
Abstract
Abstract
Background:
Although the excellent short-term cosmesis after robotic/endoscopic thyroidectomy has been reported, the long-term cosmetic outcome is not yet known. The aim of this study was to evaluate the long-term cosmetic outcome of robotic/endoscopic thyroidectomy.
Patients and Methods:
We compared 147 patients who underwent robotic or endoscopic thyroidectomy using a gasless unilateral axillo-breast (GUAB) approach or a gasless unilateral axillary (GUA) approach with 161 conventional open thyroidectomy patients. Subjective cosmetic outcomes were evaluated using a series of scar-specific questions as well as the Vancouver scar scale at 12–18 months after surgery. The cosmetic satisfaction score was defined as the sum of the two cosmetic satisfaction questions with a rating scale of 1–5. The scar consciousness score was defined as the sum of the four scar consciousness questions with a rating scale of 0–3.
Results:
The cosmetic satisfaction and scar consciousness scores were significantly better in the robotic/endoscopic group than in the open group (P<.001 in both). The cosmetic satisfaction and scar consciousness scores were the same in the robotic and endoscopic groups and were also the same in the GUA and GUAB approach groups. Patients treated by the GUA approach were more satisfied with their scarless breasts than patients treated by the GUAB approach having breast scars.
Conclusions:
Long-term postoperative cosmesis after robotic/endoscopic thyroidectomy using GUAB/GUA approaches is significantly better than conventional open thyroidectomy. In the robotic/endoscopic group, the scarless breasts resulting from the GUA approach lead to greater satisfaction than those after the GUAB approach.
Introduction
T
We have been performing endoscopic and robotic thyroidectomy by a gasless unilateral axillo-breast (GUAB) approach and a gasless unilateral axillary (GUA) approach and have reported on their feasibility, safety, and surgical completeness for benign and malignant thyroid tumors.8–13 Advantages of robotic or endoscopic thyroidectomy over conventional open thyroidectomy include excellent cosmesis and magnified surgical view. It has been reported that functional postoperative voice outcomes are better in robotic thyroidectomy using the GUAB approach than with open thyroidectomy. 14
Excellent cosmetic outcomes of robotic or endoscopic thyroidectomy have been reported by our group and other authors.2–4,8–13,15,17 However, the results were evaluated only a short time after surgery, and the long-term cosmetic outcomes are not yet known. It is better to evaluate cosmetic results in terms of scarring at least 6 months after surgery because the wounds and scars may take 6–24 months to mature. 18 In the present study, we evaluated the long-term cosmetic outcomes of robotic and endoscopic thyroidectomy by a GUAB or GUA approach and compared these with the outcomes of conventional open thyroidectomy.
Patients and Methods
We enrolled 147 patients who had undergone robotic or endoscopic thyroidectomy by the GUAB or GUA approach between August 2009 and May 2011. Of the 147 patients, 119 underwent robotic thyroidectomy (87 by the GUAB and 32 by the GUA approach), and 28 underwent endoscopic thyroidectomy (10 by the GUAB and 18 by the GUA approach). One hundred sixty-one patients who underwent conventional open thyroidectomy in the same period were enrolled as the control group, matching gender and age. No randomization was performed for robotic, endoscopic, or conventional thyroidectomy. Patients were informed about the operative procedures and its advantages and disadvantages, and written informed consent was obtained from all patients. The financial reasons and patient preference have an influence on patient selection bias for some patients. The Institutional Review Board of Hanyang University Hospital approved the study. Both sets of patients completed questionnaires.
The study included patients who underwent thyroidectomy with or without central neck dissection due to benign thyroid nodules or differentiated thyroid carcinoma. We excluded patients who underwent lateral neck dissection along with thyroidectomy and who had types of malignancy other than differentiated thyroid carcinoma. We also excluded patients with a history of neck or breast surgery or irradiation.
