
Abstract
Abstract
Background:
We previously reported our experience performing robotic-assisted transhiatal esophagectomy (RATE) in patients with early-stage esophageal cancer who had had no preoperative treatment. The purpose of this report was to determine if RATE could be performed safely with good outcomes for esophageal cancer in a more recent series of patients, the majority of whom were treated with neoadjuvant chemoradiation.
Subjects and Methods:
This was a retrospective review of patients with adenocarcinoma of the distal esophagus or gastroesophageal junction who underwent RATE between November 2006 and November 2012 at a single tertiary-care hospital. Main outcome measures included operative and oncologic parameters, morbidity, and mortality.
Results:
In total, 23 patients underwent RATE, consisting of 20 men and 3 women with a median age of 64 years (range, 40–81 years). The majority of patients (19/23 [83%]) underwent neoadjuvant chemoradiation, although 1 patient had preoperative chemotherapy only, and 3 patients went straight to surgery. Median operative time was 231 minutes (range, 179–319 minutes), and median estimated blood loss was 100 mL (range, 25–400 mL). There were no conversions to open surgery. Complications included seven strictures, two anastomotic leaks, and two pericardial/pleural effusions requiring drainage. One patient required pyloroplasty 3 months after esophagectomy. One patient died from pulmonary failure 21 days after surgery (30-day mortality rate of 4%). The median length of stay was 9 days (range, 7–37 days). Seven of the 19 patients who underwent preoperative chemoradiation had a complete response on final pathology. The mean lymph node yield was 15 (range, 5–29), and surgical margins were negative for cancer in 21 cases.
Conclusions:
RATE can be performed safely with good oncologic outcomes following neoadjuvant chemoradiation in patients with esophageal cancer. This technique has become our choice of operation for most patients with esophageal cancer.
Introduction
O
Robotic technology, with three-dimensional optics, motion scaling, tremor reduction, and multi-articulated arms, can overcome some of the limitations of laparoscopy. 9 Some of the earliest reports of robotic surgery noted that the system provided the greatest benefit for fine manipulations in small spaces, making it an ideal tool in the relatively tight mediastinal space. 10 In 2003, Horgan et al. 11 provided the first case report on robotic-assisted transhiatal esophagectomy (RATE). This report was followed by a series of 18 patients with high-grade dysplasia and T1 esophageal carcinomas where there was no need for preoperative chemoradiation. 12 However, many patients with esophageal cancer present with more advanced-stage tumors requiring neoadjuvant chemoradiation followed by esophagectomy. Bulky tumors and irradiated fields present an additional surgical challenge to an already technically demanding case. This report details our more recent experience performing RATE in 23 patients with adenocarcinoma of the distal esophagus or gastroesophageal junction over a 6-year period, in which a large percentage of patients had undergone preoperative chemoradiation.
Subjects and Methods
Between November 2006 and November 2012, all RATE procedures performed at the University of California San Diego were analyzed. A retrospective review was performed as part of an approved institutional review board protocol.
Each patient received a preoperative workup including endoscopic ultrasound to assess depth of tumor penetration and for the presence of lymph node metastasis. A computed tomography scan of the chest and abdomen and positron emission tomography were also obtained to exclude the presence of metastatic disease. Intraoperatively a diagnostic laparoscopy was performed prior to starting the procedure to confirm the lack of carcinomatosis or occult liver metastases not detected on preoperative imaging.
Operative technique
Informed patient consent was obtained prior to each procedure.
The patient is placed in a supine, split-leg position. Figure 1 depicts the port placement used in each case. A 12-mm trocar is placed in the left upper quadrant, just left of the midline. Two 8-mm robotic trocars are placed in the left and right upper quadrants, and a 10-mm assistant port is placed on the left lateral side. Exposure is obtained using a Nathanson liver retractor.
