
Abstract
Abstract
Introduction:
With an expanding population of patients requiring ventricular assist devices, it is inevitable that these patients will require noncardiac surgery. Ventricular assist devices provide mechanical support for a failing heart either as a bridge to transplant or now as a long-term support if transplant is not available, so-called destination therapy. These devices can add significant technical challenges to abdominal surgery, in that the power supply and drivelines crossing the abdomen can potentially be damaged. The use of preoperative or intraoperative imaging may aid in locating these devices and increase patient safety.
Materials and Methods:
We describe a laparoscopic cholecystectomy in two patients supported with HeartMate® II (Thoratec Corp., Pleasanton, CA) left ventricular assist devices. Our use of fluoroscopic guidance in port placement is also described. A literature review was performed to assess the frequency of laparoscopic procedures performed on patients with similar ventricular assist devices and of complications associated with the device and other comorbidities.
Results:
Laparoscopic cholecystectomy was performed without significant intraoperative hemodynamic changes. The use of imaging, such as fluoroscopy, can identify the location of the ventricular assist device and its associated drive wires to assure they are not damaged intraoperatively.
Conclusions:
Laparoscopic cholecystectomy can be performed safely on patients with ventricular assist devices. Complications due to damage to the device can be avoided with the assistance of fluoroscopy to identify the implanted abdominal portions of the ventricular assist device. Each laparoscopic procedure performed on these patients presents the surgeon with unique obstacles in which careful operative planning and intraoperative monitoring are essential.
Introduction
A
We discuss two cases of laparoscopic cholecystectomy on patients with a HeartMate® II (Thoratec Corp., Pleasanton, CA) left VAD (LVAD) and the use of intraoperative fluoroscopy to identify the abdominal portion of the device.
Clinical Cases
Case 1
The first patient was a 40-year-old male with a HeartMate II LVAD implanted for a 6-year history of ischemic cardiomyopathy who presented to our institution with signs of acute cholecystitis. At the time of initial presentation, he was afebrile (36.6°C), with a leukocyte count of 13.8×109 cells/L. Computed tomography of the chest, abdomen, and pelvis revealed cholelithiasis, with an enlarged gallbladder, and surrounding fat stranding (Figs. 1 and 2). Abdominal ultrasound showed a patulous, sludge-filled gallbladder measuring 11.8 cm in length, which was enlarged from 8.0 cm on previous examination. Cholelithiasis was again confirmed, but no gallbladder wall thickening or pericholecystic fluid was noted on the ultrasound. It was negative for biliary ductal dilatation with the common bile duct measuring 4 mm. The patient was started on broad-spectrum antibiotics and admitted for observation. The patient's leukocytosis worsened to 33.1×109 cells/L. After considering the options of percutaneous drainage versus cholecystectomy, we elected to proceed with a laparoscopic cholecystectomy due to the risk of possible infection of his VAD. The patient's anticoagulation was discontinued and reversed with fresh frozen plasma just prior to the procedure. Upon induction and intubation, necessary monitoring devices were placed, including a radial artery cannula, transesophageal echocardiogram, and a specialized VAD nurse to monitor device function. Mild hypokinetic movements were seen on echocardiogram upon pneumoperitoneum, but no additional cardiac complications were observed.

Radiograph showing the course of ventricular assist device drivelines.

Computed tomography demonstrating enlarged gallbladder and proximity of ventricular assist device drivelines.
Before the patient was prepped, fluoroscopy was used to map the location of the LVAD drivelines. The skin was marked appropriately to avoid damage to the implanted drivelines. The external driveline was prepped and draped out of the field. The patient was then placed in a left lateral decubitus position with his right flank up in order to facilitate a safe cholecystectomy. A right subcostal site was marked, and a small incision was made on the lateral aspect. A 5-mm scope was introduced into a trocar and optically guided into the abdomen. Pneumoperitoneum was then established. The underlying structures were visualized and were without injury. There was obvious inflammation observed in the right upper quadrant and a dark purple-appearing gallbladder consistent with acute gangrenous cholecystitis. An additional 5-mm subcostal trocar was placed under direct vision, with care taken to avoid the marked drivelines. A 12-mm right midabdomen trocar was placed, as well as a 12-mm right lower abdomen trocar placed under direct vision. Again, care was taken to avoid the LVAD drivelines. The gallbladder was then drained of its contents because of its tense nature, and the bile was sent for culture. The rest of the cholecystectomy was carried out in the standard fashion. The patient was hemodynamically stable during the entire operation and in the postoperative period. He was discharged on postoperative Day 4.