The operational techniques of robotic and endoscopic thyroidectomy by the GUA or GUAB approach are described in our previous articles.8–13 Here, we describe only the skin incisions for each procedure briefly. After the lesion-side arm was raised with the patient in the supine position, a 5–6-cm skin incision was made in the axillary fossa, and a second skin incision (0.5 cm [endoscopic] or 0.8 cm [robotic] in length) was made on the circumareolar margin of the breast in the GUAB approach (Fig. 1A). In the GUA approach, a 5–6-cm skin incision was made in the axillary fossa, and a second 5-mm skin incision was made just inferior to the main axillary incision instead of a circumareolar incision (Fig. 1B). A 5–6-cm low collar incision was used for total thyroidectomy or lobectomy in conventional open thyroidectomy.
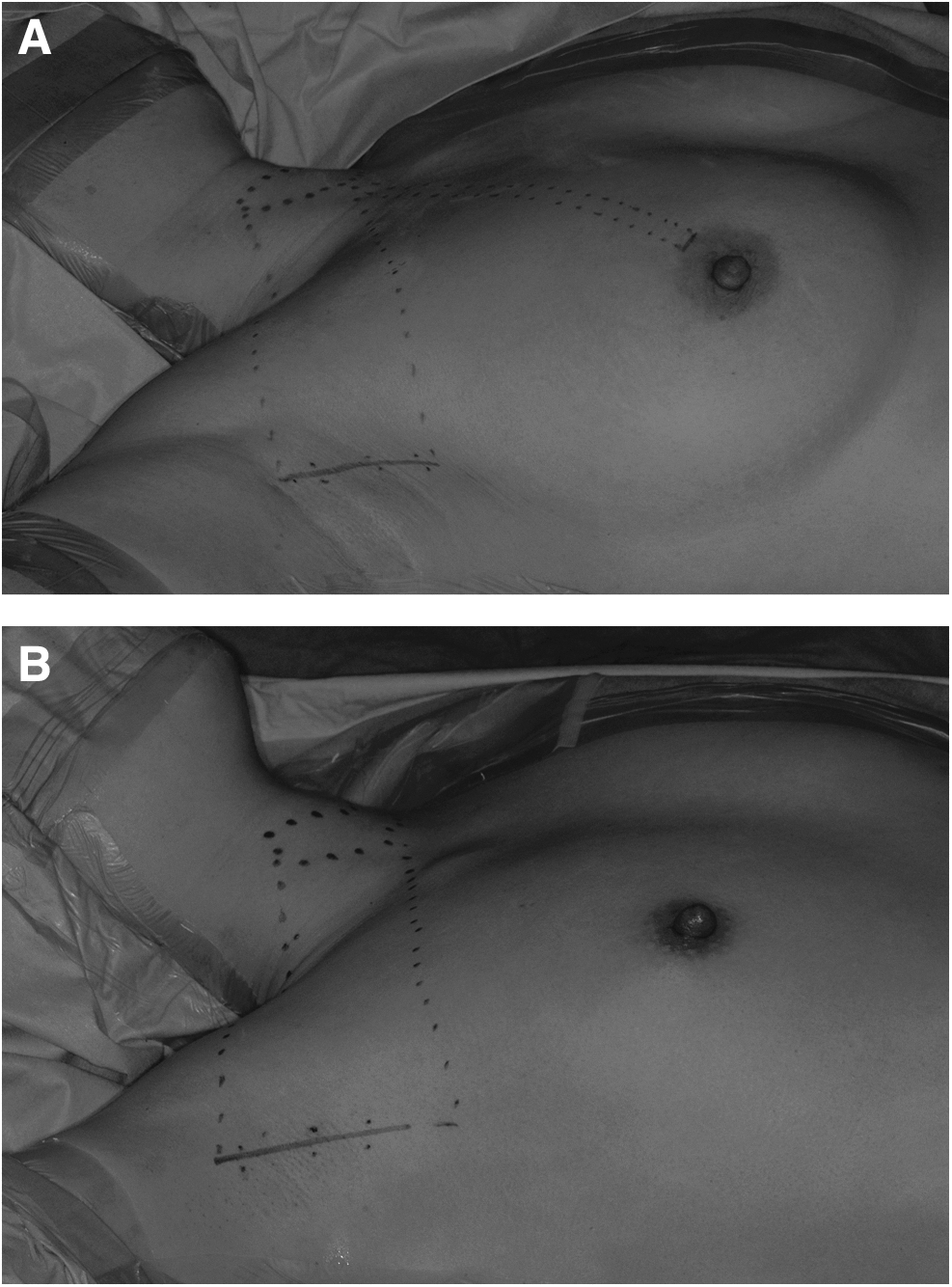
Skin incisions for robotic and endoscopic thyroidectomy.
