
Abstract
Abstract
Purpose:
To compare the outcomes of laparoscopic surgery and open surgery for gastric gastrointestinal stromal tumors (GISTs) by size-matched analysis and evaluate whether laparoscopic surgery for lesions of >5 cm is feasible.
Patients and Methods:
Data of 44 consecutive patients with gastric GIST who underwent surgery from 1988 to 2011 were reviewed. Twenty-three patients who underwent successful laparoscopic surgery were compared with 10 patients with similar tumor sizes who underwent open surgery. Among the 23 patients in the laparoscopic group, we compared postoperative results between GISTs of ≤5 cm and >5 cm.
Results:
There were no differences in clinicopathological characteristics between the laparoscopic surgery group (LG) and the open surgery group (OG). The operation time was not different, but the blood loss (5.5 mL [range, 0–425 mL] in LG and 125 mL [range, 0–676 mL] in OG) (P=.008) and postoperative hospital stay (21 days in OG and 8 days in LG) (P<.001) were significantly less in the LG. Postoperative complications and recurrence were not different. Comparison between patients with lesions of >5 cm and patients with smaller lesions in the LG found that smaller lesions were associated with a shorter postoperative hospital stay (7.5 days versus 11 days) (P=.037).
Conclusions:
Laparoscopic resection of primary gastric GISTs is feasible even for tumors of >5 cm.
Introduction
G
Wide resection margins have not shown benefit6,14; therefore, a laparoscopic approach may be considered for select GISTs in favorable anatomical locations.1,2,13,14 However, there are several controversies regarding laparoscopic resection of gastric GISTs. First, although several reports have shown that laparoscopic surgery is feasible and has the benefit of minimal invasiveness,14,15 larger tumors tend to be approached by open surgery, and the reported advantages of the laparoscopic approach over the open approach may be the result of this selection bias. Second, the 2011 National Comprehensive Cancer Network guidelines 1 and clinical practice guidelines for GIST in Japan 13 suggested that laparoscopic resection is safe only for tumors of ≤5 cm; however, the feasibility and safety of laparoscopic resection for GISTs of >5 cm are still unclear.
In this study, we compared open versus laparoscopic approaches for gastric GISTs with size-matched analysis. We then investigated the feasibility and safety of laparoscopic resection for gastric GISTs of >5 cm.
Patients and Methods
A retrospective review of a collected database was searched for the last 44 patients who underwent primary resection for gastric GIST by the upper gastrointestinal surgery group of the Department of Surgery and Oncology, Kyushu University Hospital, Fukuoka, Japan. The resections were performed between October 1988 and May 2011. The surgical approach was selected based on the surgeon's decision. All operations were performed by the same surgical team. We excluded previously treated gastric GISTs and advanced metastatic/unresectable gastric GISTs. Immunohistochemical analyses for KIT (CD117), CD 34, α-smooth muscle actin, S-100 protein, vimentin, desmin, and Ki-67 were performed for diagnosis. The diagnosis of GIST in this retrospective study was made from compatible histological pathology on light microscopy and the positivity of CD117 (KIT) expression.1,13,16
Clinical data included patient age and gender, clinical presentation, physical examination, operative details, clinical diagnosis, and tumor recurrence. Pathological data included tumor location and gross appearance. Data on tumor size (maximum diameter in cm), growth pattern, mitotic figures, and immunohistochemical results were collected from medical records. The extent of resection was defined as follows: R0=no residual tumor, R1=microscopic residual tumor with positive resection margin, and R2=macroscopic residual tumor. 17 Recurrence-free survival time was defined as the time from surgery until the time of clinical or radiological evidence of relapse. Each tumor was categorized as very low risk, low risk, intermediate risk, or high risk according to the Joensuu risk criteria.18,19
Thirty-three patients with GIST of the stomach were included in our study. Twenty-three patients underwent laparoscopic resection. Because the largest tumor in the laparoscopic surgery group (LG) was <10 cm, we matched these patients with 10 patients in the open surgery group (OG) with a tumor size of <10 cm who underwent complete resection. According to the guideline from the Japanese Study Group on GIST in Japan, 13 the indication for use of imatinib for GIST is only for the patients with unresectable tumor, noncurative resection, and recurrent disease, and imatinib was not used as an adjuvant treatment in any patient.
