
Abstract
Abstract
Background:
The existence, etiology, diagnosis, and treatment of median arcuate ligament syndrome (MALS) have long been subjects of debate. To our knowledge, there have not been any studies assessing the effectiveness of surgical treatment in improving physical and psychological quality of life in pediatric patients.
Subjects and Methods:
This is an Institutional Review Board–approved prospective study including all patients undergoing surgical treatment of MALS between 2009 and 2012 at our institution. Demographic information, presenting symptoms, radiological imaging, procedure duration, hospital length of stay, and perioperative complications were gathered for analysis. Patients and their parents were asked to complete the Child Health Questionnaire, a physical and psychological health survey, both within 1 week prior to and at least 3 months following their surgery.
Results:
Six patients underwent laparoscopic release for MALS. The majority of patients were female (n=5 [83.3%]), with an average age of 15.7±1.5 years. Presenting symptoms lasted on average 16.5±12.7 months prior to treatment. Average pre- and postsurgical ultrasound celiac artery peak velocities with inspiration were 332.0±34.1 cm/second and 224.3±31.2 cm/second, respectively, with a statistically significant decrease of 107.67 cm/second (P=.03). The average follow-up period from time of surgery to time of quality of life survey completion was 13±11.3 months, with a range of 3–29 months. A significant improvement from pre- to postsurgical scores was observed in the physical functioning (P=.03), mental health (P=.03), and self-esteem categories (P=.03) of the child assessment. Similarly, there was a significant postsurgical improvement in all categories pertaining to the parent's quality of life (P=.03). Improvement was also seen in the parents' perception of their child's physical functioning (P=.03), bodily pain/discomfort (P=.03), mental health (P=.03), and general health perceptions (P=.03). No intraoperative or postoperative complications occurred.
Conclusions:
Our preliminary results demonstrate that laparoscopic median arcuate ligament release for MALS in the pediatric population is safe and effective and improves overall quality of life for the patients and their parents. In carefully selected patients, laparoscopic release for MALS without additional celiac artery reconstruction normalizes blood flow in the celiac artery and improves physical and psychosocial quality of life for the child and his or her parents.
Introduction
M
This debate likely stems from the ambiguity of the clinical presentation of MALS and whether invasive surgical treatment is warranted. Variance in early results of surgical treatment is likely due to the lack of a consistent definition of the disorder. Previous studies included subjects with a wide variety of symptoms, both physical and psychological. It is not surprising that surgical outcomes within these cohorts were also varied. Reilly et al. 2 described a large cohort that identified symptoms congruent with successful surgical repair. These symptoms are now widely used in the diagnosis of MALS and include postprandial pain, nausea, vomiting, weight loss, epigastric bruit (although not always present), and lack of psychological history.3,4
Although the prevalence of these symptoms and the treatment outcomes in the adult population are relatively well documented, data involving the pediatric population remain minimal.5,6 Additionally, there are no data assessing the physical and psychological quality of life improvement as a result of MALS treatment. As laparoscopic repair in pediatric MALS patients increases, it is important that we properly assess the surgical effects and outcomes in this population. Here we present our preliminary experience with laparoscopic release of the median arcuate ligament in 6 patients with MALS, including the medium-term outcomes and change in physical and psychological health following surgical intervention.
Subjects and Methods
This was an Institutional Review Board–approved, Health Insurance Portability and Accountability Act (HIPAA)–compliant prospective study involving all patients undergoing surgical treatment of MALS between 2009 and 2012 at the Mayo Clinic (Rochester, MN). Demographic information, presenting symptoms, duration of symptoms, radiological imaging studies, duration of procedure, hospital length of stay, and perioperative complications were gathered for analysis. Following informed consent, patients and their parents were asked to complete a validated physical and psychological health survey once within the week prior to surgery and again at least 3 months following their surgery.
We obtained a license and used the Child Health Questionnaire (CHQ)-87 (CHQ-87), a validated, health-related quality of life assessment instrument for children created by Landgraf et al. 7 The CHQ-87 is an 87-item Likert questionnaire that asks respondents to identify their level of agreement or disagreement with a series of statements in order to assess 12 different physical and psychosocial statuses. Because of variable survey compliance within certain categories, we limited our assessment to the following nine categories: physical functioning, role/social emotional, role/social behavioral, role/social physical, bodily pain, mental health, self-esteem, and general health perceptions. Informed consent and Institutional Review Board approval were obtained to allow the adolescents to complete the questionnaire themselves.
