
Abstract
Abstract
Purpose:
The instrument crowding derived from commercially available access devices in single-incision laparoscopic surgery (SILS) is a challenge to overcome. This study was designed to evaluate the short-term surgical outcomes of SILS by applying a self-made device in patients with benign colon diseases.
Patients and Methods:
We collected and reviewed the medical records of patients who received SILC by using a self-made glove-port system from March 2007 to July 2012. All operations were performed by a single surgeon. Sixty-four patients (36 males and 28 females) were enrolled for this study. Among them, 15 patients received right-side colon resection, 31 patients received left-side colon resection, and 18 patients received total colectomy.
Results:
In the analysis of medical records from these groups of patients, we found that there was no significant difference of gender, body mass index, tumor size, incision length, and blood loss among these three groups. Furthermore, no significant difference of the pain scores, average length of hospital stay, and average duration of bowel return was observed among these three groups. However, it was notable that younger age, longer duration of operation, and longer bowel resection were indeed significantly found in the patients undergoing total colectomy. On the other hand, curved instruments were used in 5 (16.1%) of 31 patients with left-side colon resection.
Conclusions:
A simple self-made glove-port device was proven as a practical method of SILS for colorectal diseases. These findings suggested that single-incision laparoscopic total colectomy provides compatible clinical outcome in the patients with benign colon diseases compared with the other two surgical procedures used in this study.
Introduction
In colorectal diseases, conventional laparoscopic surgery raises fewer complications compared with other conventional surgeries.5,6 Moreover, laparoscopic colectomy brings faster recovery and less cost expenses in patients ranked as American Society of Anesthesiology class 3 and 4 compared with open colectomy. 7 Single-incision laparoscopic colectomy (SILC), one of the types of SILS, has effectively developed to treat benign and malignant colorectal diseases because it has the innovations of new access devices, instruments, and surgical techniques. 8 Therefore, SILC appears to be feasible and safe when performed by surgeons who are highly skilled in laparoscopy. Despite technical difficulties, there may be some potential benefits brought by SILC over conventional laparoscopic colectomy.9,10
In SILS, a single incision is typically made at the umbilicus, and specifically developed access devices are used for the introduction of trocars and instruments. 11 In most cases, no other abdominal wounds are required, and the umbilical incision, although larger than that from conventional laparoscopy, is minimally visible once healed. Accumulating evidence indicates the feasibility and safety of SILS for gastrointestinal, colorectal, and bariatric surgery.12–17 Despite these encouraging reports, challenges remain in SILS. Most commercially available access devices are rigid and have only one access point, which may hamper dissection due to its instrument crowding. 11 In addition, the instruments are parallel to each other, which in turn not only limits the performer's operation movement, but also further increases the difficulties of tissue manipulation and dissection. To overcome these obstacles, specially designed curved instruments are developed and further used. However, the cost expense of these curved instruments is very high. Here, we have developed another simple glove-port device10,18,19 by using a commercially available wound protector and a surgical glove, which may both improve the feasibility of SILS and decrease the cost expense. The goal of this study was to evaluate whether our self-made access device for SILS could be generally applied in benign colon diseases with different surgical procedures, including right-side colon resection, left-side colon resection, and total colectomy.
Subjects and Methods
Sample collection
After approval of the Institutional Review Board was received, this study was conducted to collect medical records retrospectively of the patients with benign colon diseases undergoing SILS by using a self-made glove-port system from March 2007 to July 2012 at our institution. We collected and analyzed the demographic, intraoperative, and postoperative data, including age, gender, body mass index, measurable tumor size, incision length, length of bowel resection, estimated blood loss, use of a curved instrument, duration of operation, drain placement, pain score, hospital stay, bowel return, and use of an extra port.
Self-made glove-port system
SILC procedures were performed with a self-made glove-port system. In brief, the system was constructed by connecting a commercial wound protector (ALEXIS® wound retractor system; Applied Medical, Rancho Santa Margarita, CA) to a surgical glove. Trocars (e.g., 5 mm, 10 mm, and 15 mm) were then introduced through the little finger, thumb, and middle finger of the glove, respectively (Fig. 1). The double-ring design of the wound protector allows not only the wound protector and surgical glove to be connected tightly, but also the glove to roll completely around the wound protector without air leakage. The device allows a larger range of movement, better wound protection, and more feasibility of direction change at any time. Furthermore, it is suitable for all body types.

