
Abstract
Abstract
Background:
Although laparoscopic colorectal resection and laparoscopic liver resection have been accepted as effective alternatives to conventional open procedures, there are only a few reports on the clinical availability of simultaneous performance of these two procedures. We report our collective experience of patients with colorectal cancers treated with totally laparoscopic colorectal and liver resection, in comparison with those treated with an open approach.
Patients and Methods:
This study is a retrospective, case-match review of prospectively collected data. Between May 2008 and December 2012, 24 patients with primary colorectal cancer and associated hepatic lesions underwent simultaneous laparoscopic colorectal and liver resection (laparoscopic group). They were matched with patients who underwent an open procedure (open group; n=24 out of 232) based on the types of surgery. Patient demographics, operative details, tumor-related parameters, and postoperative outcomes were analyzed.
Results:
Demographic features and pathologic outcomes were similar in both groups. The median duration of operation was significantly longer in the laparoscopic group than in the open group (290 versus 244 minutes; P=.008), and the median estimated blood loss was larger (325 versus 250 mL; difference not significant, P=.35). However, the time to starting a soft blended diet (3.0 versus 4.5 days; P<.001) and postoperative stay (8.0 versus 10.5 days; P=.001) in the laparoscopic group were both significantly shorter than in the open group. The postoperative complication rate was lower in the laparoscopic group (17% versus 42%; difference not significant, P=.06). The minor complication rate was significantly lower in the laparoscopic group (4% versus 33%; P=.02).
Conclusions:
A totally laparoscopic approach might provide short-term benefits associated with enhanced postoperative recovery despite a longer procedure time and larger blood loss. It can be a reasonable option for simultaneous colorectal and hepatic resection.
Introduction
A
The introduction and development of laparoscopic techniques have contributed greatly to the improvement of short-term outcomes after surgery over the last two decades. Laparoscopic colorectal resection has proven to be safe and effective based on several large randomized trials8–11 and has been accepted as a standard alternative to the conventional open procedure. Although laparoscopic liver resection was started as early as laparoscopic colorectal resection, the widespread dissemination of this procedure has been hampered by its technical difficulties and oncological concern over the transection of a solid organ. More recently, with the evolution of technology and increased experience, laparoscopy for hepatic resection has become an established technique. Hepatobiliary surgeons from selected expert centers have reported laparoscopic liver resection to be safe and feasible, not only for benign disease but also for hepatocellular carcinomas or colorectal liver metastasis.12–16
Simultaneous laparoscopic colorectal and hepatic resection is now an attractive option for treating patients with primary CRCs and resectable SLMs, and several reports have suggested that one-stage operations for such cases can be performed safely.17–20 However, most of these studies have been case series of initial experiences, and there have been too few patients to draw definite conclusions. Here, we have compiled our collective experience of patients with CRCs and associated liver lesions treated with totally laparoscopic colorectal and liver resection, in comparison with cases treated using an open approach.
Patients and Methods
Patients and data collection
This study was a retrospective, case-match review of prospectively collected data regarding a consecutive series of patients with CRCs undergoing simultaneous laparoscopic colorectal and hepatic resection in the Samsung Medical Center (Seoul, Republic of Korea) between May 2008 and December 2012. During the study period, 6574 patients underwent radical resection for a primary CRC, and 297 underwent a simultaneous liver procedure. Of these, 265 cases performed by two separate expert surgical teams—colorectal and hepatobiliary—were included in the study. Minor procedures that did not need the expertise of a hepatobiliary surgeon and could be performed by a colorectal surgeon alone, such as intraoperative liver biopsy or wedge resection of an SLM in the liver's edge, were excluded from analysis. Patients who underwent resection for a CRC and intraoperative radiofrequency ablation (RFA) without liver resection were also excluded.
Finally, 24 cases of simultaneous laparoscopic colorectal and hepatic resection and 232 cases of a totally open procedure were identified. The 24 laparoscopic cases were matched with open cases at a ratio of 1:1, based on the types of colorectal and hepatic surgery (Fig. 1). After cases were matched by operation name, additional parameters were taken into account sequentially: age, body mass index, and gender. Other parameters were not taken into consideration while doing the matching. When the number of patients selected for the control group with the former criteria exceeded that in the intervention group, inclusion/exclusion was determined randomly. Patient demographics, operative details, tumor-related parameters, and postoperative outcomes were investigated in each patient. Postoperative complications and mortality were defined as events occurring within 30 days after surgery. The institutional review board of Samsung Medical Center approved this study.