We developed the questionnaires for the assessment of subjective cosmetic satisfaction and scar consciousness. The cosmetic satisfaction score was defined as the sum of the score of the two questions about the neck scar and the contour of the neck using a verbal response scale ranging from 1 to 5 (corresponding to decreasing satisfaction) (Table 1). For those in the robotic or endoscopic thyroidectomy group, the cosmetic satisfaction questionnaire contained two additional questions about the axilla and breast scar. The scar consciousness score was defined as the sum of the scores of the four questions marked on a scale from 0 to 3 (again of decreasing satisfaction) (Table 2). The survey was performed at 12–18 months postoperatively when the wound and scar had matured and given in a paper survey format at the outpatient clinic. The average survey point score was 15.3±1.78 months after surgery.
We also assessed neck, axilla, and breast scarring at 12–18 months after surgery using the Vancouver scar scale, which was originally developed to assess burn scars and is now widely used for assessing other types of scar.19,20 The Vancouver scar scale consists of four variables: vascularity, pigmentation, pliability, and height. Scores range from 0 to 14, with 0 corresponding to normal skin (Table 3). The scars were assessed by two examiners, and the mean value of the scar score was used.
Statistical analysis
Characteristics of patients and tumors in the robotic/endoscopic thyroidectomy group were compared with patient and tumor characteristics in the conventional open thyroidectomy group using the chi-squared test and Student's t test. The cosmetic satisfaction score and scar consciousness score were compared using the Mann–Whitney U test. We also analyzed the cosmetic satisfaction and scar consciousness scores according to the extent of thyroidectomy, age, and gender. The correlation among the cosmetic satisfaction score, scar consciousness score, and Vancouver scar scale was analyzed using Spearman's correlations. All statistical analyses were performed with SPSS version 18.0 (SPSS, Inc., Chicago, IL). A value of P<.05 was considered statistically significant.
Results
The characteristics of patients and tumors are summarized in Table 4. The robotic/endoscopic thyroidectomy group included 137 women and 10 men, with a mean age of 43.8±8.8 years (range, 23–60 years). The open thyroidectomy group included 150 women and 11 men, with a mean age of 44.2±8.2 years (range, 25–68 years). There were no significant differences in tumor size and pathologic type between the robotic/endoscopic and open group, but more patients underwent total thyroidectomy in the latter (87.6%) than in the former (51.0%).
Data are mean±standard deviation or number (%) values.
CND, central neck dissection; GUA, gasless unilateral axillary; GUAB, gasless unilateral axillo-breast.
Long-term cosmetic satisfaction score
Long-term cosmetic satisfaction results are presented in Table 5. Cosmetic satisfaction with the neck scar (Question 1) and with the neck contour (Question 2) was better in the robotic/endoscopic group (1.42±0.65 and 1.75±0.89, respectively) than in the open group (2.47±0.99 and 2.40±0.89, respectively) (P<.001 in both). (Note that low scores correspond to more satisfactory outcomes.) The cosmetic satisfaction score was better in the robotic/endoscopic group (3.17±1.37) than in the open group (4.85±1.76) (P<.001) and also showed a similar pattern in subgroup analysis based on the extent of surgery, age, and gender.