A U.S. normative standard has not yet been developed for the CHQ-87. The most comprehensive and internally consistent study was done in adolescent children in The Netherlands by Raat et al. 8 reporting Cronbach's alpha correlations ranging from 0.69 to 0.90. Data from this patient population were used as a normative comparison in our study.
Similarly, the CHQ-PF-50, a parent quality of life questionnaire that parallels the CHQ-87, was completed by either the father or mother of each child. The same nine health concepts were assessed, this time from the parent's perception of his or her child's health and well-being. Two additional concepts (parental impact–emotional and parental impact–time) were also assessed. Unlike the CHQ-87, a well-validated normative standard has been developed for the CHQ-PF-50 and was used to calculate comparison data in our study. Scoring of the CHQ-87 and CHQ-PF-50 consisted of averaging scores in each section and recoding and recalibrating them to positive scores ranging from 0 to 100. Higher scores signify greater satisfaction with health and quality of life.
Postoperative and preoperative scores were compared with Wilcoxon signed-rank tests separately for children and their parents. Using the same methods, we also compared CHQ-87 scores with the data provided by Raat et al. 8 in order to evaluate a comparison with normative standards. Each CHQ-PF-50 scale was compared with the U.S. norm using a z-score transformation. This score was calculated by taking the general U.S. population mean for a given scale and subtracting it from a sample's scale score. The difference is then divided by the general U.S. population's standard deviation. Corresponding categories between parents and their children were then compared using the Wilcoxon signed-rank test in order to identify any conflicting perceptions of medical treatment results. All analyses were performed using JMP software, version 9.0.1 (www.jmp.com).
Clinical work-up
Our algorithm for pediatric patients who had the potential diagnosis of MALS included an evaluation by pediatric gastroenterology, pediatric surgery, and vascular surgery. Other specialists were consulted as needed. To maintain individual and multidisciplinary expertise, we limited the individuals within each department evaluating pediatric patients once MALS was entertained. A typical work-up of these patients included history and physical exam, complete blood count, electrolyte panel, liver function and pancreatic enzyme serum tests, upper and lower endoscopy with biopsy, total abdominal and pelvic ultrasound (gallbladder and ovaries), duplex ultrasound of the aorta and mesenteric vessels (Fig. 1), delayed gastric emptying and enteric transit studies, either computed tomography (CT) enterography or upper gastrointestinal study with small bowel follow-through to evaluate the small bowel, CT angiogram and/or magnetic resonance imaging angiogram with inspiration and expiration films (Fig. 2), and other testing as needed (i.e., selective arterial angiography).
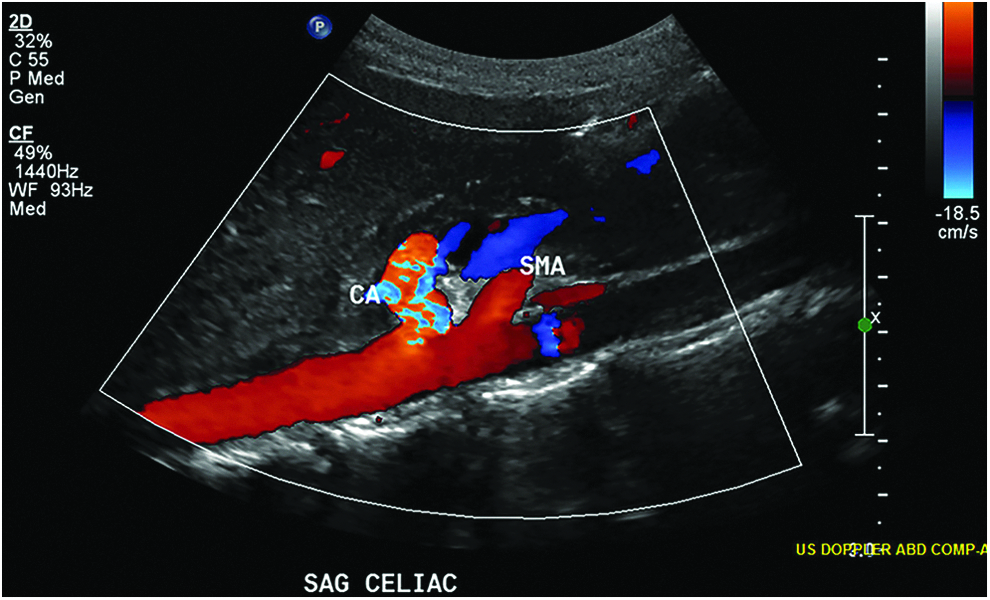
Duplex ultrasound of the aorta and mesenteric vessels. CA, celiac artery; SAG, sagittal; SMA, superior mesenteric artery.