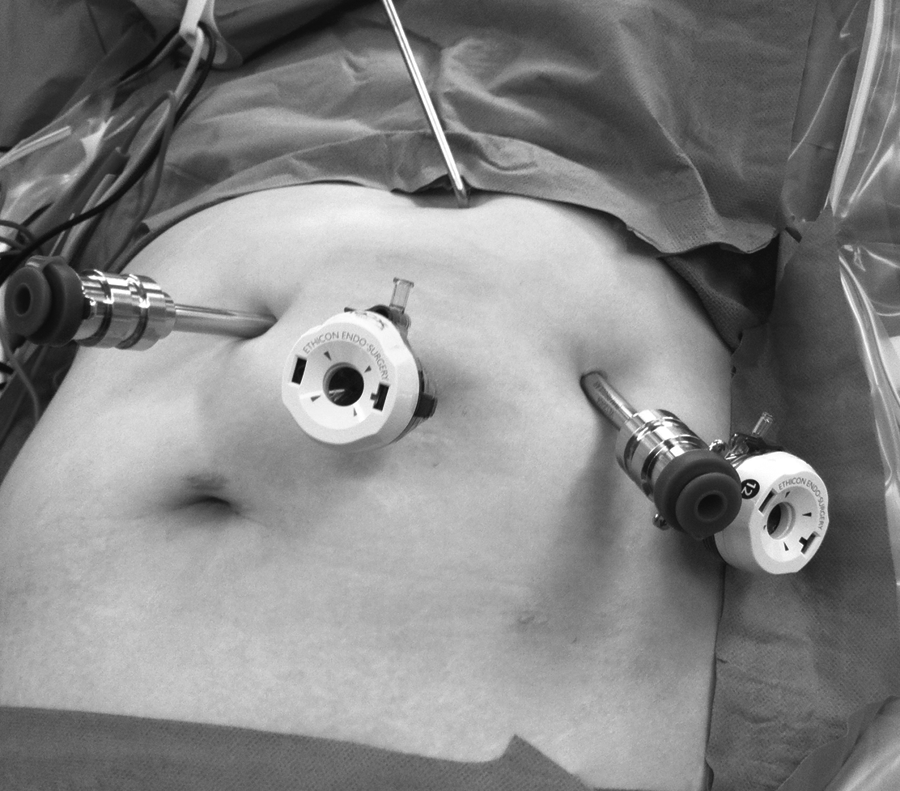
Port placement for robotic-assisted transhiatal esophagectomy.
The initial mobilization and dissection are carried out laparoscopically with the patient in a reverse Trendelenburg position. The short gastric vessels are ligated using an ultrasonic scalpel. Careful dissection of the gastroepiploic artery preserves the blood supply to the neo-esophagus while allowing sufficient length for the gastric pull-up. A complete crural dissection is performed with a combination of blunt dissection and ultrasonic scalpel (Fig. 2). A Penrose drain placed around the distal esophagus allows an assistant to provide critical traction during the procedure. With the stomach retracted superiorly, the left gastric artery is identified and divided with a stapler.
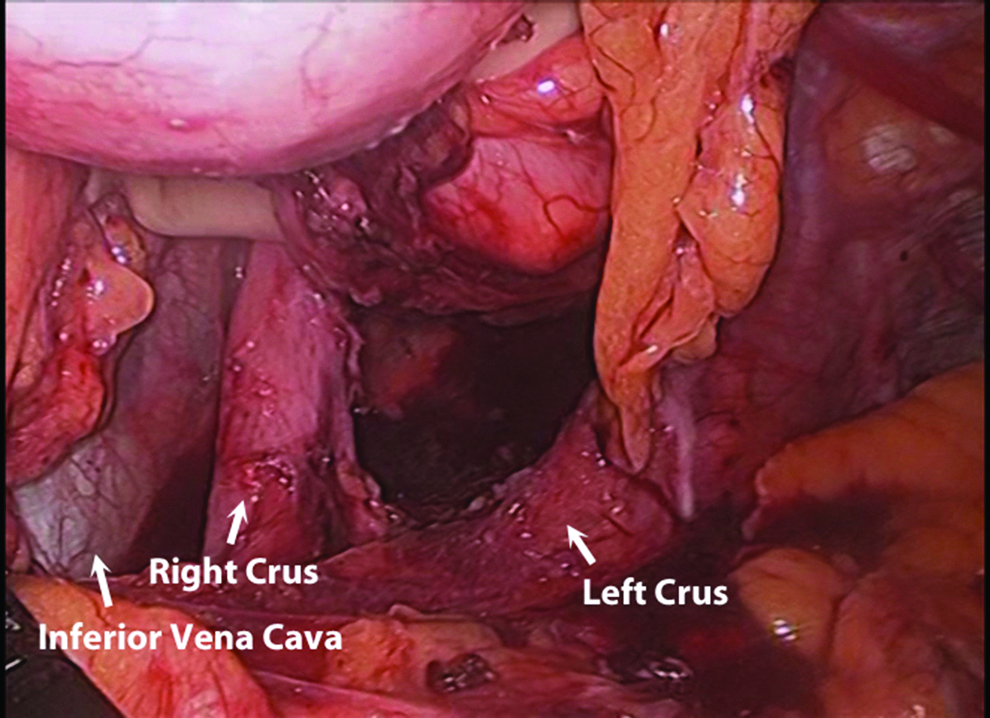
Crural dissection.
