
Abstract
Abstract
Background:
The current treatments available for bromhidrosis, such as subdermal excision of the apocrine glands, liposuction-curettage, and laser therapy, have certain drawbacks, for example, requirement of repeated treatments, high recurrence rate, and induration, pain, and scarring in the armpits. In this study we aimed to investigate the clinical efficacy and complications of endoscopic surgery for treatment of bromhidrosis.
Patients and Methods:
From August 2010 to June 2013, 18 patients (15 women and 3 men; mean age, 31 years old; age range, 19–40 years) with axillary bromhidrosis underwent endoscopic resection of the apocrine glands. The clinical efficiency and patient satisfaction were investigated by the Dermatology Quality Life Index scoring system, and complications of the surgery were assessed.
Results:
The mean operative time was 128 minutes (range, 92–164 minutes). Subcutaneous fluid drainage occurred in 5 of the 18 patients. Skin necrosis, upper limb edema, and bleeding did not occur in any patient. In 2 patients, subcutaneous fluid accumulation recurred after discharge. Numbness of the inside of the upper arm occurred in 3 patients. After approximately 0.5–2 years of follow-up, all patients had considerably reduced axillary sweating. The Dermatology Quality Life Index assessment indicated that the influence of bromhidrosis on the patients' life quality was greatly reduced.
Conclusions:
Our endoscopic surgical technique for the treatment of axillary bromhidrosis causes minimal tissue damage, allows full exposure, and is associated with few complications and a low recurrence rate.
Introduction
B
Clinical treatment options for this condition include subdermal excision of the apocrine glands,2–4 liposuction-curettage,5–7 and laser therapy.8,9 Conservative therapies are also used such as topical medications, 10 systemic agents, injections, 11 and physical therapy (iontophoresis). But, conservative management therapies could not achieve a permanent effect because of their drawbacks of repeated treatments, high recurrence rate, and induration, pain, and scarring in the armpits. 12 Local surgical excision of the apocrine glands has been proved to be the most effective surgery, but it has a relatively high risk of complications, of which skin necrosis is the most severe complication. 13
The commonly used method of apocrine resection is subcutaneous apocrine gland curettage. 14 This treatment does not cause obvious scarring of the armpits, but because the surgical area is not well defined, the apocrine glands cannot be removed completely. Fusiform-shaped excision of the axillary skin can maximize the removal of apocrine tissue, with reliable efficacy and a low recurrence rate 15 ; however, the resultant scarring limits shoulder abduction, and therefore this technique has gradually fallen out of favor. Excision of the apocrine glands through a small incision has also been attempted. 16 The resultant scar is small and hidden, but the apocrine glands cannot be completely removed through the small incision. 17 Therefore, precise location of the apocrine glands is very important for treatment of bromhidrosis to reduce the complications. Recently, many researchers have reported the use of endoscopic/arthroscopic-assisted surgery for completely resection of the apocrine glands.16,18–21
The Dermatology Quality Life Index (DLQI) is a questionnaire that has been widely used as a health-related quality of life measure for patients suffering from skin disease. 22 In this study, we attempted to perform endoscopic apocrine resection surgery to treat bromhidrosis. The clinical efficiency and patients' satisfaction were investigated by the DLQI scoring system, and complications of the surgery were assessed after a 0.5–2-year follow-up.
Patients and Methods
Patients
Between August 2010 and June 2013, 18 patients (15 women and 3 men), ranging in age from 19 to 40 (mean, 31) years old, underwent endoscopic apocrine resection for the treatment of axillary bromhidrosis in Wuxi People's Hospital (Wuxi, Jiangsu Province, China). All patients provided informed consent before surgery. The study was supported by Wuxi People's Hospital. The protocol was approved by the hospital's Medical Research Ethics Committee.