Case 2
The second patient was a 68-year-old male with a HeartMate II LVAD implanted for ischemic cardiomyopathy approximately 1 year prior to presentation for septic shock. On admission he was afebrile (36.4°C) and was found to have a leukocyte count of 41.6×109 cells/L. The patient was hemodynamically unstable, was transferred to the intensive care unit, and was started on broad-spectrum antibiotics and pressors. Initial imaging with computer tomography was negative for acute abdominal process. During further workup a gallbladder ultrasound was completed, showing sludge within a mildly prominent gallbladder, wall thickening without pericholecystic fluid, and no common bile duct dilation. A follow-up cholescintigraphy (hepatobiliary iminodiacetic acid) scan was completed, demonstrating no filling of the gallbladder prior to and following morphine augmentation. There was visualization of the biliary tree and duodenum by 10 minutes but still no visualization of the gallbladder after 60 minutes. These findings were consistent with acute cholecystitis. We elected to place a percutaneous transhepatic cholecystomy tube in this patient because of the severity of his critical illness. Within days the patient improved clinically, and his leukocytosis improved. The patient was placed on 6 weeks of intravenous antibiotics, and an interval cholecystectomy was planned.
In the interim, approximately 4 weeks after discharge, the patient had clinically improved but developed bacteremia and was readmitted. VAD infection was suspected, and given the patient's need for cardiac transplantation in the future, we elected to proceed with the laparoscopic cholecystectomy early to enable the patient to have definitive management of his cardiac condition. Again, the patient's anticoagulation was discontinued and reversed with fresh frozen plasma just prior to the procedure.
Before the patient was prepped, the LVAD drivelines were identified using C-arm fluoroscopy. Additionally, a fluoroscopic cholangiogram was performed, which demonstrated flow of contrast into a slightly dilated but otherwise normal-appearing common bile duct and common hepatic duct (Fig. 3). A 10-mm infraumbilical incision was created, and the abdomen was insufflated using a Veress needle. A 10-mm cannula was placed, and initial laparoscopic exploration revealed inflammatory change in the right upper quadrant with edematous tissue planes around the liver with omentum densely adherent to the undersurface of the right lobe of the liver. Additional trocars were placed in the anterior axillary line below the right costal margin, in the epigastrium, and the right upper quadrant. Fluoroscopy was repeated to ensure all trocar sites were well clear of the LVAD drivelines. After the omental adhesions were dissected away, the gallbladder was encountered with a majority of the organ, from the fundus to the infundibulum, grossly necrotic and liquefied. The remaining tissue was dissected away and amputated. The open end of the gallbladder was oversewn after a repeat cholangiogram was performed to visualize the common bile duct. The patient tolerated the subtotal cholecystectomy procedure well and was hemodynamically stable during the entire operation.
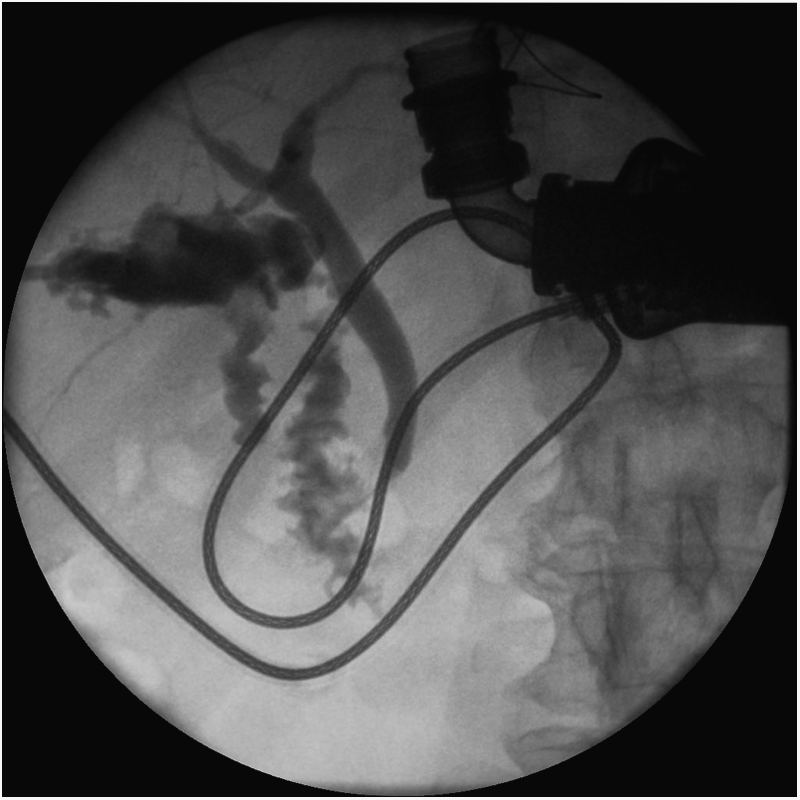
Intraoperative fluoroscopic cholangiogram.