Patient and tumor characteristics and other clinical parameters were compared between the two groups. To determine whether laparoscopic surgery for gastric GIST of >5 cm is feasible and has results equal to those for lesions ≤5 cm, comparison between the two groups of patients according to tumor size in the LG was performed.
Surgical technique for laparoscopic resection
Laparoscopic resection was indicated for tumors <10 cm in size in our institution. However, we considered it technically difficult to resect a tumor without any spillage or damage, so we performed an open procedure. The patient was placed under general anesthesia in the supine position with his or her legs spread apart. A surgeon stood on the right side of the patient, while an assistant stood on the left side. A camera operator stood between the patient's legs. A Hasson trocar was inserted using an open technique with a 10-mm incision. Carbon dioxide was insufflated through this port with a pressure setting of 8 mm Hg. A 30° laparoscope was introduced through the umbilical port, and diagnostic laparoscopy was performed. Two 5-mm ports were inserted into the left and right sides of the 12-mm port as shown in Figure 1. We placed an additional port if necessary. The jejunum was clamped by clamp forceps 5–10 cm from the ligament of Treitz (Fig. 2), and the tumor location was confirmed by endoscopy. Contact with the surface of the tumor was avoided even if the tumor did not expand to the serosa. The boundary of tumor was marked by methylene blue dye paint. If necessary, gastric vessels or the omentum around the tumor was divided using ultrasonic coagulating shears (SonoSurg™ X; Olympus Co., Ltd., Tokyo, Japan) or a vessel divider and sealer (LigaSure™; Covidien, Ltd., Tokyo). For some anterior or posterior gastric wall lesions, tumors were removed by the lesion-lifting method. Most tumors were laparoscopically resected with a linear stapler (Figs. 3 and 