Illustrations of the self-made single-port system.
Surgical procedures
Under general anesthesia, patients were placed in the lithotomy or supine position. Brief diagrammatic representations of the equipment relative to the surgeon are shown in Figure 2. An incision of 2.5–3 cm was made at the umbilicus or McBurney's point. If the lesion was located above the rectosigmoid junction, an umbilical incision was made; if the lesion was located below the rectosigmoid junction, a McBurney incision was made. Then, for SILC, the self-made glove-port system with the wound protector was placed, and a CO2 pneumoperitoneum was produced with a maximal pressure of 12 mm Hg. A laparoscope with an angle of 30° and 10 mm in diameter was used for all patients. A medial to lateral approach was used for all procedures. Conventional and curved laparoscopic instruments were used interchangeably. Dissection was primarily done with an electrocautery and/or a LigaSure™ instrument using the ForceTriad™ energy platform (both from Valleylab, Boulder, CO).
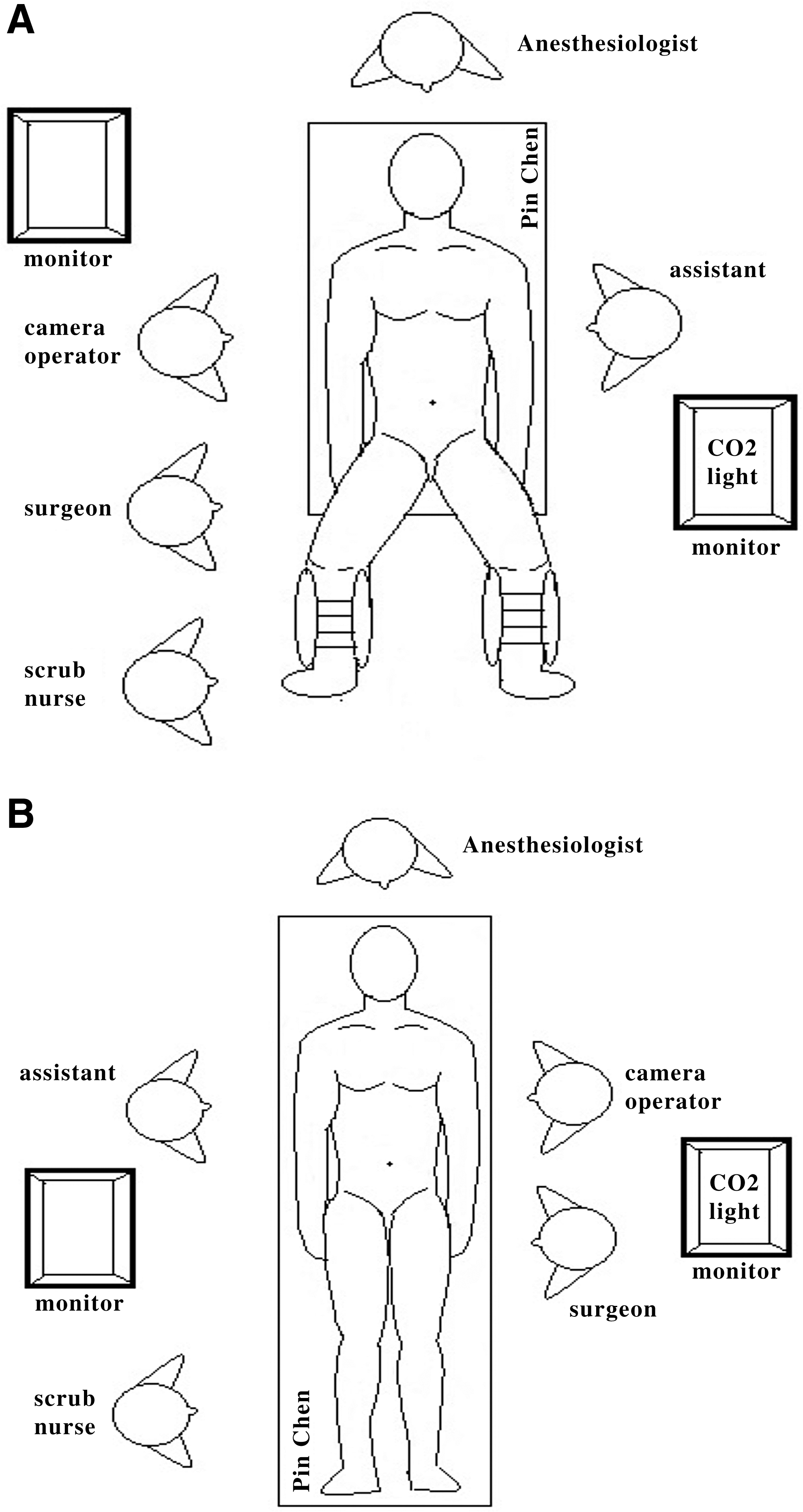
Brief diagrammatic representations of the relative position of the equipment relative to the surgeon in
For right-side resections, the ileocolic and right colic vessels and, if necessary, the middle colic vessels were identified and ligated with hemoclips. The colon was detached from the retroperitoneum, the greater omentum was freed from the colon and the terminal ileum, and the specimen was removed through the umbilical wound. A side-to-side ileotransverse anastomosis was made extracorporeally with GIA™ staplers (Ethicon Endo-Surgery, Cincinnati, OH).