Preoperative preparation
Blood coagulation tests, chest radiographs, and electrocardiograms were obtained before surgery. In young women, the surgery was scheduled such that it did not coincide with their menstrual periods. The armpit hair was shaved, and the patients were placed in a supine position with their arms abducted to about 90° in order to fully expose the axilla. The surgery site should avoid the hair-bearing area. The axillary hair-bearing area along with a 1-cm-wide hair-free outer margin was marked (the ellipse-marked area in Fig. 1).

The position marked for incisions. Incisions should be made beyond the 1-cm-wide outer margin of the axillary hair-bearing area (ellipse-marked area). The black mark in the midaxillary line was the location of the 10-mm incision for placing the endoscopic tube. Either one of the other two black marks located the 5-mm incision for placing the operating apparatus according to surgical convenience.
Surgical technique
A 10-mm incision in the midaxillary line and a 5-mm incision in the posterior axillary line were made beyond the axillary hair-bearing area (Fig. 1). Blunt dissection of the deep fascia was performed in order to establish the catheter space. Then a 10-mm trocar and a 5-mm trocar were placed through the above incisions as the observation hole and the operation hole, respectively. Carbon dioxide gas was insufflated at a pressure of 4–6 mm Hg. A Harmonic® scalpel (Ethicon Endo-Surgery, Blue Ash, OH) was used to establish the subcutaneous operating space, which extended from the pectoralis major medially to the latissimus dorsi laterally, between the superficial and deep fascia. The loosened layers of the dermis and subcutaneous tissue containing the apocrine glands were carefully undermined with a pair of endoscopic scissors, and the apocrine glands were then separated from the skin. The remaining few apocrine glands attached to the dermis were excised carefully, to avoid injury to the subdermal vascular plexus (Fig. 2). A low-vacuum drain was placed in the axilla, and an elastic bandage was wrapped over the axilla. Arm movement was strictly limited for 4 days after surgery to allow reestablishment of the skin vascular supply. When fluid drainage was less than 10 mL/day, the tube was removed (Fig. 3).
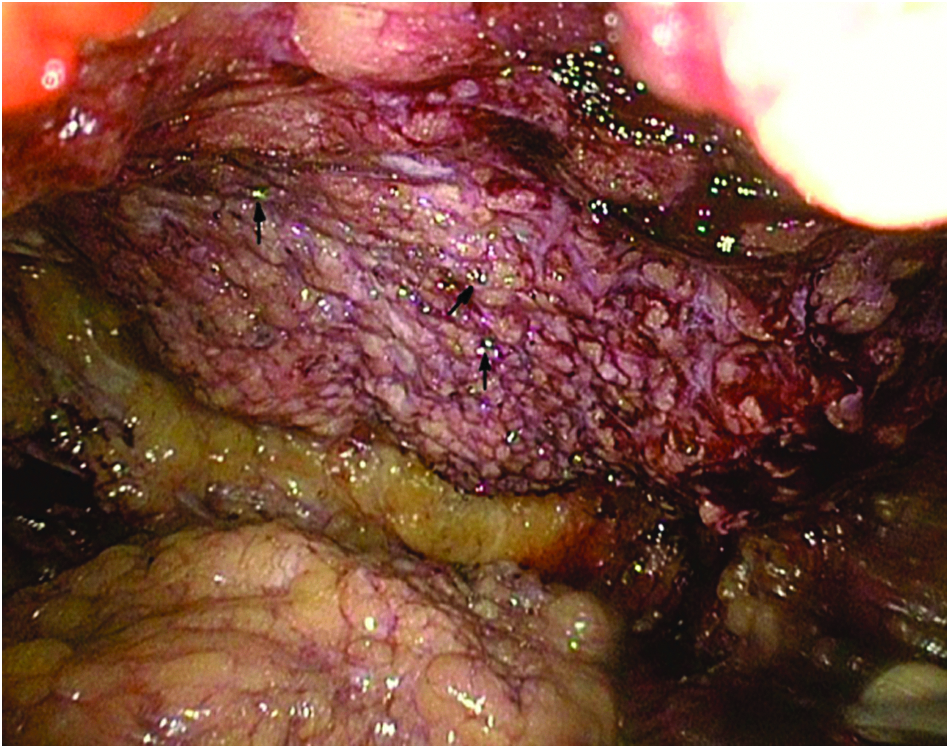
Loosened layers of the dermis and subcutaneous tissue containing apocrine glands were carefully undermined with a pair of endoscopic scissors, and the apocrine glands were separated from the skin. The black arrows indicate hair follicles.

