
Abstract
Abstract
Laparoscopic-assisted distal gastrectomy (LADG) with D2 resection is gradually being performed for treating advanced gastric cancer. This meta-analysis aims to compare the clinical outcomes between LADG and open distal gastrectomy (ODG) when considering the impact of the learning curve. The PubMed, Embase, and ISI databases and the Cochrane Library were electronically searched. Randomized controlled trails and retrospective comparative studies published between 1994 and 2013 were collected. We divided the included studies into two subgroups according to whether the authors had experience of at least or fewer than 40 cases of LADG with D2 resection and then compared the operative time, intraoperative bleeding, the amount of resected lymph nodes, short-term recovery parameters, and complications between LADG and ODG groups. Ten comparative studies including 1100 patients were selected. Meta-analysis showed that when LADG was compared with ODG, surgeons with experience of at least 40 cases could achieve more resected lymph nodes (P=.002), reduced time to flatus (P<.0001), shortened time to liquid diet (P<.00001), and lower complication rates (P=.02). However, the above advantages of LADG faded in the subgroup of surgeons with experience of fewer than 40 cases. Our meta-analysis suggested that the learning curve has significant effects on most of the important surgical and short-term recovery outcome parameters. Accomplishment of 40 cases of LADG with D2 lymphadenectomy is required to achieve optimum proficiency.
Introduction
S
In the past decade, several centers have reported the application of LADG with extended lymphadenectomy (D2) in patients with advanced gastric cancer.5–7 However, there are still two very important practical barriers that have precluded the full acceptance of LADG with D2 resection as an alternative to open distal gastrectomy (ODG). First, the difficulty in attaining adequate lymph node dissection under laparoscopic view may cause insufficient en bloc resection, especially for the node-positive cases. 8 Second, whether laparoscopic D2 resection results in intra- and postoperative complication rates comparable to those of ODG is also unclear.
The learning curve is an important issue to consider when evaluating the influencing factors of short-term outcomes of LADG. It is generally accepted that surgeons who are qualified in performing LADG with D1 resection should have experienced laparoscopic gastrectomy in at least 30 cases to overcome the learning curve.9–11 When it comes to laparoscopic D2 surgery, it might be much more difficult for beginners to have a continuous experience accumulation of important steps, including controlling instruments, regulating operation fields, and vascular skeletonization, during their training period. Until now, unfortunately, there have been few published randomized controlled trials (RCTs) specifically focused on the safety and efficacy of LADG with D2 lympadenectomy for advanced gastric cancer, not to mention the effect of the learning curve on the operative procedure and patients' recovery. In view of this, we performed a meta-analysis aiming to address the impact of the learning curves of laparoscopic D2 gastrectomy on short-term outcome parameters. We divided the included studies into two subgroups according to the status of surgeons' experiences and compared the operative time, intraoperative bleeding, resected lymph nodes, short-term recovery parameters, and complications between LADG and corresponding ODG groups.
Materials and Methods
Literature search
We followed QUOROM guidelines for conducting meta-analysis. 12 Two investigators (D.Z. and J.W.) performed a systematic literature search independently by using the PubMed, Embase, and ISI databases and the Cochrane Library Central between January 1994 and May 2013. The search strategy was based on the following medical subject heading terms: “stomach neoplasm,” “gastrectomy,” “comparative study,” “randomized controlled trials,” “clinical trial,” “minimally invasive,” and “laparoscopy.” The related articles function and reference lists were used to broaden the search. The investigators and experts in laparoscopic surgery ensured that all potentially relevant reports were identified. No restriction was set for languages or date of publication. When further information was required, the corresponding authors of relevant articles were contacted by the reviewers.
Data extraction
The above two investigators performed the data extraction independently, and in the case of discrepancy, the decision was made by mutual consensus. A data abstraction was carried out to record details of first author, year of publication, study type, patient characteristics, preoperative diagnosis, sample size for either technique, extent of lymphadenectomy, type of gastrointestinal reconstruction, and conversion rate from LADG to ODG. The following outcome parameters were collected: the operative time, intraoperative bleeding, the amount of resected lymph nodes, time to first flatus, time to liquid diet, postoperative hospital stay, complications, and short-term mortality.