The robotic patient cart is then docked, and a circumferential dissection of the esophagus is carried out via the transhiatal access. Care is taken to include all periesophageal tissue and fat and the contained lymph nodes. With care the pleura will not be entered, but if it is, the defect is usually small enough to be closed with a polymer clip. Chest tubes are not routinely placed at the time of surgery and reserved only for cases in which patients develop postoperative symptomatic pleural effusions. Small single defects in the pleura are typically approximated using polymer vascular clips. Once the esophagus is completely mobilized, the azygous vein to the right (Fig. 3) and the aorta to the left (Fig. 4) can be clearly visualized. Following this, a left neck dissection is performed to access the cervical esophagus. Typically, given the proximal extent of the dissection, crepitus is observed in the neck prior to dissection. Care is taken to preserve the recurrent laryngeal nerve.

Mediastinal dissection. The esophagus is rotated toward the patient's left, and the azygous vein is seen on the right.
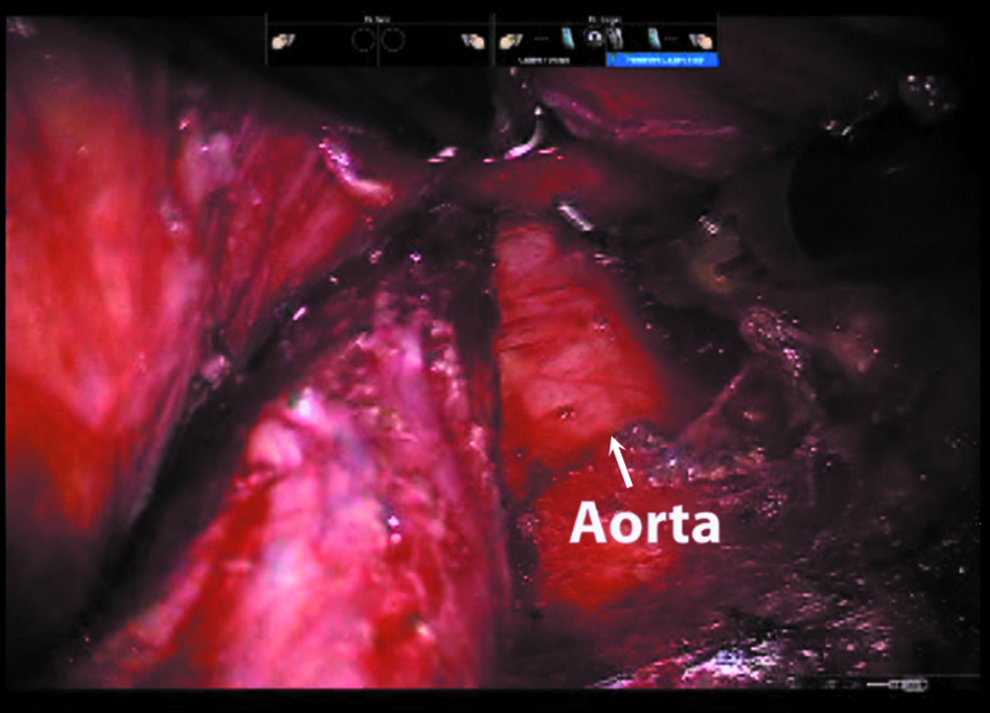
Mediastinal dissection. The esophagus is rotated toward the patient's right, and the aorta is seen on the left.
Laparoscopically, the stomach is then divided along the lesser curvature to create a tube measuring approximately 6 cm in width. The distal extent of the gastric transection is determined by an intraoperative endoscopy at the beginning of the case. We prefer to use staple loads reinforced with a biocompatible copolymer (polyglycolic acid:trimethylene carbonate). We do not routinely perform a pyloromyotomy or pyloroplasty, nor do we place a jejunostomy feeding tube. The specimen is sutured to the remaining stomach for efficiency and to prevent twisting as the gastric conduit is pulled through the mediastinum. A proximal ligation of the esophagus is completed, and the specimen, along with the tubularized stomach, is pulled through the hiatus (Fig. 5). The gastroesophageal anastomosis is completed through the left neck incision. Our preferred method is a side-to-side stapled anastomosis, which was performed in all but 5 patients in this series.