Data are mean±standard deviation or number (%) values.
Long-term scar consciousness score
Table 6 presents the patients' scar consciousness results for the robotic/endoscopic group and the open group. The questions asked patients about the extent to which they noticed the scar (Question 5), the extent to which they tried to hide their neck (Question 6), how their scar influenced their choice of clothes (Question 7), and how often they thought about their scar (Question 8). Scores were significantly lower in the robotic/endoscopic group than in the open group (P<.05 overall). The scar consciousness score was significantly lower in the robotic/endoscopic group (1.66±2.16) than in the open group (3.09±3.25) (P<.001) and also showed a similar pattern in subgroup analyses based on extent of surgery, age, and gender.
Data are mean±standard deviation or number (%) values.
Vancouver scar scale
The Vancouver scar scale score for the neck (1.41±0.71) was significantly lower than that for the axilla (2.12±0.93) and higher than that for the breast (0.58±0.47) (P<.001 for both). There was a significant correlation between the Vancouver scar scale score for the neck and the cosmetic satisfaction score (Spearman's rho=0.18, P=.040) and scar consciousness score (Spearman's rho=0.21, P=.034) in the open group. In the robotic/endoscopic group, the Vancouver scar scale score for the axilla did not correlate with the cosmetic satisfaction score (Spearman's rho=0.03, P=.79); however, it did correlate with the scar consciousness score (Spearman's rho=0.24, P=.01). The Vancouver scar scale score for the breast did not correlate with the cosmetic satisfaction score (P=.98) or with the scar consciousness score (P=.94) in the robotic/endoscopic group.
Comparison of robotic and endoscopic thyroidectomy
The cosmetic satisfaction scores (3.10±1.25 versus 3.46±1.79, P=.208) and the scar consciousness scores (1.76±2.21 versus 1.25±1.94, P=.225) for the robotic and endoscopic groups were not statistically different. The Vancouver scar scale score for the axilla was significantly higher in the robotic group than in the endoscopic group (2.22±0.92 versus 1.68±0.86, P<.005), whereas the Vancouver scar scale score for the breast was similar for the two groups (0.61±0.55 in the robotic group and 0.55±0.41 in the endoscopic group, P=.59).
Comparison of the GUA and GUAB approaches
The cosmetic satisfaction score (3.24±1.45) and the scar consciousness score (1.60±2.15) for the GUA approach were similar to those for the GUAB approach (3.13±1.33 and 1.70±2.18, respectively) (P=.668 and .789, respectively). Satisfaction with the axillary scar from the GUA approach (2.32±0.87) was the same as that from the GUAB approach (2.44±1.06) (P=.452) (Question 3). However, satisfaction with the breast scar for the GUA approach (1.58±0.63) was significantly greater than for the GUAB approach (2.07±0.78) (P<.001) (Question 4). The answers for satisfaction with the breast scar for the GUA approach were as follows: very satisfied, 25 patients (50.0%); satisfied, 21 (42.0%); and average, 4 (8.0%); there were no dissatisfied or very dissatisfied patients. Answers for satisfaction with the breast scar for the GUAB approach were as follows: very satisfied, 24 patients (24.7%), satisfied, 44 (45.4%), average, 27 (27.8%), and dissatisfied, 2 (2.1%); there were no very dissatisfied patients.