Inclusion criteria
1. Study design: RCTs and nonrandomized comparative studies
2. Target population: patients with advanced gastric carcinoma located in the middle or lower part of stomach, no evidence of local and distant metastasis on preoperative examination, no preoperative treatment including chemotherapy, radiotherapy, etc.
3. Main purpose: comparing the short-term outcomes of LADG and ODG with D2 resection
4. Availability of quantitative data on the outcome parameters listed below
5. When several studies reported on the same patient data or studies originated from the same institution, we selected the one of the best quality or the most recent publication.
Exclusion criteria
1. Studies included patients who received total or proximal gastrectomy.
2. Studies in which other laparoscopic approaches were used such as totally laparoscopic technique, hand-assisted laparoscopic procedure, and robotically assisted surgery
3. Studies in which the outcome measures of interest were not reported or the related data were impossible to calculate from the published articles
4. Studies in which the LADG and ODG were not equivalently matched in terms of age, sex, depth of tumor invasion, and extent of lymphadenectomy
5. Studies that only focused on LADG with D1 or D1+ lymphadenectomy
Outcomes of interest and definitions
The total number of retrieved lymph nodes was recorded for evaluating the power of tumor clearance. The total incidence rate of various complications was calculated. Surgical complications included organ injury, bleeding, anastomotic complications, fistula, lymphorrhea, ileus, gastrasthenia, dumping syndrome, abdominal abscess, bowel volvulus, ascites, epididymitis, enterocolitis, pancreatitis, and wound infection. Pneumonia, pleural effusion, and cardiocerebral vascular complications were classified as nonsurgical complications. The definition developed for “short-term mortality” was the incidence of death in the hospital or 30-day mortality after the operation.
Subgroup analysis
Subgroup analysis was performed by dividing the overall cohort into the following two study groups in order to determine whether the learning curve had an effect on the outcomes: Group 1 (the surgical team had had experience of at least 40 cases of LADG with D2 resection) and Group 2 (the surgical team had had experience of fewer than 40 cases of LADG with D2 resection).
Assessment of methodological quality
The quality of included studies was assessed using the modified Newcastle–Ottawa Scale for all the included studies. 13 Studies with more than 5 stars were considered as high-quality studies.
Statistical analysis
Weighted mean difference (WMD) with its corresponding 95% confidence interval (CI) was used for the analysis of continuous variables. To calculate WMD, we extracted the data of mean and standard deviation (SD) provided by the authors. Values in the form of standard error (SE) were converted to SD according to the following formula: SE=SD/
Owing to the between-study variability of sample size, surgical intervention, and perioperative management, overall estimates were calculated by using the random effect models. 18 Quantitative assessment of heterogeneity was explored by the chi-squared test with significance set at a P value of .10 and was measured using the I2 statistic. Egger's test and graphical test with Begg's funnel plot were used to detect the publication bias. 19 A two-sided P value of <.05 was considered statistically significant.
SAS version 9.13 software (SAS Institute, Cary, NC), Review Manager version 5.2 software (Cochrane Collaboration, Software Update, Oxford, United Kingdom), and Intercooled Stata version 7.0 for Windows software (StataCorp, College Station, TX) were used for conducting this meta-analysis. Medcalc version 12.7.7.0 software (MedCalc Software, Ostend, Belgium) was used to perform receiver operator characteristic (ROC) curve analysis in order to state that the “threshold of 40 cases” was the optimal experience. The cutoff point was calculated using SAS version 9.13 software.
Results
Description of studies
The two investigators had 100% agreement on the data extraction. The strategy of study selection is displayed in Figure 1. As outlined in Table 1, there were no RCTs available. Ten comparative studies published between 2005 and 2013 were eligible for meta-analysis.19–28 These studies involved 1100 patients, of whom 497 received LADG and 603 underwent ODG. Five studies were published in the most recent 3 years. The techniques for gastrectomy with D2 lymphadenectomy used in all included studies were similar. Among the 10 studies, five studies were reports from centers that had experiences of more than 40 cases of LADG with D2 surgery, whereas the remaining five were their initial studies on laparoscopic D2 surgery (Table 2). With regard to quality assessment, the agreement on scoring of individual studies was high (weighted κ=0.89). According to the Newcastle–Ottawa scoring system, all of the 10 included studies were classified as high-quality studies (Table 3).