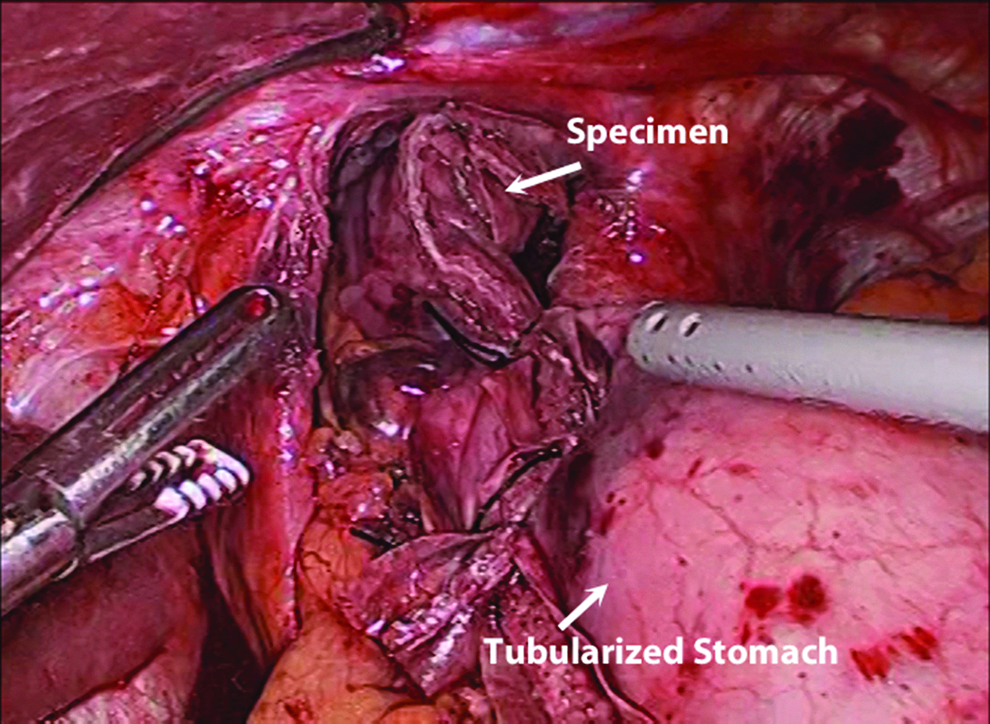
Advancement of the specimen and the tubularized stomach through the mediastinum.
Postoperative care
Patients are routinely extubated in the operating room and transferred to the intensive care unit for continued care. A nasogastric tube is left in place postoperatively for 2–3 days. All patients complete a contrast swallow study on postoperative Day 6, and if no evidence of extravasation is noted, they are advanced to a liquid diet. Following discharge, patients are followed up in the clinic by an oncologic surgeon. Routine imagining is obtained on a regular basis to evaluate for recurrences or disease progression. Upper endoscopy and a swallow study were performed for any patient complaining of dysphagia or extensive nausea and vomiting.
Results
Twenty-three patients with esophageal cancer underwent RATE, consisting of 20 (87%) males and 3 (13%) females. Patient demographics are presented in Table 1. The median patient age was 64 years (range, 40–81 years). Preoperative indication for RATE was biopsy-proven adenocarcinoma in all cases. Table 2 gives endoscopic ultrasound staging distribution. Evidence of nodal involvement was present in 15 (65%) patients preoperatively, and 17 (74%) patients had tumor penetration into adventitia. Neoadjuvant chemotherapy and radiation were used in 19 (83%) patients, chemotherapy alone was used in 1 patient, and 3 patients proceeded directly to surgery given early-stage disease. Two patients had expandable esophageal stents placed preoperatively because of the tumor size and patient dysphagia; these were left in place and removed with the specimen.
ASA, American Society of Anesthesiologists; BMI, body mass index; SD, standard deviation.
The median operating time was 231 minutes (range, 179–319 minutes) with a median estimated blood loss of 100 mL (Table 3). RATE was successfully completed in all 23 patients. Median hospital stay was 9 days (range, 7–37 days) with a mode of 7 days.
Defined as skin incision to skin closure.
Results of pathologic analysis can be seen in Table 4. Negative margins were obtained in 21 (91%) patients. One patient had a positive radial margin, and an additional patient was noted to have tumor cells extending to the distal margin, which was distorted by the staple line, but with gross features consistent with the tumor abutting the margin. Tumor penetrated the adventitia in 5 (22%) patients and the muscularis propria in 5 (22%) patients but was limited to the submucosa in 4 (17%) patients. The remaining 9 (39%) patients had no residual adenocarcinoma present in the esophageal specimen. The mean number of lymph nodes retrieved was 15 (standard deviation, 6). Of the 19 patients who underwent neoadjuvant chemoradiation, 7 (37%) had a complete response (final pathological staging of T0N0).