Magnetic resonance imaging angiogram with expiration of a patient with median arcuate ligament syndrome.
Technique
Our transperitoneal laparoscopic technique was similar to that described by Said et al. 6 in our previous article on the first pediatric MALS patient. Both a pediatric surgeon and a vascular surgeon were present for all cases, with the pediatric surgeon (A.E.Z.) performing role of primary surgeon. Under general anesthesia and with arterial line placement, patients are positioned supine with the legs in stirrups, much like a standard laparoscopic Nissen fundoplication. A 12-mm trocar is inserted in the umbilicus, and four 5-mm trocars are placed in the right and left upper quadrants. The two most cranial trocars are placed high, just below the costal margin, medial to or at the mammary line. The other two trocars are placed approximately 6–8 cm caudal to the first two trocars. A liver retractor is used to elevate the left hepatic lobe in order to expose the gastrohepatic ligament. Dissection is started by opening up the gastrohepatic ligament with electrocautery. The peritoneum over the right crus is opened, and the retroesophageal space is developed. The right and left crus are exposed caudally as they decussate above the aorta. We exclusively use a technique that exposes the aorta first and then releases the median arcuate ligament cranially to caudally, directly anterior to the aorta coming onto the celiac artery (Fig. 3). This is opposed to dissecting the left gastric artery and then coming onto the celiac artery, followed by the aorta. We attempted the latter but found it a far more difficult dissection. We also frequently change the scope to a 10-mm, 45° scope or a 10-mm flexible scope to aid in directly viewing the median arcuate ligament fibers. The decussation of the right and left crus is dissected to expose the aorta. Dissection proceeds caudally and must remain on the aorta anteriorly without veering off in either direction as there are no named branches until the celiac artery is encountered. The antrum of the stomach and the pancreas will likely need to be retracted caudally. Tight bands and ganglion fibers are lysed using L-hook electrocautery on a low setting (i.e., 15). The fibers encountered here are tight and fibrous and compress the celiac axis from anterior to posterior, making the celiac axis nearly invisible. After one fiber at a time is lysed, the celiac artery will come into view as a bulge on the aorta. Care must be taken not to back-heel (touch with the curved part of the cautery hook) any artery as one is lifting up on the individual fibers. We advise against using other sources of energy for dissection. Dissection is continued until the celiac, common hepatic, and left gastric arteries are free 0.5–1.5 cm in either direction. No attempt should be made to re-approximate the crus. Although use of intraoperative ultrasound is an option, we elected not to use it either to guide dissection or to check velocities in widely patent arteries.

Intraoperative image of the aorta and celiac artery.
Results
Six patients underwent surgery for release of MALS, all of whom filled out pre- and postoperative surveys. The average age at time of surgery was 15.7±1.5 years. Five (83.3%) of the patients were female. The average duration of symptoms prior to surgery was 16.5±12.7 months. The description and prevalence of presenting symptoms are shown in Table 1. Procedure duration ranged from 99 to 235 minutes with an average time of 161.5±49.5 minutes. The postoperative hospital recovery period was 1.3±0.5 days on average. Average pre- and postsurgical ultrasound celiac artery peak velocities with inspiration were 332.0±34.1 cm/second and 224.3±31.2 cm/second, respectively, with a statistically significant decrease of 107.67 cm/second (P=.03). All peak velocity imaging was completed in the supine position following at least 6 hours of fasting to avoid falsely elevated velocities. The timing of postoperative peak velocity studies ranged from 8 to 24 weeks (average, 13.8 weeks). The follow-up survey was, on average, completed 13±11.3 months after surgery, with a range of 3 to 29 months. Surgical outcomes are reported in Table 2. No intraoperative or postoperative complications occurred; specifically, no bleeding events or blood transfusions occurred. No intraoperative or postoperative stenosis of the celiac artery was noted under direct vision, although intraoperative ultrasound was not used in these patients. No celiac artery reconstruction was added to the release. All patients had postoperative duplex ultrasound, and 2 patients had a postoperative CT angiogram, all of whom demonstrated widely patent celiac arteries and no other abnormalities. A decision to limit radiation in children was made, and CT angiography was only used as needed.
