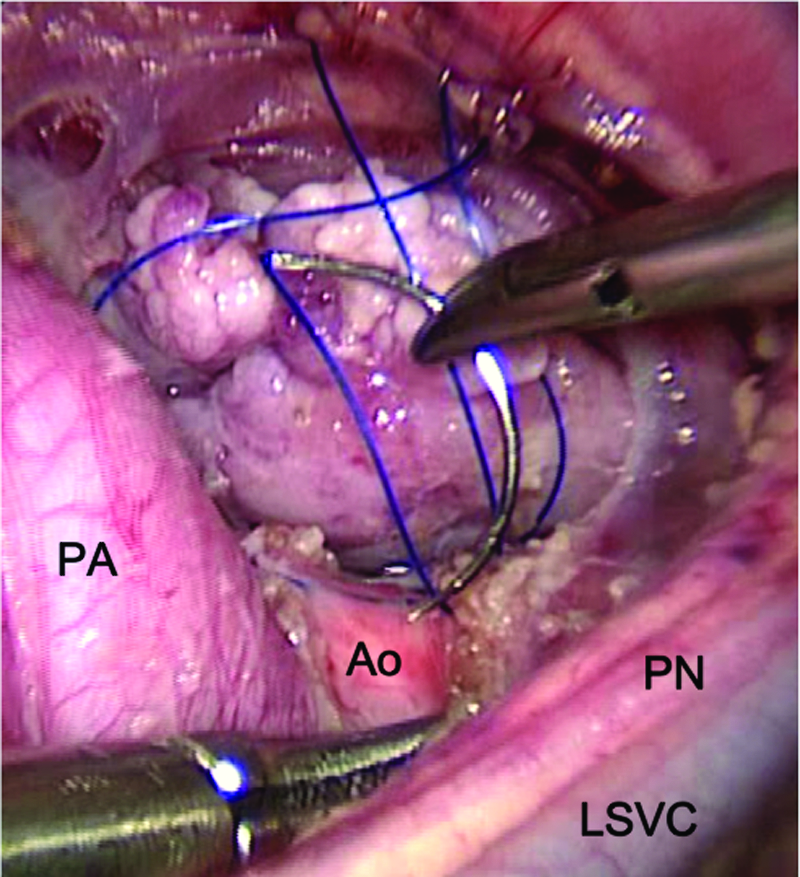
View of the second suture. Ao, ascending aorta; LSVC, left superior vena cava; PA, pulmonary artery; PN, phrenic nerve.
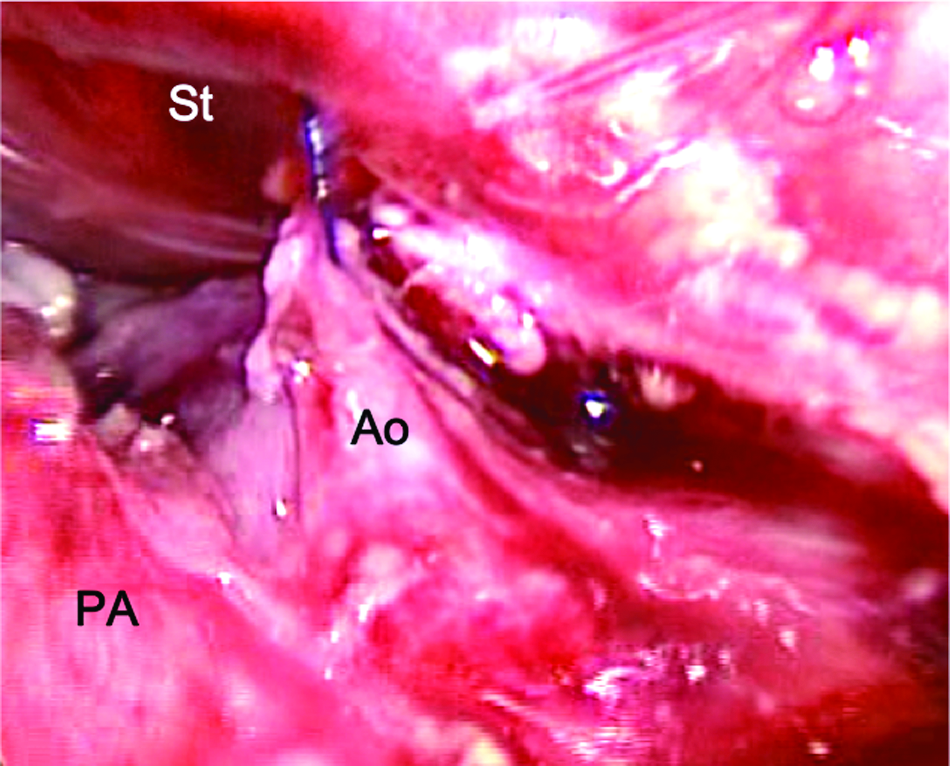
View of the ascending aorta (Ao) hitched up to the sternum (St). PA, pulmonary artery.