For left-side resections, the inferior mesenteric vessels were identified and ligated with hemoclips. After the left colon was freed, the mesorectum was dissected before dissection of the colorectum with an Echelon Flex™ 60 Endopath® stapler (Johnson & Johnson, New Brunswick, NJ). The specimen was removed through the umbilical wound or the McBurney incision wound, and the anastomosis was made intracorporeally with a PROXIMATE® ILS intraluminal curved or straight stapler (Johnson & Johnson).
For total colectomy, the inferior mesenteric, ileocolic, and right colic vessels and, if necessary, the middle colic vessels were identified and ligated with hemoclips. After the total colon was freed, the mesorectum was dissected with a LigaSure instrument, and then the colorectum was dissected with an Echelon Flex 60 Endopath stapler. The specimen was removed through the umbilical wound, and the anastomosis was made intracorporeally with a PROXIMATE ILS intraluminal curved or straight stapler. Representative images of specimen removal and postoperative wounds are shown in Figure 3.
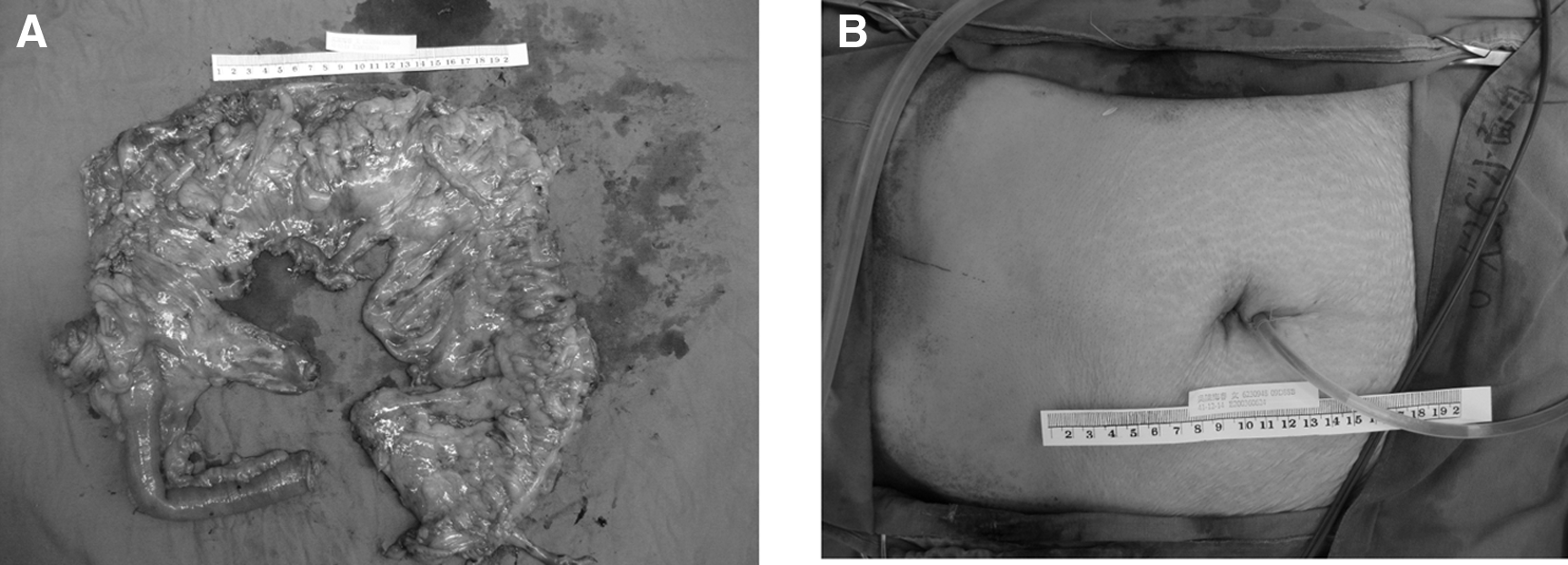
Representative images of
After the removal of the laparoscopic instruments and glove device, a Jackson–Pratt drain was placed through the incision wound if required, depending on the degree of dissection, blood loss, and presence of lymphatic or bloody discharge after completion of the procedure.