Data are mean (standard deviation) values unless indicated otherwise.
US, ultrasonography.
Table 3 shows the breakdown of average self-assessment scores within each category of the CHQ-87 survey as well as average normative values. All preoperative assessments were significantly different from the normative values (P=.03) with the exception of the behavior, emotional role/social limitations, and behavioral role/social limitations categories. In contrast, with the exception of general health perceptions (P=.03), none of the postoperative assessments showed significant deviation from the norm. A significant improvement from pre- to postsurgical scores was observed in the physical functioning (P=.03), mental health (P=.03), and self-esteem (P=.03) categories.
Data are mean (standard deviation) values.
Similarly, a categorical breakdown of the CHQ-PF-50 parental assessment is shown in Table 4. All preoperative scores except for child's behavior were significantly lower than the normative standard (z score range from −2.05 to −3.23). No postoperative categories differed from the norm. There was a significant postsurgical improvement in all categories pertaining to the parent's quality of life (P=.03). A similar improvement was seen in the parent's perception of his or her child's physical functioning (P=.03), bodily pain/discomfort (P=.03), mental health (P=.03), and general health perceptions (P=.03).
Data are mean (standard deviation) values.
Finally, Table 5 compares the common categories between the child's CHQ-87 and the parent's CHQ-PF-50 surveys. The only category to show significant difference between parents and their child was the postoperative mental health assessment. In this category the pre- and postoperative change was statistically higher in the parent's assessment but not in the child's. All other categories showed no statistical difference.
Discussion
When we first considered surgical treatment of a pediatric patient with MALS, we had no objective methods for assessing the extent to which we were benefiting our patients. This assessment was necessary to properly justify a technically demanding procedure that can potentially have great surgical risks. We initiated an Institutional Review Board–approved prospective study assessing outcomes and quality of life for both adolescents and their parents. We present the first series of pediatric patients to have pre- and post-MALS repair quality of life assessment. Our study demonstrated an improvement in physical and psychosocial health following laparoscopic median arcuate ligament release in a pediatric population; this finding has not yet been described in the literature.
MALS continues to be infrequently identified in the pediatric population. One of the contributing reasons for this is that the exact pathophysiological mechanism of pain in MALS is poorly understood. It has been postulated that the pain is neuropathic and that ganglionectomy of the celiac plexus is the appropriate therapeutic choice; however, the more widely held belief is that the pain is due to compression of blood flow in the celiac artery, resulting in ischemia throughout the foregut. This theory has been contested because of the high prevalence (12%–14%) of celiac compression in asymptomatic individuals; however, some have argued that high prevalence in asymptomatic patients is common in other occlusive diseases, such as those involving the femoral artery.9–12 In such cases the diagnosis is considered to be clinically significant and is not dismissed.
Being able to properly diagnose MALS is important in creating an appropriate treatment plan. Unfortunately, the diagnosis is challenging and often one of exclusion. Diagnostic imaging techniques such as CT and magnetic resonance imaging, when inspiration and expiration studies are included, have become more accurate to diagnose MALS. Selective catheter angiography is invasive and technically demanding, making it a less than ideal test for MALS. Lim et al. 13 proposed Doppler ultrasonography as a reliable screening method to detect stenosis of the celiac artery by measuring end-inspiration and end-expiration velocities.
Once a diagnosis is made, choosing the appropriate treatment is also difficult and controversial. The success of endovascular options, such as stenting or angioplasty, in treating mesenteric ischemia has been widely studied and shown to be effective.14,15 Unfortunately, these studies show a higher long-term failure rate for treatment of extrinsic artery compression (such as that seen in MALS), making them second-line options for MALS treatment, even in adults. 16 No studies to date have assessed the use of endovascular techniques in the pediatric population.