4). When we resected the tumor, we introduced a 5-mm laparoscope though the 5-mm port and introduced a linear stapler though the 12-mm port. Tumors involving the esophagogastric junction and pylorus were removed by laparoscopic proximal gastrectomy and laparoscopic distal gastrectomy without lymphadenectomy, respectively. The resected specimen was isolated within a specimen bag at an early phase of the procedure whenever possible to avoid instrumental contact and potential risk of dissemination, enabling us to lift the lesion for resection using the linear stapler, and retrieved from the elongated umbilical wound.
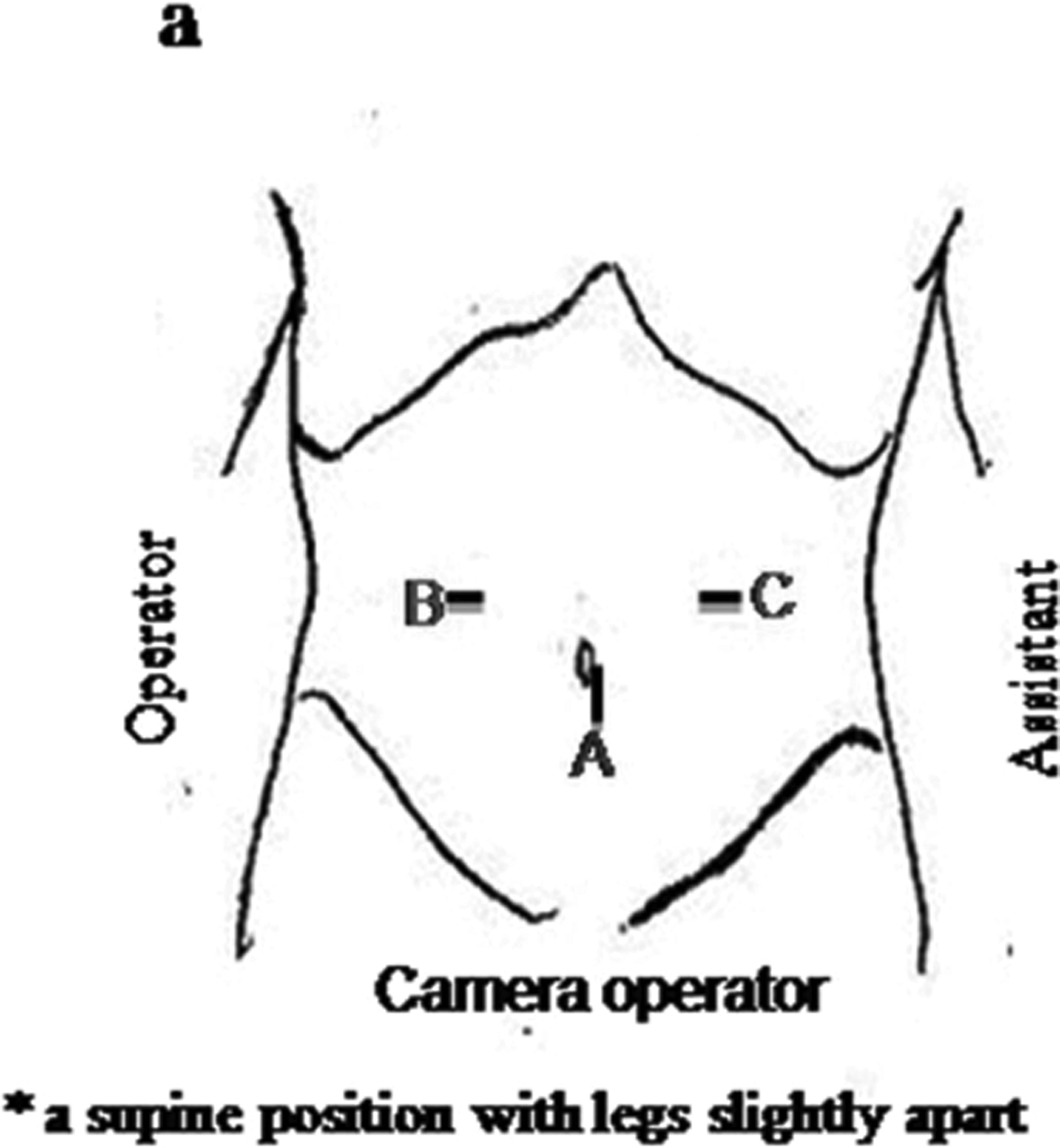
Port incisions: site A, the 12-mm port for the laparoscope; sites B and C, the 5-mm working ports for the surgeon.
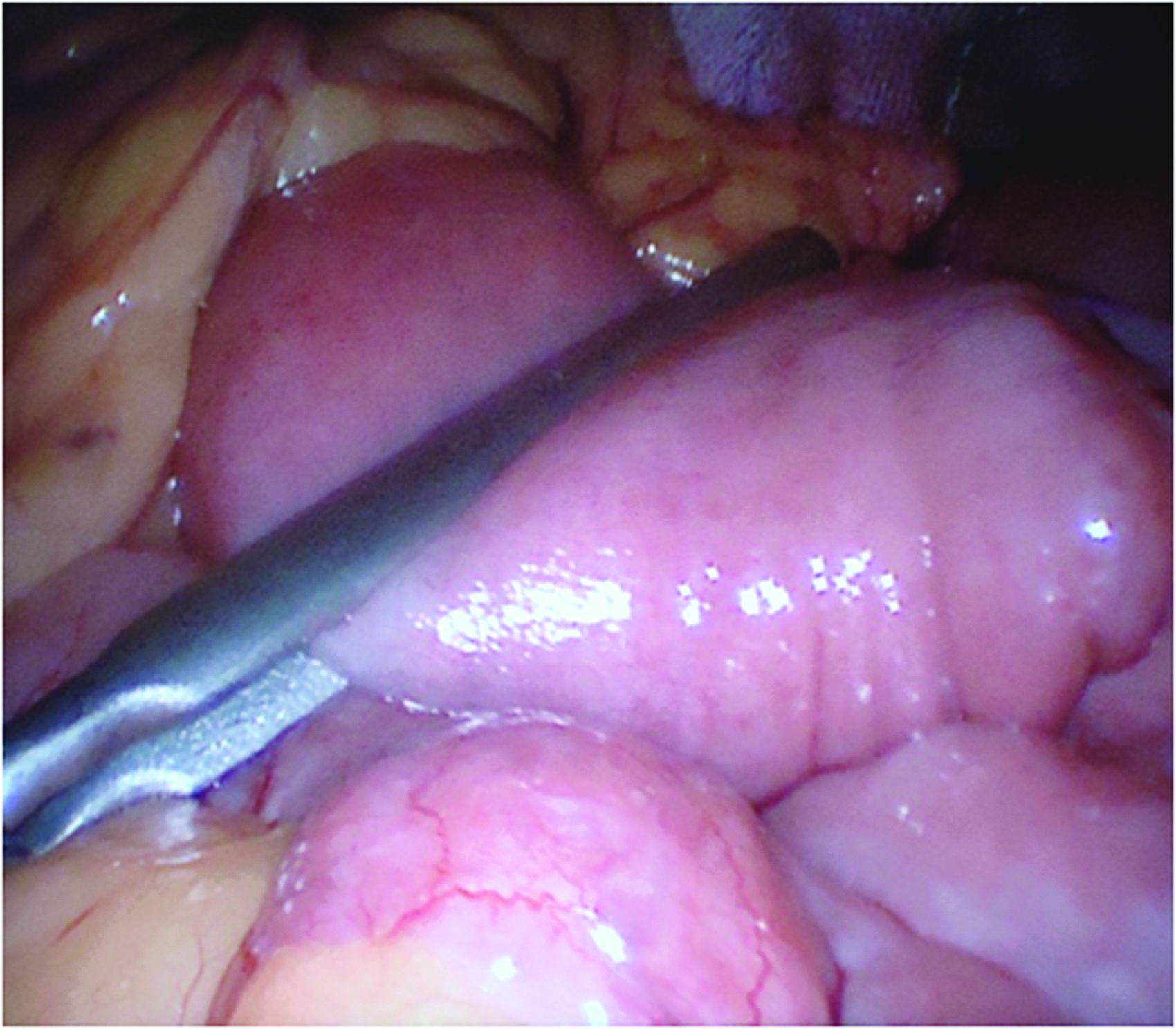
The jejunum was clamped 5–10 cm from the ligament of Treitz before endoscopy was performed to prevent intestinal dilatation with the supplied carbon dioxide.