One patient was noted to have tumor cells extending to the distal margin but with gross features consistent with the tumor abutting the margin. An additional patient had a positive radial margin.
SD, standard deviation.
Complications are outlined in Table 5. The 30-day operative mortality was 4% (n=1). This death occurred in a 63-year-old male who developed acute respiratory distress syndrome and died from respiratory failure on postoperative Day 21. He had followed a standard postoperative course until postoperative Day 6, when his oxygen requirements increased, and he progressed into respiratory failure over the next few days. Despite aggressive diuresis, broad-spectrum antibiotics and antifungals to cover potential sources of infections, and steroids, the patient failed to improve and was given comfort care. As the patient was found to have radiographic evidence of lung disease on preoperative computed tomography scans and no other clear cause of lung disease, the pulmonary critical care team determined the most likely diagnosis with idiopathic pulmonary fibrosis. No other deaths occurred within 30 days of surgery.
Some patients experienced more than one complication and are included in each category.
One in-hospital death occurred from respiratory failure.
One patient had a malignant pleural effusion 8 months after surgery, which we classified as secondary to his disease and not a surgical complication but is included here.
ARDS, acute respiratory distress syndrome; UTI, urinary tract infection.
Surgical complications include anastomotic leaks that occurred in 2 (9%) patients, both of which resolved with nonoperative treatment with total parenteral nutrition and nothing by mouth status. One of these accounts for the longest hospital stay of 37 days as the leak was diagnosed in the immediate postoperative period. A drain was still in place in this patient so no further treatment was needed. The second patient presented with a leak after drain removal and required opening of his wound. Anastomotic stricture, diagnosed endoscopically, was observed in 7 (30%) patients; 5 of these patients were successfully treated with endoscopic dilation alone, and the remaining 2 were successfully treated with dilation and triamcinolone acetonide (Kenalog®; Bristol-Myers Squibb, New York, NY) injections. Delayed gastric emptying was seen in 4 (17%) patients; 2 of these patients had symptom resolution with pyloric dilation and botox injection, and 1 had resolution with dilation alone, whereas the fourth patient required a return to the operating room 3 months after esophagectomy for a pyloroplasty. Three patients complained of dysphagia, without any evidence of anastomotic stricture; 2 of these patients had symptom resolution with endoscopic dilation, and the third patient had been previously diagnosed pharyngeal dysmotility and became jejunostomy tube dependent.
Pulmonary or cardiac complications were observed in 10 (44%) patients. Four patients had postoperative atrial fibrillation. This was intermittent and resolved prior to discharge in 3 patients; the fourth patient required beta-blockade and anticoagulation at discharge. One patient, already described, had acute respiratory distress syndrome and, ultimately, died from respiratory failure. One patient had a pulmonary embolism diagnosed during admission. Aspiration pneumonia occurred in 2 (9%) patients; both were placed on antibiotics, and 1 of these patients developed Clostridium difficile colitis. An additional 2 (9%) patients developed pleural and pericardial effusions that required re-admission for drainage. One of these patients also had recurrent ascites that resolved after paracentesis and medical management with furosemide and aldactone.
The median length of follow-up in the 18 (78%) surviving patients was 7 months (range, 1–29 months). Metastatic disease developed in 6 (26%) patients, 4 of whom have since died, and the remaining 2 are currently receiving chemotherapy for liver metastasis. There have been no local recurrences.
Discussion
The role that robotic technology will play in the future remains a debated subject. Only those procedures that can demonstrate a significant improvement over standard techniques will likely be supported in a cost- and efficiency-driven economy. Our experience demonstrates RATE can be performed with minimal blood loss, similar complications, and shorter length of stay compared to open procedures. Additionally, the shorter operative times associated with RATE compared with laparoscopy offer a significant advantage to the patient and the surgeon while allowing the surgeon to operate from the ergonomically comfortable robotic console.