Intraoperative bronchoscopy was not used. Chest drains were not used. Trocar holes and stab wounds were closed with polyglactin 910 (Vicryl®; Ethicon) 5/0 sutures, and skin was closed with Indermil® (Henkel, Düsseldorf, Germany) glue.
Results
Details of the 4 patients are summarized in Table 1. There were 3 boys, with gestational age ranging from 33 to 40 weeks and birth weights ranging from 2.3 to 3.1 kg. Patients 1, 2, and 3 had on Days 1, 2, and 3, respectively, a right thoracotomy for EA/TOF repair. Patient 4 underwent thoracoscopic esophageal repair on Day 1.
Pain cover corresponds with intravenous or oral morphine medication.
ALTE, acute life-threatening episode; ED, esophageal dilatations; F, female; GA (WG), gestational age (weeks of gestation); M, male; WB, weight at birth.
All infants presented with esophageal anastomotic strictures requiring at least one dilatation before aortopexy. One patient had an anorectal malformation requiring a colostomy, followed by a posterior sagittal anorectoplasty (pull-through procedure) at the age of 7 months (Case 2). One patient presented with severe gastroesophageal reflux requiring a laparoscopic fundoplication, gastrostomy, and a Ladd's procedure for correction of malrotation (Case 1). One patient was in intensive care (Case 4) before surgery, having experienced two consecutive life-threatening episodes in 1 month. This patient also had a left superior vena cava diagnosed by echocardiography before surgery.
The indications for aortopexy were based on clinical presentation (recurrent chest infections or apparent life-threatening events) and the finding at bronchoscopy. All infants presented with severe tracheal collapse (>90%). Median age at aortopexy was 11 months (range, 3–27 months), and median weight was 8.4 kg (range, 4.9–10.9 kg). The procedure took between 95 and 150 minutes.
All aortopexies were completed thoracoscopically. No operation was converted to open. Three patients were extubated on the table, and the fourth patient (Case 4) was extubated in the intensive care unit 18 hours after surgery. The length of postoperative stay in the hospital was 2–7 days, with a morphine pain cover of 24–48 hours. All 4 patients had an uneventful recovery.
Median follow-up was 7 months (range, 2.5–38 months). All children improved dramatically: 2 patients had complete resolution of their presenting symptoms (Cases 1 and 3), 1 patient had a mild chest infection 4 months after surgery (Case 2), and 1 patient had initial dramatic improvement with resolution of stridor and blue spells (Case 4) but developed further respiratory and feeding difficulties. This child was diagnosed with a type I/II laryngeal cleft 9 weeks after aortopexy. This had not been noted on previous bronchoscopy.
Discussion
Esophageal atresia is frequently associated with tracheomalacia. 1 Symptoms include expiratory stridor, wheezing, recurrent respiratory tract infections, and apparent life-threatening episodes (dying spells, respiratory arrest) in severe cases. Tracheomalacia is an intrinsic large airway abnormality characterized by a lack of rigidity of the tracheal wall resulting in anteroposterior collapse of the tracheal wall. This leads to airway occlusion during expiration. 8
Diagnosis is usually confirmed at rigid bronchoscopy in a child breathing spontaneously, and the morphologic classification distinguishes the tracheomalacia as mild (>50%), moderate (>80%), or severe (>90%). 9
Aortopexy was first published by Gross and Neuhauser 10 in 1949, and the original operation has been modified to different open approaches: anterior mediastinal, 11 mediastinal window, 12 sternotomy, 13 right 14 or left15,16 thoracotomy, and left lateral muscle-sparing thoracotomy. 1 In an attempt to avoid the trauma and scarring of thoracotomy, DeCou et al. 17 described thoracoscopic aortopexy in 2001. This technique was then modified by Shaarschmidt et al. 2 in 2002 with 2 patients.