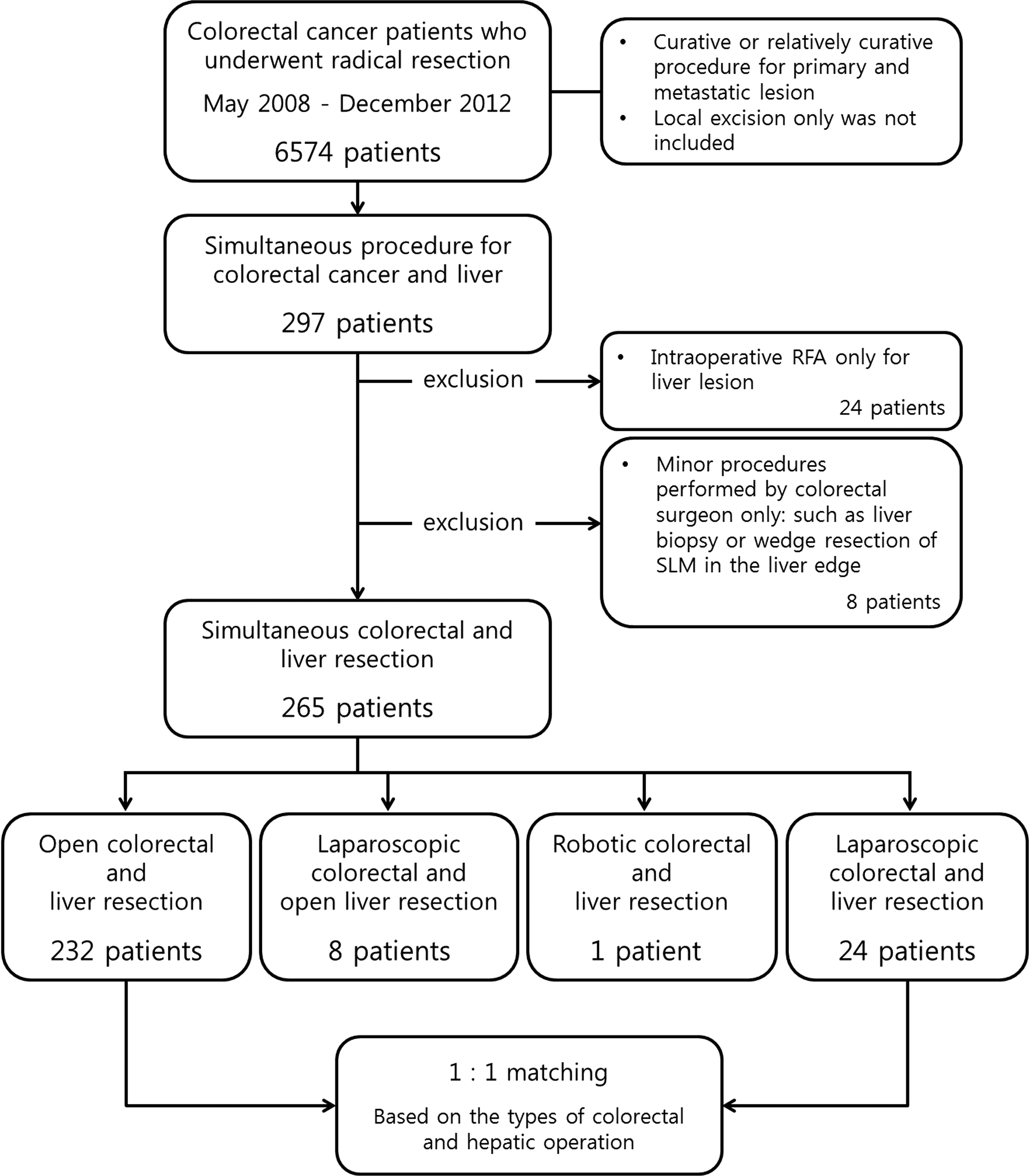
Schema of the patient selection flow according to inclusion/exclusion criteria. RFA, radiofrequency ablation; SLM, synchronous liver metastasis.