One of the larger series of RATE published to date, by Dunn et al. 13 in 2012, evaluated the results of 40 patients. Notable complications in their series were a leak rate of 25%, stricture rate of 68%, and recurrent laryngeal nerve paresis rate of 35%. Our results compare favorably to these with a 9% leak rate, 30% stricture rate, and no laryngeal nerve paresis observed. Our mean lymph node retrieval was 15±6, which is similar to their value of 18.5. They reported a slightly higher average operative time of 311 minutes, which still offers a significant advantage over open surgery. These values reflect the efficiency in which the procedure can be performed, as an often-cited concern is the time required for robotic docking, and variations may simply be secondary to the experience of the robotic team.
In 2011, Clark et al. 14 performed a review of robotic-assisted esophagectomy, including both transhiatal and transthoracic approaches. They reported an anastomotic leak rate ranging from 14% to 40%. Galvani et al., 12 in their RATE series of 18 patients, reported a leak rate of 33% and noted they achieved better results when a stapled anastomosis was performed. Our leak rate of 9% is favorable to these published values, and we believe it demonstrates the benefit of a stapled, cervical anastomosis.
It should be noted that our series was completed by a team consisting of an expert robotic surgeon, specializing in esophageal and foregut surgery, and an experienced oncologic surgeon who has performed esophagectomy from various approaches. One of the benefits of robotic surgery is its faster learning curve compared with laparoscopy and the potential to essentially level the playing field. Still, it has yet to be demonstrated that RATE can be adapted by less experienced surgeons with equivalent results. Our hope would be that robotic technology would allow wider access to a minimally invasive approach to what is traditionally a technically challenging operation.
National Comprehensive Cancer Network guidelines suggest that at least 15 nodes should be retrieved to appropriately stage a patient without neoadjuvant chemoradiation. We achieved a mean of 15 nodes in a patient population where 83% had undergone neoadjuvant chemoradiation, a factor known to alter node retrieval. Proponents of a thoracic approach often cite the ability to perform a formal lymphadenectomy. Data have supported, however, that a transhiatal approach is oncologically equivalent to thoracotomy-based procedures but with less morbidity.15,16
A minimum of a 5-year follow-up will be needed before we can compare our survival rates with published values by cancer stage; however, we are encouraged by our results to date. Seven patients are 2 years out from surgery, and of those there is a 57% survival rate. This is comparable to the 5-year rate published by Hagen et al. 2 in one of the most comprehensive analysis of en bloc esophagectomies with systematic lymph node dissections. There have been multiple studies comparing open versus minimally invasive esophagectomy, suggesting an equivalent oncologic outcome and a potentially improved morbidity. 17 This is consistent with our experience.
Having a minimally invasive option in the treatment of this disease allows patients and physicians to work together to choose a modality tailored to their needs. For older patient with multiple comorbidities, an open esophagectomy with a systematic lymph node dissection may be an undesirable option in light of high morbidity, mortality, and lengthy recovery periods. Similarly, the pain and pulmonary complications associated with a thoracic approach, even if the procedure is done laparoscopically, may mean that it is not the best option for many patients. Laparoscopic transhiatal approaches, while offering significant improvements, still have significant limitations, including a steep learning curve. For patients with more advanced tumors who have undergone preoperative chemoradiation and, as a result, have a much more hostile surgical field, we feel a RATE approach offers a significant advantage. We have demonstrated completion of these difficult cases with time efficiency and operative and pathologic outcomes that are similar to those of open transhiatal esophagectomy.
Conclusions
In this single-institution experience, we have found RATE to provide acceptable outcomes in terms of morbidity, mortality, and length of stay, with good oncological outcomes, making this our standard approach to esophagectomy in patients with distal esophageal adenocarcinomas who have undergone preoperative neoadjuvant chemoradiation.
Disclosure Statement
S.H. has received financial compensation for consulting and teaching and an educational grant from Intuitive Surgical in the past. There was no direct financial support for the current study. A.M.C., J.S.B.-G., J.C., G.R.J., B.J.S., M.A.T., and M.B. have no financial conflicts of interest.
Footnotes
Author Contributions
Study concept and design were performed by A.M.C., M.B., and S.H. Acquisition of data was performed by A.M.C., J.S.B.-G., J.C., and S.H. Analysis and interpretation of data were performed by A.M.C., B.J.S., G.R.J., M.A.T., S.H., and M.B. Drafting of the manuscript was performed by A.M.C. Critical review of the manuscript for important intellectual content was performed by J.S.B.-G., J.C., B.J.S., G.R.J., M.B., M.A.T., and S.H. Administrative, technical, and material support was provided by A.M.C., J.S.B.-G., M.A.T., and S.H. Study supervision was performed by B.J.S., G.R.J., M.B., and S.H.