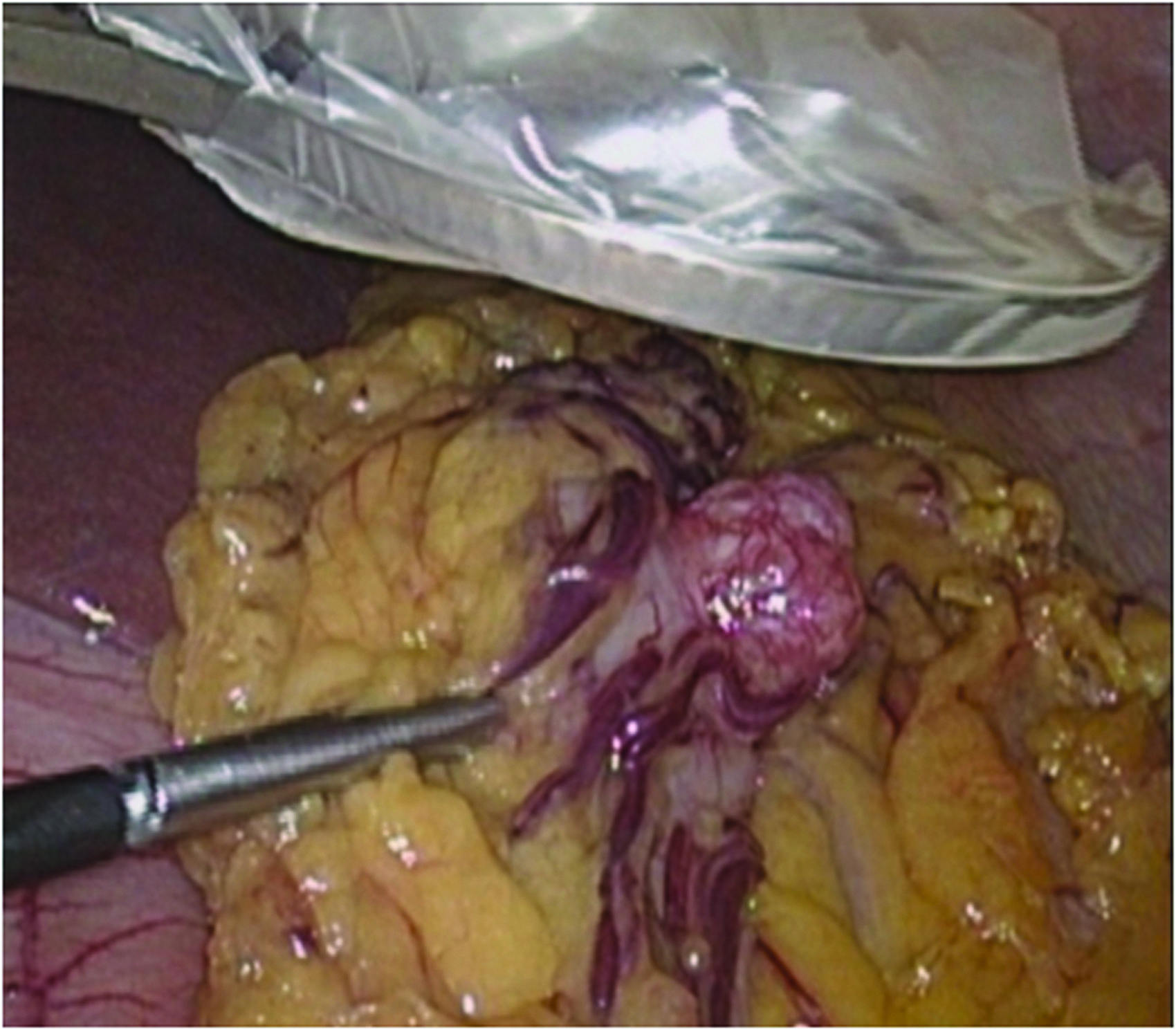
The tumor was protected before resection.