Preoperative staging and decision to perform liver resection
Confirmation of the colonic pathology via colonoscopic biopsy was done for all the patients before it was decided whether to perform surgery. All patients underwent preoperative chest and abdominopelvic computed tomography (CT) scans. Whole-body positron emission tomography scanning was used selectively in some patients. Rectal magnetic resonance imaging was performed when the primary CRC was located in the rectum. Liver magnetic resonance imaging was performed in most cases to identify additional hidden metastases that were not found in CT scans. Preoperative liver biopsies were not performed routinely because of the risk of tumor dissemination during the procedure.
Expert hepatobiliary surgeons served as members of a multidisciplinary committee in determining the resectability of the disease and operating methods. In all cases of a primary CRC with resectable SLMs, a synchronous resection was considered. Additional RFA was considered as an option to reduce the extent of hepatectomy or in selective cases with bilobar disease. Because of the retrospective nature of the study, the selection criteria for simultaneous laparoscopic procedures were not determined strictly and changed as time went by. In the early phase, we carefully selected patients with a unilobar hepatic metastasis as this requires a less intense hepatic procedure (i.e., left lateral sectionectomy), without a need for simultaneous resection of the other side of the liver or intraoperative RFA. However, after several successful cases, the indications were extended to that of conventional laparoscopy of each procedure.
Surgical technique
Colorectal resection with complete abdominal exploration always preceded liver resection or RFA. Intraoperative ultrasonography was not performed routinely because most of the patients were evaluated preoperatively with gadolinium-enhanced magnetic resonance imaging scans of the liver. Two separate expert surgical teams performed all procedures. Each team was composed of one or more experienced attending physicians from the colorectal or hepatobiliary departments.
For dealing with the primary CRC, the principles of cancer surgery, which include en bloc resection, adequate lymphadenectomy with ligation of the lymphovascular pedicles, and the establishment of clear resection margins, were used for both open and laparoscopic approaches. A conventional five-port technique, reduced-port technique, or single-incision laparoscopic technique was applied to the procedures for CRCs in the laparoscopic group, and no hand-assisted laparoscopy was included.
For liver resections, a sling could be secured around the hepatoduodenal ligament in preparation for a Pringle maneuver, although this was not performed routinely. An extra-Glissonian approach with division of the pedicles using a linear cutting vascular stapler or ligation between Hem-o-lok® clips (Teleflex®, Research Triangle Park, NC) was used for laparoscopic anatomical resections including hemihepatectomy and sectionectomy. Nonanatomical resection included bisegmentectomy or segmentectomy and nonanatomical subsegmentectomy. Parenchymal transection was performed using a Cavitron ultrasonic surgical aspirator (Tyco Healthcare, Mansfield, United Kingdom). A harmonic ACE® ultrasonic dissector (Ethicon Endo-Surgery, Cincinnati, OH) and bipolar coagulator were added in the laparoscopic group of patients. All laparoscopic liver resections were performed totally laparoscopically, without hand assistance. Resected specimens were extracted through an extension of the umbilical port site or via a Pfannenstiel incision, which was also used for the intestinal specimen extraction and anastomosis. In all of the patients treated with RFA, complete necrosis of the liver metastasis was confirmed by intraoperative ultrasonography and postoperative CT scans within 1 week after the procedure.
Conversion to an open operation was defined as an abdominal incision larger than that needed for specimen retrieval.
Statistics
The data were analyzed using SPSS version 19.0 software (IBM SPSS Statistics, Armonk, NY). Continuous variables are presented as median (range) values. They were analyzed using the Mann–Whitney nonparametric U test. Categorical variables are presented as the number (percentage), and chi-squared and Fisher's exact tests were used for their analysis. Results were considered statistically significant at P<.05.
Results
Patient characteristics
The demographic and clinicopathological characteristics for all 48 patients are listed in Table 1. The laparoscopic and open groups were similar in terms of age, gender, body mass index, American Society of Anesthesiologists grade, and history of abdominal surgery. The location of the primary CRC and the numbers of liver lesions were not significantly different between the groups. Although there was a trend of having bilobar disease in the open group, this did not reach statistical significance.
ASA, American Society of Anesthesiologists; BMI, body mass index; OP, operation.