Early surgical treatments involved open division of the constrictive ligament. Long-term results were variable, and many believed similar results could be obtained through noninvasive options. 17 Laparoscopic release of the median arcuate ligament was first used in 2000, providing a promising new treatment option that reduces postoperative hospital care and recovery time.4,18
The literature suggests that if an adequate diagnosis is made, laparoscopic release of the median arcuate ligament without additional reconstruction can be successful in reducing symptoms in adults.19–22 Diagnosis in our cohort was limited to the following criteria: experiencing symptoms similar to those reported by Reilly et al., 2 clinical agreement by pediatric gastroenterology, pediatric surgery, and vascular surgery that a diagnosis of MALS is probable, radiological evidence of celiac artery compression via duplex ultrasonography and either CT or magnetic resonance angiogram, and no other contributing diagnoses after an extensive and appropriate work-up. Although properly diagnosing which patients have MALS allows for some interpretation, appropriate selection is essential in choosing the correct treatment plan. Patient selection is the single most important factor contributing to what we think is a successful overall outcome. This is corroborated by the quality of life survey and postoperative radiological evidence.
Postoperative flow rates weeks to months later on duplex ultrasonography were performed on all patients and suggest that laparoscopic repair was successful in producing lasting patency of the celiac artery. Although we used CT angiography on 2 patients, demonstrating a widely patent celiac axis, a decision was made to limit radiation in children, and CT use for surveillance was stopped. We also noted that no patients had any intraoperative stenosis, and no celiac artery reconstruction was required in any of the patients. This is somewhat different than the situation in older adults, who often require a patch or bypass to resolve a residual stenosis. Perhaps the early intervention in adolescents occurs before a fixed stenosis occurs, but this is mere conjecture at this point. We also noticed anecdotally that the adolescents who complained mostly of exercise-induced pain had more significant pain relief after laparoscopic MALS release, but we had no way of capturing this objectively. Regarding technique, we chose an antegrade technique that dissects the celiac artery from the aorta caudally and distally onto the celiac axis as opposed to a retrograde technique dissecting the left gastric artery first and then moving proximally and cranially onto the celiac axis. We attempted the latter retrograde method but found the first antegrade technique much easier. As described in our earlier article, 6 we used intraoperative Doppler ultrasonography neither intraoperatively to guide the dissection nor intraoperatively to check for residual stenosis as we discovered widely patent, normal-appearing celiac arteries in all cases, although we did have intraoperative ultrasonography available at all times.
Our results appear to show that laparoscopic MALS release positively impacted physical functioning, mental health, and self-esteem following treatment. It is interesting that children assessed their pain roughly the same pre- and postoperatively; however, their pain was significantly closer to normative values as a result of treatment. Parents observed an improvement in nearly every category of quality of life in their child. In contrast to the child's self-assessment, parents viewed their child's bodily pain to be better as a result of surgery. Parents' lifestyles were also positively impacted. The emotional involvement and the time consumption their child's condition required were greatly reduced following surgery. Overall, parents and their children agreed on their quality of life evaluations. This consistency further confirms the benefit provided by MALS treatment. This benefit extends from that of the patient to the family as a whole.
Our study has some limitations. Being a tertiary referral center provides our institution with a greater prevalence of patients diagnosed with MALS. Even so, our cohort was small because of the rarity of this disorder. Further study in larger cohorts, although difficult, is necessary to confirm these trends. In addition, we are limited, as all surveys are, by recall bias. However, the preliminary data thus far appear to correlate with our clinical and statistical findings that patients, within our described parameters, may benefit from laparoscopic surgical treatment.
Conclusions
Pediatric MALS symptoms can greatly impact a child's life, and the decision to operate can be difficult. Our preliminary results from a prospective descriptive study demonstrate that laparoscopic median arcuate ligament release for MALS without additional celiac artery reconstruction in the pediatric population is safe and effective and improves overall quality of life for patients and their parents. It is important that no complications were noted and that no residual stenosis was encountered as well. In carefully selected patients, MALS repair not only provides lasting patency of flow within the celiac artery, but also appears to improve physical and psychosocial quality of life for the child and his or her family.
Footnotes
Disclosure Statement
No competing financial interests exist.