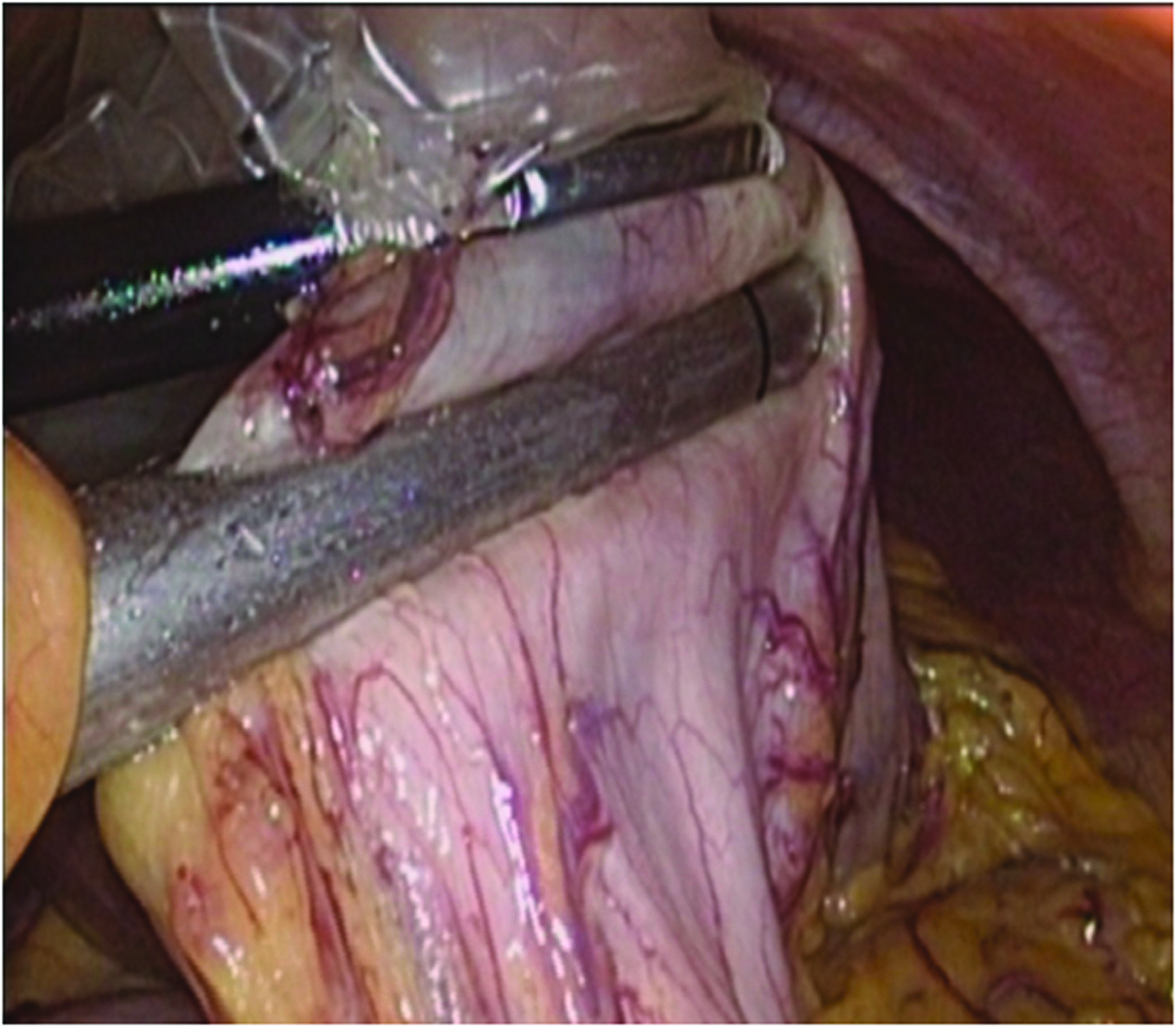
Resection was done with a linear stapler with a safety margin.
Statistical analysis
Continuous variables were summarized as mean (standard deviation) or median (range) as appropriate. Categorized variables were summarized as percentages or counts. Statistical analysis of categorical variables was conducted with the chi-squared test or Fisher's exact test. The Mann–Whitney U test was used to compare continuous parameters. Analyses of cumulative disease-free survival and cumulative survival were performed by Kaplan–Meier analysis. A value of P<.05 was considered statistically significant. All statistical analyses were performed using SPSS software (version 15.0 for Windows; SPSS, Inc., Chicago, IL).
Results
Clinicopathological characteristics of patients
Clinical and pathological variables of patients are summarized in Table 1. The LG and OG comprised 23 patients (8 [34.8%] males, 15 [65.2%] females) and 10 patients (6 [60.0%] males, 4 [40.0%] females), respectively. Most tumors in both groups were spindle cell-type tumors (88.2% in LG and 70% in OG). The median age of patients in the LG and OG was 69 and 64 years, respectively. The median tumor size in the LG and OG was 2.9 cm (range, 1–7 cm) and 4.7 cm (range, 1.2–9.6 cm), respectively. There were no significant differences between the LG and OG in terms of age, gender, tumor location, or tumor size. There were also no differences in pathological factors, such as the mitotic rate, risk category, and tumor cell types, between the two groups.