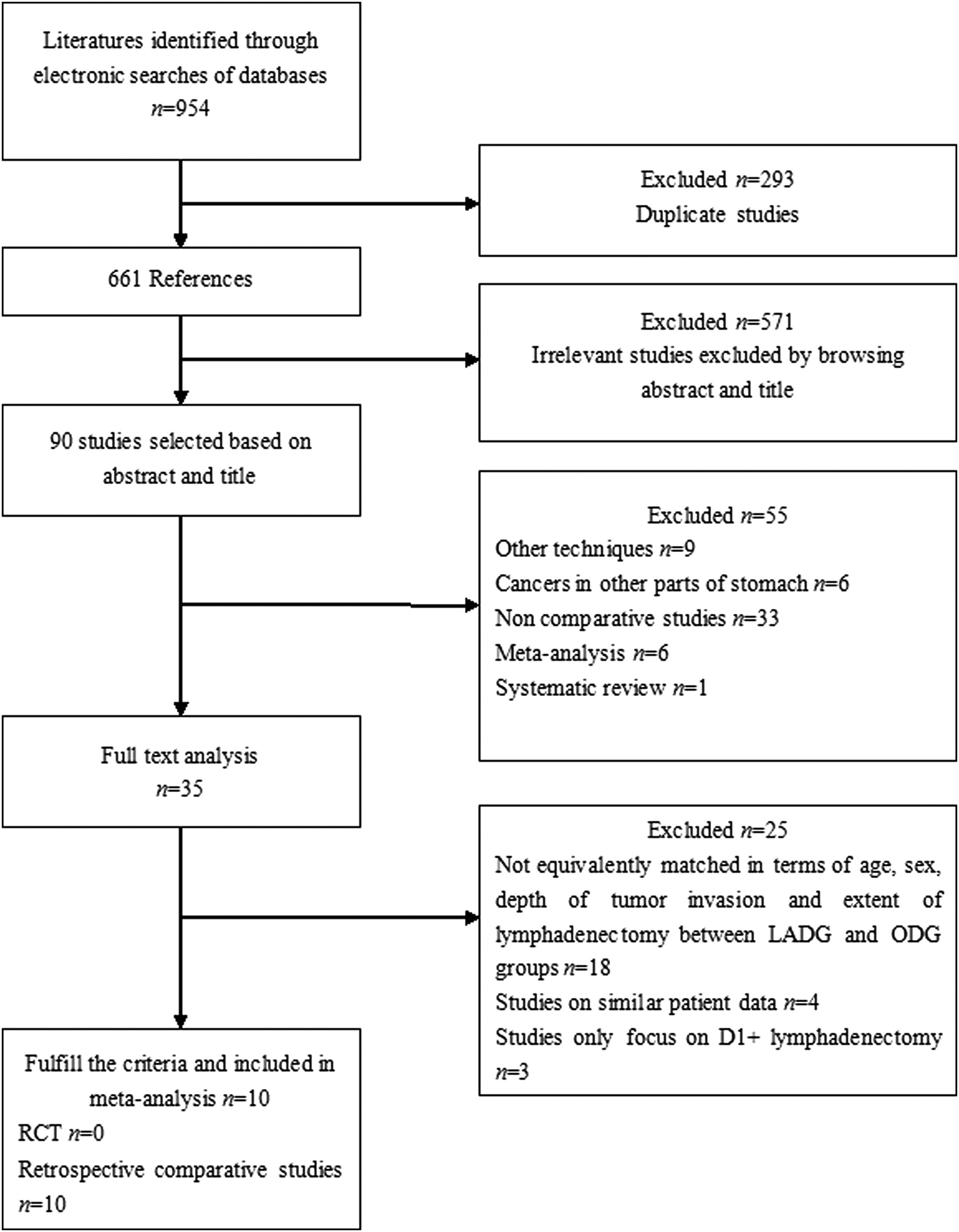
Flow diagram of study selection. LADG, laparoscopic-assisted distal gastrectomy; ODG, open distal gastrectomy; RCT, randomized controlled trial.