Examination of the outcome after discharge. The blood supply of the axillary skin was good. Only two small scars measuring less than 1 cm each were present.
Postoperative care and complications inspection
With the patient supine and the head to one side after return to the ward, a semirecumbent position was adopted in favor of breathing and drainage if the patient did not complain of discomfort after regaining consciousness. The patient was assisted to turn over, and the back was patted to prevent lung infections. Postoperatively, patients were instructed to avoid eating spicy foods and drinking alcohol, in order to prevent bleeding and expansion of the sweat glands. Strenuous activity and extreme movement of the upper arms should be avoided.
Complications were assessed by clinical inspection of the wound 1 week after the procedure. Subcutaneous fluid accumulation was prevented by continuous axillary drainage and maintaining unobstructed negative pressure drainage. A partial compression bandage was used 2–3 days later. After postoperative suction drainage for 3 days, the drainage tube was pulled out, and when the drainage volume was less than 20 mL/day, the subcutaneous fluid aspiration was observed. An upper arm position was taken in the endoscopic surgery so that the armpit was exposed, which for a long time will lead to bilateral brachial plexus compression. Any abnormal conditions (numbness, pain, and burning sensation) of the skin of upper lateral area and fingers were closely observed.
Assessment of clinical efficacy and patients' satisfaction
The clinical efficacy and satisfaction were evaluated according to the DQLI scoring system. A questionnaire was used to investigate patients' satisfaction with the surgery. If the total DLQI score was 0–1, it was considered that there was no effect on the patient's life; 2–5, a small effect; 6–10, a moderate effect; 11–20, a very large effect; and 21–30, an extremely large effect on the patient's life. The follow-up period averaged 0.5–2 years. Malodor elimination, axillary sweating reduction, and reduced hair growth were also investigated. In the end, patients were given the power to evaluate whether they were totally satisfied with, partially satisfied with, or regretful about the procedure concerning the convenience of the surgery, surgical complications, and cosmetic outcome.
Results
In total, 18 consecutive patients with bromhidrosis were treated with endoscopic surgery. The mean operation time was 128 minutes (range, 92–164 minutes). The mean hospitalization time after operation was 5 days.
Effectiveness of the endoscopic surgical treatment of bromhidrosis
The status of bromhidrosis in all patients was improved with an average follow-up of 6 months after surgery (Table 1). A significant malodor elimination reduction (in 16 of the 18 patients) was obtained such that no malodor was smelled even when the patient was sweating. An improved result (2 in 18 patients) was obtained in that the malodor was much reduced but was still occasionally noticeable to the patient only when he or she was sweating. After approximately 0.5–2 years of follow-up, all patients reported a considerable reduction in axillary sweating. Axillary hair growth was significantly reduced in most patients (83%).
BMI, body mass index.
Complications following endoscopic surgical treatment of bromhidrosis
Complications following the surgery are given in Table 2. Subcutaneous fluid drainage occurred in 5 of the 18 patients. The drain was removed in approximately 4 days. None of the patients developed bleeding, skin necrosis, wound infection, upper limb edema, or shoulder joint activity obstacle. In 2 patients, subcutaneous fluid accumulation occurred 8–14 days after discharge and was drained by percutaneous puncture. Three patients developed numbness of the medial aspect of the upper arm, and this symptom generally disappeared within 1 month after the operation.