GIST, gastrointestinal stromal tumor; HPF, high-power field; LG, laparoscopic surgery group; OG, open surgery group.
Operative characteristics and postoperative outcomes
All patients underwent complete resection (R0). Of 20 patients who underwent partial resection of the stomach in the LG, 4 underwent the lesion-lifting technique, and the remaining 16 patients underwent tumor removal by extragastric resection. 20 The operative blood loss volume (125 mL in OG and 5.5 mL in LG) (P=.008) and length of postoperative hospital stay (21 days in OG and 8 days in LG) (P<.001) were significantly less in the LG. The median operative time (170 minutes in OG and 121 minutes in LG) (P=.09) was similar in both groups. In terms of complications, 1 patient in the LG developed pneumonia, and 1 patient in the OG experienced delayed gastric emptying. The patient in the LG who had postoperative pneumonia underwent laparoscopic partial resection and stayed 10 days in the hospital. He was alive without recurrence at 4 years after operation. One patient in the OG who underwent proximal gastrectomy developed postoperative delayed gastric emptying. The patient stayed the hospital for 1 month, and in outpatient follow-up, he is alive without any complication and recurrence at 3.5 years after operation. The incidence of complications was not significantly different between the two groups (P=.52). With a median follow-up time of 42 months (range, 1–275 months), there was no recurrence in the LG, whereas 1 patient in the OG with a 5-cm tumor at the body of the stomach and a mitotic rate of 25/50 per high-power field developed recurrence at the upper part of the stomach and metastatic disease in the liver 11 months after surgery. He underwent the second operation for resection the metastasis tumors. After the second operation, he received imatinib treatment and still alive at 59 months after the operation. All patients were alive at the end of the follow-up period (Table 2).
Level of significance for P values was<.05.
One patient underwent concomitant cholecystectomy at the same operation.
P value is calculated by the log rank method.
LG, laparoscopic surgery group; NA, not applicable; OG, open surgery group.
Characteristics of patients in the LG stratified by tumor size
We next analyzed the feasibility of laparoscopic surgery for GISTs of >5 cm. Characteristics of the 23 patients in the LG are summarized in Table 3. Eighteen patients (7 males, 11 females) had tumors of ≤5 cm, and 5 patients (1 male and 4 females) had tumors of >5 cm. The median age, lesion location, and mitotic count were comparable between the two groups. The majority of patients with lesions of ≤5 cm (15 patients) were categorized as having a low risk of recurrence, whereas all patients with lesions of >5 cm were considered to have an intermediate risk.
GIST, gastrointestinal stromal tumor; HPF, high-power field; NA, not applicable.
Operative data and surgical outcomes of patients in the LG stratified by tumor size
Seventeen patients with lesions of ≤5 cm underwent partial gastric resection, and 1 patient underwent distal gastrectomy. Three patients with lesions of >5 cm underwent partial gastric resection, 1 underwent proximal gastrectomy, and another underwent segmental gastrectomy. The median operative time, complications, and median blood loss volume were similar between the two groups. Patients with lesions of ≤5 cm had shorter postoperative hospital stays (7.5 days in patients with a tumor ≤5 cm and 11 days in those with a tumor >5 cm) (P=.037) (Table 4). Details of patients with GISTs of >5 cm are summarized in Table 5.
Level of significance for P values was<.05.
One patient underwent concomitant cholecystectomy at the same operation.
P value was unable to be calculated owing to the small number of patients.
NA, not applicable.
F, female; M, male.