Surgical procedures
Because the patients were matched according to the types of colorectal and hepatic operations that they underwent, the surgical procedures of the two groups were almost identical (Table 2). However, 1 more patient in the open group underwent low anterior resection and needed a diverting ileostomy. Additional intraoperative RFA was performed in 1 patient in the laparoscopy group and in 2 patients in the open group. Five and 4 patients in the laparoscopic and open groups, respectively, underwent simultaneous procedures to other organs, in addition to colorectal and hepatic resection. In the laparoscopic group, these included one excision of seeding nodules in the pelvic cavity, two unilateral salpingo-oophorectomies, one uterine myomectomy, and one partial cystectomy. In the open group, there was one incidental appendectomy, one unilateral salpingo-oophorectomy, one bilateral salpingo-oophorectomy and appendectomy, and one transabdominal hysterectomy and bilateral salpingo-oophorectomy. All patients in the laparoscopic group underwent simultaneous colorectal and hepatic resection successfully, without conversion to open or additional incisions.
RFA, radiofrequency ablation.
Pathological outcomes
The pathology parameters were similar between the laparoscopic and open groups (Table 3). The T stage, N stage, and size of the primary CRC were not significantly different between the groups. Other pathological outcomes such as the proximal resection margin, distal resection margin, and number of harvested lymph nodes were similar in both groups and generally at an acceptable level. Circumferential resection margins were examined in all cases of left-sided CRCs (21 patients in each group), and one was presumed to be positive in a patient in the laparoscopic group with a circumferential resection margin of <1 mm. The patient had a huge rectosigmoid colon cancer and underwent partial cystectomy in addition to colorectal and hepatic procedures because of direct invasion by the tumor.
Among the patients in the laparoscopic group, 2 did not have an SLM. One of them had two possible metastatic lesions in segment VI of the liver and underwent laparoscopic nonanatomical subsegmentectomy of the liver with anterior resection of the colon; the histopathology report revealed that they were eosinophilic abscesses. The other patient was a carrier of hepatitis B virus and was presumed to have a viable hepatocellular carcinoma with a typical image finding. He also underwent laparoscopic nonanatomical subsegmentectomy of the liver in addition to right hemicolectomy for biopsy-proven ascending colon cancer. As for the rest, every patient had an SML with a primary CRC. The maximal diameter of SLM nodules was similar between both groups. Negative resection margins for liver resection were achieved in all cases.
Perioperative outcomes and postoperative complications
Table 4 lists comparisons of perioperative outcomes and postoperative complications between the two groups. The median duration of operation was significantly longer in the laparoscopic group (290 minutes; range, 283–551 minutes) than in the open group (244 minutes; range, 149–375 minutes; P=.008). The median estimated blood loss was greater in the laparoscopic group (325 mL; range, 50–900 mL) than in the open group (250 mL; range, 50–850 mL). However, the difference did not reach significance (P=.35).
One patient developed ileus and superficial surgical site infection (SSI) at the same time.
Regarding postoperative recovery, the times to the first bowel movement and a soft diet and the length of postoperative hospital stay were compared. The time to the first bowel movement was defined as the moment when the patient recognized the first flatus or stool passage via the anus or stoma and was not significantly different between the groups. Times to resume a soft diet and length of postoperative stay were significantly shorter in the laparoscopic group (both P<.001).
The overall complication rate was lower in the laparoscopic group (17% versus 42%), but the difference did not reach statistical significance (P=.06). The postoperative complications were graded according to the Clavien–Dindo classification. 21 In the laparoscopic group, major complications (Grades III and IV) occurred in 3 patients (12%). Two patients developed anastomosis leakage and underwent laparoscopic exploration with a diverting ileostomy formation on their fourth postoperative day. Another patient developed bile leakage and needed intervention to drain it. In the open group, 2 patients (8%) suffered from the major complication of an anastomosis leakage. One of them underwent explorative laparotomy with a diverting ileostomy formation on the sixth postoperative day. The other patient already had a diverting ileostomy, and the accumulated fluid in his pelvis was controlled with an interventional drainage procedure. The major complication rate was not significantly different between the two groups. However, minor complications (Grades I and II) were significantly less frequent in the laparoscopic group (P=.02). There were no intraoperative complications or postoperative mortalities.