Discussion
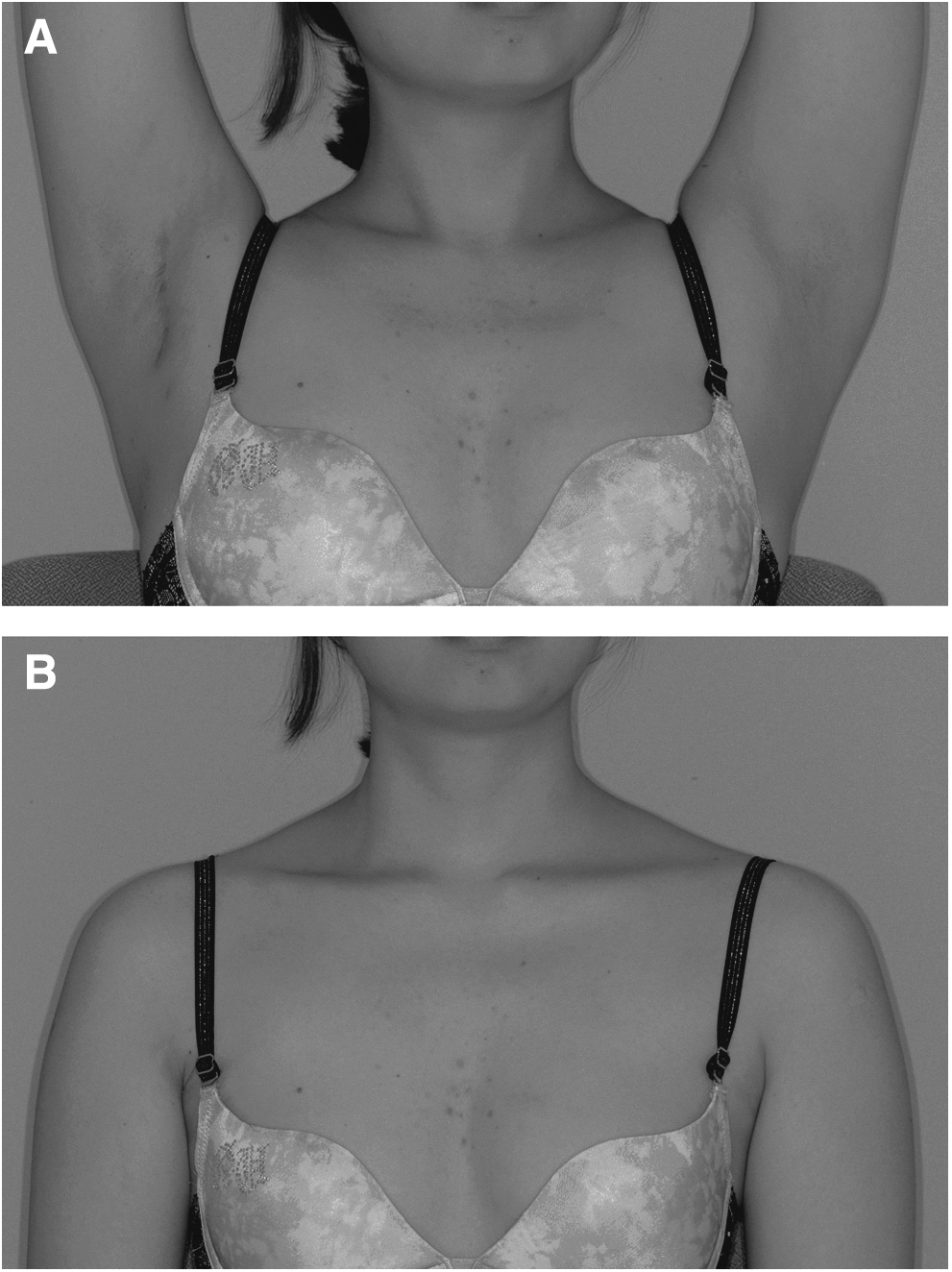
The most obvious advantage of robotic or endoscopic thyroidectomy is the excellent cosmetic outcome (Fig. 2). To our knowledge, this is the first report on the long-term cosmetic results after robotic/endoscopic thyroidectomy, although there are reports on short-term postoperative cosmetic outcomes.
After tissue injury, all wounds undergo the same basic steps of repair, including inflammatory, proliferative, and maturational phases. 18 The maturational phase is a dynamic process. Macrophages release proteases and collagenases, which degrade the immature (type III) collagen, and the wound fills with type I collagen. This process may persist for from 6 months to 2 years after injury. The long-term cosmetic result cannot therefore be evaluated until at least 6 months after surgery. In this study we evaluated the cosmetic results 12–18 months after surgery.