Patients' satisfaction assessed by DLQI scoring system
About 72% (13 in 18 patients) of the bromhidrosis patients were totally satisfied, and 5 patients were partially satisfied with the effectiveness of endoscopic surgical treatment (Table 1). The DLQI scores are given in Table 3. In this study, the patients' life was greatly affected by the bromhidrosis (total DLQI score, 13), and after treatment with the endoscopic apocrine resection, patients were more self-assured, and the negative impact of bromhidrosis on their daily life, social activities, and work or study had greatly decreased (total DLQI score, 1).
The Dermatology Life Quality Index (DLQI) was scored as follows: very much, 3; a lot, 2; a little, 1; and not at all, 0.
Discussion
Bromhidrosis is a distressing and troublesome problem that seriously affects the daily and social life quality of affected patients. The clinical treatments available for bromhidrosis include liposuction, 6 the glycine–soja sterocomplex topical agent, 10 and apocrine gland subcision. 13 Among these treatments, apocrine gland subcision with an ultrasonic scalpel and endoscope is reported to be the most effective treatment. 23 Yoo et al. 21 have performed endoscope-assisted ultrasonic surgery to treat axillary bromhidrosis. This method offers the advantages of a small surgical incision, hidden wound, and short recovery time but is associated with the risk of recurrence because the apocrine glands cannot be completely removed. According to the 2006 publication by Yoo et al., 21 the odor release recurred 3 months later, and complications such as congestion, hematoma, seroma, and wound dehiscence occurred in 28 out of 896 patients (3.1%). Superficial epidermis necrosis was an additional incentive that was reported by 37% of patients studied by Qian and Wang. 1 In the present study, we completely removed the apocrine glands with endoscopic scissors, and malodor was eliminated in all 18 patients with no recurrence, bleeding, infection, skin necrosis, or edema in the 0.5–2-year follow-up.
Our endoscopic method involved only two small incisions (10 mm and 5 mm) and caused minimal injury; moreover, the incisions were hidden, and no axillary scarring occurred. Furthermore, the glands were excised under direct vision, and the clear observation of the subdermal vascular network helped to effectively prevent intraoperative vascular injury. Postoperative skin hematoma and flap necrosis were completely avoided with this technique in our study, as well as the lack of recurrence in 0.5–2 years of follow-up.
However, there were some limitations of long operative time, requirement for general anesthesia, and expensive cost. Additionally, complications such as subcutaneous fluid accumulation (in 2 patients) and numbness (in 3 patients) occurred, which has rarely been reported by other researchers. Subcutaneous fluid accumulation might be caused by the liquefaction and necrosis of the hair follicles and glands in the space between the flap and subcutaneous tissue. The numbness inside of the upper arm might be caused by injury to an intercostobrachial nerve. However, these symptoms had disappeared, respectively, within 2 weeks and 1 month later. Shelley and Butterworth 24 reported that absence of axillary hair may be related to an associated underdevelopment or absence of the axillary apocrine sweat glands. Qian and Wang 1 also reported a 95% hair loss rate in the patients with subdermal excision of apocrine glands. In the present study, we completely removed the apocrine glands, which may be the reason of hair loss (83%). In addition, many female patients showing the complication of axillary hirsutism were extremely satisfied with the axillary hair reduction. 1
The changes in patients' daily life quality and mental state were assessed. We used the DLQI questionnaire, which has been widely used to measure the health-related life quality for patients suffering from skin disease, to evaluate the influence of the axillary bromhidrosis before and after the surgery. From the results, we concluded that patients achieved more confidence in daily life after the endoscopic surgery for bromhidrosis. In addition, it should be noted that there is a major limitation in the present study in that the sample size is small. However, the findings in the present study are still very important for treatment of bromhidrosis. More randomized controlled trials with larger sample size are vitally important to obtained more solid evidence in the future.
In conclusion, the present endoscopic surgical technique for the treatment of axillary bromhidrosis caused minimal tissue damage while enabling full exposure and was associated with few complications and low recurrence rate. Long operative time, requirement for general anesthesia, and high cost are the main drawbacks of our technique.
Disclosure Statement
No competing financial interests exist.