Discussion
Laparoscopic surgery, which was designed to reduce the surgical stress and pain associated with large incisions, has been shown to improve short-term outcomes and to give similar long-term outcomes to many kinds of surgical procedures. Laparoscopic colorectal resection was started in the very early days of laparoscopy and has been accepted as a standard treatment option, even for advanced lesions.8–11 In contrast, laparoscopic liver resection did not become widespread until quite recently. Concern over potential uncontrollable bleeding, air embolisms, inadequate oncologic resection, loss of the tactile sense that can help to identify intraparenchymal lesions, and the lack of minimally invasive skills acquired by hepatobiliary surgeons have slowed the development of laparoscopic liver resection techniques. Nevertheless, with accumulated experience, hepatobiliary surgeons from selected expert centers started to report liver resections via laparoscopy. Studies on thousands of cases of laparoscopic liver resections concluded that laparoscopy was associated with lower morbidity, less pain, a faster recovery, and a shorter hospital stay than open procedures, without compromising oncologic clearance.12–16
The optimal surgical timing for resectable SLMs remains controversial. Earlier reports recommended a staged approach with initial resection of the primary CRC followed by hepatic resection 2 or 3 months later.22–24 However, we prefer a synchronous procedure if the hepatic lesion is resectable, based on increasing evidence of the safety and feasibility of simultaneous hepatectomy with colorectal resection.5–7 At first, simultaneous resection was performed in an open manner. When the primary CRC was located in the right colon, the skin incision was not extended much. However, for patients with cancers of the sigmoid colon and rectum, a long midline incision was inevitable. Subsequently, some surgeons combined a laparoscopic colorectal resection with an open procedure for the liver, as reported by Huh et al. 25 However, this technique also left a large scar in the upper abdomen, and the advantage of laparoscopy was not realized fully.
Simultaneous laparoscopic resection of the primary CRC and associated liver lesions was first performed in our center in June 2008. Since then, we have conducted 24 consecutive cases of simultaneous laparoscopic colorectal and hepatic resection, including major hepatectomy: six hemihepatectomies and nine sectionectomies.
Our data have confirmed the well-known benefits of laparoscopic surgery for simultaneous colorectal and hepatic resections. Despite a longer operation time and greater blood loss, postoperative recovery was clearly faster in the laparoscopic group than in the open group; these patients resumed a soft diet earlier and were discharged 2 days sooner on average than those in the open group. The overall complication rate was 17% in the laparoscopic group and 42% in the open group, but the difference did not reach statistical significance. It is interesting that, after grading according to the Clavien–Dindo classification, the result changed statistically. Whereas the incidence of major complications was similar in both groups, the minor complication rate became significantly different. Most of the minor complications occurring in the open group were superficial surgical site infections and adhesive ileus, which seem to be strongly related to the presence of a bigger wound.
There were some limitations in this study. Because of the retrospective nature, we could not exclude the possibility of selection bias. Moreover, as with all reported studies of this approach, the number of patients in the laparoscopic group was small. Because of the types of colorectal and hepatic operations alter the difficulty of surgery materially, we thought that stratifying the study population for all potentially prognostic factors should be preceded by matching the procedures. Although the numbers in the control group seemed large enough, after matching by procedures, they were insufficient to try certain stratifying methods such as propensity score matching.
Nevertheless, although limited, our experience suggests that simultaneous laparoscopic colorectal and hepatic resection is safe and feasible with acceptable pathology parameters. Moreover, the comparisons of perioperative outcomes and postoperative complications between the two groups showed that the general benefits of laparoscopy were well maintained in this long and extensive procedure.
In conclusion, within the limits of a retrospective study analyzing a relatively small sample of highly selected patients, this study showed that a totally laparoscopic approach was a reasonable option for simultaneous colorectal and hepatic resection. It might provide short-term benefits associated with enhanced postoperative recovery and reduce the minor complications associated with the presence of a large surgical wound. It could provide an alternative to open procedures when performed by an expert surgical team, composed of experienced colorectal and hepatobiliary surgeons.
However, further long-term follow-up studies and large-scale verifying studies for confirming the safety of simultaneous laparoscopic colorectal and hepatic resection are needed.
Footnotes
Disclosure Statement
No competing financial interests exist.