Aortopexy is one of several procedures available to treat tracheomalacia. Placements of extratracheal or intratracheal stents and splint 18 have been described in the literature. However, intratracheal stents appear to be associated with a higher failure rate and a significant morbidity and mortality compared with standard aortopexy. 19 In general, aortopexy is accepted as the most effective treatment method for severe tracheomalacia, with a success rate of 85%–92%.1,15
There are no evidence-based guidelines for the treatment of tracheomalacia in children. 20 Our indications for surgery were based on severe symptoms combined with the finding of severe tracheomalacia (>90% occlusion of the trachea) on rigid bronchoscopy. In the literature, the incidence of severe tracheomalacia requiring an aortopexy in EA/TOF patients varies between 2% to 25%.16,21,22 This variable incidence reflects the different surgical practices and is not readily explained. In 1987, our group reported a 10% incidence in a series of 210 EA/TOF infants, 22 whereas more recently Dave and Currie 1 reported a 6.6% aortopexy rate in 227 patients with EA/TOF.
The optimal approach to thoracoscopic aortopexy is still debated. In the event of a previous left thoracotomy, a right-sided approach may be a solution.2,5 As most infants with esophageal atresia and tracheo-esophageal fistula will have had a right-sided operation, the left-sided approach is likely to be easier. In their series of 5 patients, Perger et al. 6 used only left thoracoscopy. All our patients had the aortopexy performed through a left-sided approach, in line with our previous experience with the open operation.
Thoracoscopic aortopexy has also been successful in older children. Durkin et al. 4 reported success in a 12-year-old boy, and other authors have described this procedure in patients between 2 weeks and 4 years of age.2,3,5,6 In our series, age at surgery was 3–27 months.
Early complications of open surgery from the literature include phrenic nerve palsy, pericardial/pleural effusion, lung collapse/consolidation, pneumonia, chylothorax, thymic engorgement and compression, chest wall deformities or scoliosis, vocal cord palsy, aortic tears, and death.1,23 In the largest published series of open aortopexy (105 patients, including 44 patients with tracheo-esophageal fistula), we observed an 18% complication rate overall (16% for the tracheo-esophageal group). 23 In this series, there were no postoperative complications.
The thoracoscopic approach may allow for early extubation, whereas open surgery may require a stay in the intensive care unit (0 median intensive care unit day in the series of Calkoen et al. 23 to 1.9 days in the series of Dave and Currie 1 ). Moreover, pain experienced after a thoracoscopic procedure might be less than after open surgery even if the muscle-sparing technique has been used. In our series, pain relief (i.e., use of morphine) was less than 48 hours. A major factor in the shorter pain relief may be linked to the absence of a chest drain, which has now been shown to be unnecessary after thoracoscopy in children. 24 None of our patients had a chest drain after surgery and did not require one postoperatively, but this was also our experience with the open operation. A shortened postoperative length of stay may also be an important benefit of the thoracoscopic approach. In our series it ranged between 2 to 7 days. Perger et al. 6 described a full respiratory recovery achieved within 14 days in their 5 patients.
Recurrence of an acute life-threatening episode is described in the largest published series of thoracoscopic aortopexy. 3 The two described recurrent acute life-threatening episode cases required a redo procedure. One of our patients had a further respiratory event and was found to have a laryngeal cleft. The other 3 patients remained symptom free. Perger et al. 6 described recurrent chest infection in 3 patients in their series of 5. One of our patients had a mild chest infection 4 months after surgery.
Lastly, cosmesis is much improved with the thoracoscopic approach, leaving three minimal incisions below the left arm and small stab incisions anteriorly, whereas open surgery leaves an anterior transverse thoracotomy or median sternotomy scar.
Although our results are encouraging, this series remains a single-center retrospective study on a small amount of patients. Furthermore, a longer follow-up is required to assess the ongoing effect on the airways. A multicenter prospective study may be required to confirm the advantages related to the use of minimally invasive technique for aortopexy.
In conclusion, thoracoscopic aortopexy is a feasible, safe, and successful operation to treat severe tracheomalacia in patients after EA/TOF repair. Considering the good preliminary results of the thoracoscopic approach, this procedure should be considered early in the treatment of all patients with severe tracheomalacia, in centers where advanced minimally invasive procedures are available.
Footnotes
Disclosure Statement
No competing financial interests exist.