
Abstract
Abstract
Background and Objectives:
The fascial anatomy of the anterior midline of the abdominal wall is permanently altered by the vertical plication of the rectus abdominis muscles commonly performed during abdominoplasty. In order to achieve safe and expeditious peritoneal entry in patients undergoing laparoscopy after a previous abdominoplasty, a modification of the standard midline open technique was developed. This not only facilitates entry and insufflation, but it also provides an acceptable cosmetic result following the laparoscopic surgery.
Materials and Methods:
A modified midline open Hasson technique of laparoscopic peritoneal entry that addresses the anatomical distortion created by a previous midline fascial plication was used in 24 consecutive patients undergoing elective laparoscopic cholecystectomy and is described herein.
Results and Conclusions:
This modified entry technique consistently allowed safe and expeditious peritoneal entry in 24 consecutive patients undergoing laparoscopic surgery after a previous abdominoplasty.
Introduction
V
Previous studies on modified entry techniques in patients who underwent prior abdominal wall reconstruction emphasized midline avoidance for the placement of the initial trocar 4 or used a closed approach with the Veress needle. 5 The feasibility of laparoscopic colectomy without compromising the cosmetic results of a previous abdominoplasty by strategic incision and port placement has also been reported.
A midline open entry technique that takes into account the anatomical changes created by a previous abdominoplasty was developed with the objective to afford reproducibly safe and expeditious peritoneal entry to operators with limited experience in teaching environments. It is a modification of the technique used by and familiar to most general surgeons and is applicable to a variety of procedures. A stepwise, illustrated description of the technique is reported, and the results of its use in 24 consecutive patients undergoing elective laparoscopic cholecystectomy are reviewed.
Technique Description
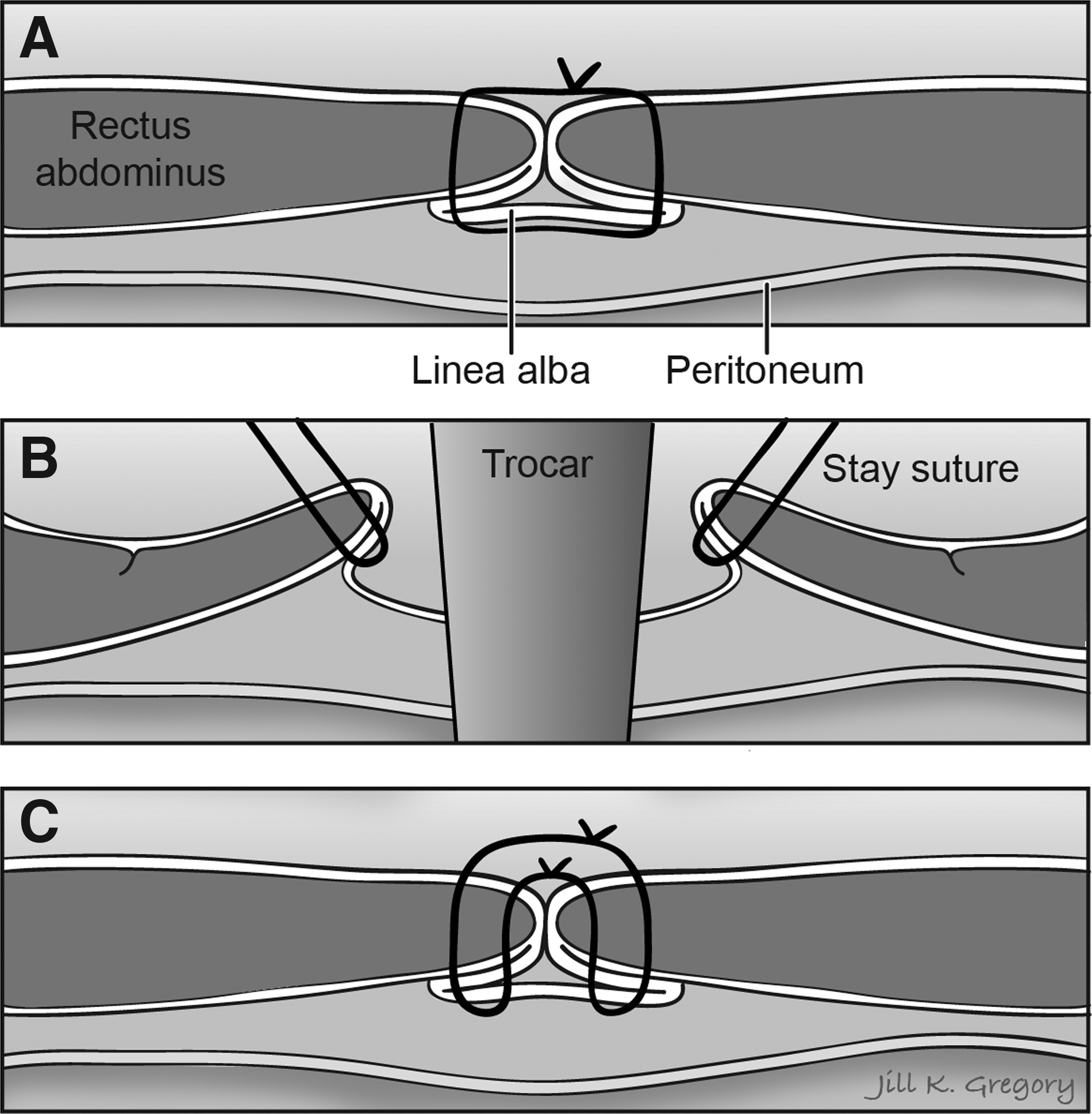
A small skin incision is placed along the existing circumumbilical scar from the previous abdominoplasty and deepened to visualize the fascia, which is then grasped using Kocher clamps placed 5–10 mm on either side of the midline. The fascia is elevated into the wound, applying traction to the Kocher clamps. Using the scalpel, a vertical incision is then made in the fascial plication scar, and any intervening suture material is excised. Both sides of the plication scar incision are secured with stay sutures and retracted with “S” retractors, and the underlying true anatomical midline fascia is visualized and elevated into the wound using again Kocher clamps. This fascial layer is incised vertically with the scalpel and retracted laterally to expose the underlying peritoneum, which is then grasped and incised to introduce a 12-mm Hasson cannula under vision, and then a pneumoperitoneum is established (Fig. 1B). The stay sutures are fastened to the cleats on the Hasson cannula obturator.
At the completion of the laparoscopic phase of the procedure, the Hasson cannula is removed, and the integrity of the fascial plication layer is restored by tying together the stay sutures placed at the beginning of the procedure (Fig. 1C).
Results
Twenty-four consecutive patients with history of a previous abdominoplasty with midline fascial plication, all of them women, underwent elective laparoscopic cholecystectomy. In all the patients, peritoneal entry was gained by a surgical trainee under the supervision of the authors using the technique described herein. All the patients were re-evaluated at 4 weeks after the procedure. There were no intraoperative or postoperative complications.
Conclusions
Midline peritoneal entry under direct vision can be safely and expeditiously achieved with an open technique after a previous midline fascial plication, as long as the anatomical distortion associated with that procedure is taken into account.
Footnotes
Disclosure Statement
No competing financial interests exist.