Postoperative care
All patients received standard postoperative care and pain management. Visual analog scale pain scores were recorded on the first postoperative day. Patients were asked to rank their pain on a scale of 1 (no pain) to 10 (the worst pain imaginable). If drains were placed, they were removed when the drainage amount was <50 mL/day. Patients were kept fasting until the return of bowel function, defined as passage of flatus, and then sips of water were allowed. If this was tolerated, the diet was advanced to clear liquids followed by a soft diet. When tolerating a general diet, patients were discharged typically on postoperative Day 5–7, and they were followed up in the outpatient clinic.
Statistical analysis
Continuous data were presented as mean±standard deviation values, and categorical data were given as number (n) and percentage (%). Comparability of demographic data and clinical outcomes among these groups was tested by using the chi-squared test for categorical variables and one-way analysis of variance and post hoc analysis with Scheffé's method for continuous variables. All statistical assessments were evaluated at the .05 level of significance. Statistical analyses were performed using SPSS version 15.0 statistical software (SPSS Inc., Chicago, IL).
Results
Sixty-four patients (36 males and 28 females) were enrolled for the study. All these patients had different kinds of benign diseases, including 8 cases with diverticulosis, 42 cases with benign colon tumor, 8 cases with familial adenomatous polyposis, 5 cases with colonic inertia, and 1 case with rectal prolapse. All of them also underwent surgery for disease treatment. Among them, 15 patients received right-side colon resection, 31 patients received left-side colon resection, and 18 patients received total colectomy. Thus, these 64 patients were divided into three groups based on the type of colon resection for further data analysis. Of the 31 patients in the left-side colon resection group, 24 patients received high anterior resection, 5 patients received low anterior resection, and 2 patients received left hemicolectomy. All operations were performed by a single surgeon.
We first analyzed the demographic data of the patients receiving different procedures as shown in Table 1. In the right-side colon resection group, there were 10 males (66.7%) and 5 females (33.3%) with a mean age of 54.5±12.2 years (range, 32–69 years). In the left-side colon resection group, there were 18 males (58.1%) and 13 females (41.9%) with a mean age of 61.8±12.8 years (range, 33–86 years). In the total colectomy group, there were 8 males (44.4%) and 10 females (55.6%) with a mean age of 39.3±17.3 years (range, 18–68 years). In general, no significant difference in gender, body mass index, or measurable tumor size was found among these three groups. Furthermore, it was expected that the patients in the total colectomy group might be younger than in the other two groups, which was indeed observed in our study.
Statistically significant difference.
Next, the surgical data and clinical outcomes among these three groups were further analyzed and are shown in Table 2. All operations were performed successfully without any intraoperative complications or need to convert to laparotomy. Similarly, there was no significant difference among these three groups with respect to the incision length and blood loss. However, longer duration of operation and longer of bowel resection were significantly noticed in the total colectomy group.
Statistically significant difference.
Furthermore, we observed that curved instruments were used in 5 patients in the left-side colon resection group. Among these five patients, 4 patients received a McBurney incision wound, and 1 patient received protective loop ileostomy created over the McBurney incision wound because of multiple underlying diseases. Nine of the 31 patients in the left-side colon resection group received an extra port (5 mm) over the left lower quadrant of the abdomen in addition to the umbilical incision wound because of difficult anatomy.
Finally, there was no obvious complication caused by surgery in any of these 64 patients postoperatively. Also, no significant difference in the incidence of postoperative stress ulcers, pain scores, or length of hospital stay was found among the three groups.