In this study, the cosmetic satisfaction score was significantly better in the robotic/endoscopic group than in the open group regardless of the extent of thyroidectomy, age, and gender. However, it is interesting that in the subgroup analysis based on gender, the men had relatively less interest in their neck scar than the women in both groups.
The long-term cosmetic satisfaction with the neck scar in the current study was slightly better than the short-term cosmetic satisfaction 3 months after surgery that was reported in our previous articles.11,12 These results suggest that cosmetic satisfaction improves as the scar fades over time.
In this study, we also evaluated how conscious the patients were about their scars. In all four questions about scar consciousness, the robotic/endoscopic group was less aware of their scars than the open group. Patients in the open group were more conscious about their neck scar, tried to hide their neck more frequently, and had problems in choosing clothes. These results may suggest that robotic/endoscopic thyroidectomy leads to a better quality of life than open thyroidectomy.
Better cosmetic satisfaction and scar consciousness scores in the robotic/endoscopic group did not depend significantly on age. They were better than in the open group in any age group, although the cosmetic satisfaction score in the patients under 45 years of age (2.97±1.26) tended to be better than that in patients of 45 years of age and above (3.37±1.36) in the robotic/endoscopic group. These results suggest that robotic/endoscopic thyroidectomy can be applied to an older age group.
The Vancouver scar scale score for the neck scar in the open group correlated with the cosmetic satisfaction score and scar consciousness score in this study. A better neck scar provided better cosmetic satisfaction and less scar consciousness. The Vancouver scar scale score of the axilla was higher than that of the neck in this study. This might be because the axillary skin incision site is damaged by tight retraction above the chest wall during robotic or endoscopic thyroidectomy to maintain sufficient working space. The Vancouver scar scale score of the axilla was not related to cosmetic satisfaction about the neck; however, it did correlate with the scar consciousness score in the robotic/endoscopic group. This may be because, although patients are sometimes aware of their axillary scar, they can hide it under their arms. The Vancouver scar scale score of the breast was lower than that of the neck and axilla. This is because the breast incision made at the circumareolar margin was relatively small (0.5–0.8 cm), healed well, and became inconspicuous over time.
We have already reported that there were no significant differences of complications, postoperative pain, and short-term cosmetic satisfaction between robotic and endoscopic thyroidectomy. 12 In the current study, the two groups had similar long-term cosmetic satisfaction and scar consciousness. However, the Vancouver scar score of the axilla was significantly higher in the robotic group than in the endoscopic group. This might be related to the bulky arms of the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA) robot and lack of tactile sensation.
The long-term cosmetic outcomes were excellent in both GUA and GUAB approach groups. In terms of breast scar satisfaction, the GUA approach group yielded a higher degree of satisfaction because of the absence of breast scars. However, in the GUAB approach group, most patients were satisfied with their breast scar, or found it acceptable, and only 2 (2.1%) patients were dissatisfied with their breast scars. This may be because a small breast incision heals well and becomes inconspicuous over time.
There were some limitations to this study. First, the validity of the questionnaire we developed has not been established. However, we think that it is appropriate for assessing cosmetic outcomes after thyroidectomy because it includes questions about neck scar satisfaction, neck contour satisfaction, and scar consciousness, and the questionnaires are easy and rapidly completed. Second, there may have been patient selection bias because there was no randomization among the robotic, endoscopic, and open thyroidectomy groups.
In conclusion, robotic or endoscopic thyroidectomy using a GUAB or GUA approach provides much better long-term cosmetic outcomes than conventional open thyroidectomy. In robotic/endoscopic thyroidectomy, a GUA approach leads to greater satisfaction than a GUAB approach because it results in a scarless breast, although cosmetic satisfaction and scar consciousness are the same for the two groups.
Footnotes
Disclosure Statement
No competing financial interests exist.