Discussion
We herein reported the technical acceptability and safety of laparoscopic resection for patients with gastric GIST. The volume of blood loss and postoperative hospital stay were less in the LG compared with the OG, while the operation time was similar. We also reported the successful treatment of >5-cm gastric GISTs by the laparoscopic technique.
Laparoscopic surgery is increasing in popularity for GIST treatment, and the 2011 National Comprehensive Cancer Network guidelines 1 and clinical practice guidelines for GIST in Japan 13 suggested that laparoscopic resection is safe for tumors of <5 cm. However, there has been no prospective randomized trial directly comparing laparoscopic and open surgery. Although several previous series reported the feasibility and oncological safety of laparoscopic surgery for GIST,14,15,21–27 there have been few reports comparing open surgery and laparoscopic surgery for GIST.14,27 In addition, the benefit of the laparoscopic approach may be the result of selection bias because larger tumors tend to be approached by open resection. Therefore, we selected patients in the OG and LG with similarly sized tumors and found that the amount of blood loss was smaller in the LG compared with that in the OG. There was no recurrence in the LG. These findings suggest that laparoscopic resection is safe and feasible in terms of oncologic outcome and has the benefit of a minimally invasive approach. The length of hospital stay in the LG in our series was longer than that reported in Western countries.14,22,26,27 The explanation may be the differences in the health insurance system. The postoperative morbidity rate (4.3%) of laparoscopic surgery in our study was comparable with that in other studies (0%–16.4%).14,21,22,26,27 The recurrence rate after laparoscopic resection for gastric GIST has been reported to range from 0% to 8%.15,21,24,25 With a median follow-up of 42 months (1–275 months), there was no recurrence in the LG, whereas there was one recurrence in the OG.
The other controversy of the minimally invasive approach regards the tumor size that is safe for laparoscopic resection. Several studies have reported the success and safety of laparoscopic resection for large gastric GISTs.14,21–23,26,27 The clinical practice guidelines for GISTs in Japan 13 suggested that a laparoscopic approach should be limited to tumors of <5 cm. De Vogelaere et al. 21 recently reported the feasibility of laparoscopic surgery irrespective of size. However, the borderline of analyzed sizes was 2 cm in that report. No study has compared gastric GISTs of ≤5 cm with those >5 cm. Our study has shown that laparoscopic surgery for gastric GISTs of >5 cm is safe and that the postoperative outcomes are comparable with those of laparoscopic surgery for smaller lesions in terms of operative time, operative blood loss volume, and complications. The postoperative hospital stay in our study was longer than others from Western countries21,22,26; however, this is typical in Japan, similar to the results from many studies in Japan. Shimizu et al. 20 and Otani et al. 28 reported respective postoperative hospital stays of 13.2 days and 7.2–13.7 days in the group undergoing laparoscopic surgery. The explanation for this is the medical insurance system in Japan, which encourages patients to stay longer. Even in this circumstance, the length of hospital stay in the laparoscopic group is shorter than that in the open group. Therefore, we consider the laparoscopic procedure may contribute to the shortening the hospital stay. The hospital stay for patients with larger tumors was longer than that in the other patients, but the difference may have little impact on the clinical significance. There was no disease-related mortality in either group. These findings suggest the oncologic safety of the minimally invasive approach.
We acknowledge that there are several limitations inherent to our retrospective analysis. First, the number of patients in our study was relatively small. Second, because the maximum size of tumors in our study was ≤10 cm, the safety and feasibility of laparoscopic resection for tumors of >10 cm remain controversial. Further study by prospective randomized controlled trials with larger numbers of patients and larger tumor sizes will help to determine the benefit of laparoscopic resection.
In conclusion, surgical treatment remains the gold standard therapy for resectable GISTs. Complete resection with preservation of the integrity of the capsule and avoidance of infiltration of the resection margins is the main principle of GIST surgery. The laparoscopic approach is considered to be safe and feasible for tumors of >5 cm in centers experienced with advanced laparoscopic surgery.
Footnotes
Disclosure Statement
No competing conflict of interest exist.