Discussion
To achieve better performance of SILC, a glove-port system was developed and used. Commercially available access systems offer immovable trocar sites. Instrument crowding may thereafter commonly occur when access devices with immovable trocar sites are used, especially when colectomy requires larger areas of dissection. Curved instruments may then be required, but this may eventually increase total cost expense. However, the high cost expense may be overcome by our self-made glove-port device. In addition to economic advantage, our self-made glove port, with designation of a 15-mm trocar used in the middle finger of the glove, a 10–12-mm trocar used in the thumb, and a 5-mm trocar used in the little finger, also made the range of movement large enough to overcome the instrument crowding. With greater range of movement, this glove port encounters less instrument crowding than commercially available devices. Uematsu et al. 20 also develop a novel access device for SILC, but this device requires an additional component and causes less freedom of movement of the instruments. To improve this drawback, they also develop another unique method, extracorporeal magnetic retraction. 21 However, we must emphasize that our self-made glove-port device is suitable for all body types (fat or thin) because the wound protector can be rolled for all kinds of body sizes of patients.
In this study, curved instruments were only used in 16.1% of the SILC cases with left-side colon resection, implying that the cost expense is a much more important point to consider than instrument crowding for patients. Moreover, most commercially available access devices are designed for laparoscopic cholecystectomies and appendectomies, which require a smaller wound of around 2.5 cm. However, this may contribute to instrument crowding. Fortunately, the wound size required for our device is typically 3–4 cm, which obviates the issue of instrument crowding. More important is that any type of trocar can be used for our self-made glove-port system.
It is worth mentioning that the results obtained from SILC with our self-made device were compatible with others in the literature as follows. Geisler and Garrett 22 reported in a study of 102 consecutive cases of SILC, including 23 cases of total colectomy, an average operating time of 99 minutes, mean length of incision of 3.7 cm, and average estimated blood loss of 140 mL. Furthermore, in 5 patients with diagnosis of either ulcerative colitis (n=4) or familial adenomatous polyposis (n=1) receiving single-port laparoscopic total proctocolectomy with ileal pouch–anal anastomosis, Geisler et al. 23 obtained the results of a median age of 43 years, a median body mass index of 20.66 kg/m2, a median operative time of 153 minutes, and a median estimated blood loss of 100 mL. The results from the study of Baig et al. 24 showed a mean age of 58 years and body mass index of 23.9 kg/m2 in 35 cases of consecutive SILC, including 8 cases of total colectomies. Also, they concluded that the glove-port technique not only facilitates procedural frequency and familiarity, but also is economically favorable. Finally, Leblanc et al. 25 and van den Boezem and Sietses 26 both demonstrated SILS for total colectomy as a safe and feasible procedure. Coupling these studies with ours suggests the safety and feasibility of SILC.
On the other hand, we compared the short-term surgical results among these three colon resection procedures for benign colon diseases in this study and found that single-incision laparoscopic total colectomy was a safe procedure as well compared with single-side colon resection regarding patient data, including the incision length, blood loss, incidence of postoperative stress ulcers, pain scores, and length of hospital stay. In this total colectomy group with 18 patients, 8 cases were familial adenomatous polyposis, 5 cases were colonic inertia, 2 cases were diverticulosis, and 3 cases were multiple colon polyps. We expected that the statistically significant younger age of the patients in the total colectomy group may be due to the relatively younger age distribution of the patients with familial adenomatous polypsis and colonic inertia. Furthermore, a longer duration of operation and longer length of bowel resection were indeed significantly found in the total colectomy group compared with the other two groups in this study. However, the clinical outcome of the single-incision laparoscopic total colectomy in this study was similar to that in other studies as mentioned previously.22–26 Because of the relatively small size of the benign lesions, less extension was required for the incision wound while retrieving the specimen, which makes the wound smaller and achieves a better cosmetic appearance than that of malignant lesions. Based on the requirement of cosmetic appearance, the preservation of the abdominal wall and limited incisional access may be attractive in those patients at a relatively younger age undergoing total colectomy for familial adenomatous polyposis and colonic inertia. 27 However, this awaits further investigation to strongly support our conclusion.
In conclusion, the results of this study provide strong evidence of the feasibility of SILS for the treatment of benign colorectal diseases. The simple self-made glove-port system indicates a practical method of SILS for colorectal diseases. Moreover, single-incision laparoscopic total colectomy has a compatible clinical outcome for the patients with benign colon diseases compared with the other two surgical procedures in this study.
Disclosure Statement
No competing financial interests exist.