Discussion
Since the Randomized Evaluation of Mechanical Assistance for the Treatment of Congestive Heart failure (REMATCH) trial has shown the use of LVADs in advanced heart failure patients improves quality of life and can provide meaningful survival benefit with a 48% decrease in mortality over medical therapy, the number of patients with LVAD will continue to grow. 1 Many of these patients will be awaiting heart transplant with the LVAD as a bridge to transplant or as “destination therapy” when deemed not a suitable candidate for cardiac transplantation. It is estimated that approximately one-quarter of patients with LVADs will have noncardiac, solid-organ complications requiring surgical intervention. 2 To date there are 25 previously reported cases of laparoscopic surgery successfully performed on patients with VADs, with seven of these procedures being laparoscopic cholecystectomy.3–22
During abdominal operations, certain precautions can be taken to improve the safety of patients with VADs. The use of imaging, such as fluoroscopy, can help to identify the locations of the VAD and its associated drive wires. Fluoroscopy is readily available in most operating rooms and relatively low risk, inexpensive, and efficient for identifying implanted medical devices. Standard port positions for a laparoscopic cholecystectomy may need to be modified to avoid the device, especially the subxiphoid port. Patient position is also important to optimize cardiac return. The reverse Trendelenburg position used in many laparoscopic procedures reduces preload and cardiac output, putting additional stress on the already impaired cardiovascular system. 23 Additionally, the pneumoperitoneum required for laparoscopic surgery can significantly reduce cardiac output and cardiac index. This can be avoided by maintaining intraabdominal pressure lower than 10–12 mm Hg. 22
Infection can also be a concern. Antibiotic prophylaxis in accordance with the usual standard for abdominal surgical procedures was used in our patients. Previous studies have shown that bacterial colonization of a VAD would not be able to be eradicated with antibiotics and that device replacement would be necessary. 24
The most frequently reported complication in these patients is postoperative bleeding due the necessary anticoagulation therapy required for the VAD in order to avoid thromboembolic events.22,25,26 Many of these patients require hospital admission prior to elective operations and conversion from warfarin to heparin anticoagulation, which can be stopped or reversed in the immediate perioperative period. In emergency procedures, such as with these two patients, transfusion of fresh frozen plasma is required to acutely correct the patient's chronic anticoagulation. Some authors have recommended postponing resumption of anticoagulation in these patients to reduce bleeding risk as this has not been shown to lead to an increased number of thromboembolic events. 25 Of the various VADs currently being used, the HeartMate II LVAD has been associated with an extremely low thromboembolic risk and can be managed with less stringent anticoagulation compared with other similar devices. 27 Although our patients' international normalized ratio was elevated preoperatively despite administration of fresh frozen plasma and continued to remain elevated postoperatively, neither had any signs of hemorrhage during the postoperative period. They were both restarted on their oral anticoagulation therapy postoperatively with an intravenous heparin bridge.
Conclusions
Laparoscopic abdominal surgery can be performed safely in patients with VADs. Complications due to damage to the device can be avoided with the assistance of fluoroscopy to identify the implanted abdominal portions of the LVAD. The emergence of VADs represents a viable alternative to transplant for patients with end-stage cardiac disease, and as the number of individuals with these devices grows, the surgical community can expect to see more of these patients requiring noncardiac surgery and must be aware of the challenges afforded. Each procedure performed on these patients presents the surgeon with additional obstacles, and careful operative planning and monitoring are essential.
Footnotes
Disclosure Statement
No competing financial interests exist.