Matching based on: 1, age and sex; 2, depth of tumor invasion on preoperative diagnosis; 3, extent of lymphadenectomy; 4, tumor site; 5, tumor size; 6, postoperative pathologic stage; 7, histological type; 8, body mass index; 9, American Society of Anesthesiologists status; 10, median or mean follow-up; and 11, type of gastrointestinal reconstruction.
AJCC, American Joint Committee on Cancer; ASA, American Society of Anesthesiology; B-I, Billroth I; B-II, Billroth II; BMI, body mass index; LADG, laparoscopic-assisted distal gastrectomy; ODG, open distal gastrectomy; PNR, prospective nonrandomized study; R, retrospective study; R-Y, Roux-en-Y; UICC, Union for International Cancer Control.
AGC, advanced gastric cancer; EGC, early gastric cancer; LADG, laparoscopic-assisted distal gastrectomy.
The quality of each study was graded as low level (total score 0–5) or high level (total score 6–9).
Selection: (1) Assignment for treatment: One star was assigned if details of criteria for assignment of patients to treatments provided. (2) One star was assigned if the laparoscopic-assisted distal gastrectomy group was representative of patients for gastric cancer; no star was assigned if groups of patients were selected or selection of the group was not described. (3) One star was assigned if the open distal gastrectomy group was representative of patients for gastric cancer; no star was assigned if groups of patients were selected or selection of the group was not described.
Comparability: Comparability variables were as follows: 1, age; 2, sex; 3, depth of tumor invasion on preoperative diagnosis; 4, extent of lymphadenectomy; 5, median or mean follow-up; 6, American Society of Anesthesiologists status; 7, tumor size; 8, postoperative pathologic stage; and 9, histological type. (4) Two stars were assigned if the groups were all comparable for the variables 1–5; 1 star was assigned if one of these five characteristics was not reported, even if there were no other differences between the groups, and other characteristics had been controlled for; and no star was assigned if the two groups differed. (5) Two stars were assigned if the groups were all comparable for the variables 6–9; 1 star was assigned if one of these four characteristics was not reported, even if there were no other differences between the groups, and other characteristics had been controlled for; and no star was assigned if the two groups differed.
Outcome assessment: (6) One star was assigned if primary outcome parameters were clearly defined. (7) One star was assigned if more than 90% of patients were followed up.
Operative time
Accompanied with heterogeneity (HG=37.28, P<.0001), all of the 10 studies provided calculable data for analyzing the operative time.19–28 Our results revealed that the operative time for LADG D2 surgery was significantly longer than that for ODG in both of the two subgroups (P<.0001). Nevertheless, it was found that a reduction of 17.7 minutes in the operative time could be achieved if surgeons had accomplished 40 laparoscopic D2 radical gastrectomies (Table 4).
The value is a weighted mean difference (WMD).
P<.05 was defined as indicating a significant difference.
CI, confidence interval; HG, heterogeneity; LADG, laparoscopic-assisted distal gastrectomy; NA, not applicable; ODG, open distal gastrectomy; OR, odds ratio.
Intraoperative blood loss
Eight of the 10 studies were suitable for analysis of intraoperative bleeding.19–24,27,28 The blood loss for the subgroup of surgeons with experience of fewer than 40 LADGs was found to be 139.61 mL less in the LADG group than in the ODG group (WMD, −139.61; 95% CI, −223.68 to −55.53; P=.002), whereas the corresponding number was 182.31 mL in the subgroup of surgeons with experience of 40 or more cases (WMD, −182.31; 95% CI, −269.18 to −95.45; P<.00001) (Table 4). The above results suggested that the more experiences surgeons had, the better they could control the intraoperative bleeding during laparoscopic surgery.
Dissected lymph nodes
All of the 10 studies reported the amount of dissected lymph nodes without significant heterogeneity (HG=9.42, P=.40). The learning curve effect on this outcome parameter was obvious (Fig. 2 and Table 4). In the subgroup of surgeons with experience of 40 or more LADG cases, the number of resected lymph nodes of the LADG group was on average 2.02 larger than that for the ODG group, and this difference was significant (WMD, 2.02; 95% CI, 0.34–3.70; P=.02). However, the above advantage faded when surgeons with experience of <40 cases performed laparoscopic D2 gastrectomy (WMD, −0.92; 95% CI, −3.09 to 1.26; P=.41) (Fig. 2 and Table 4).
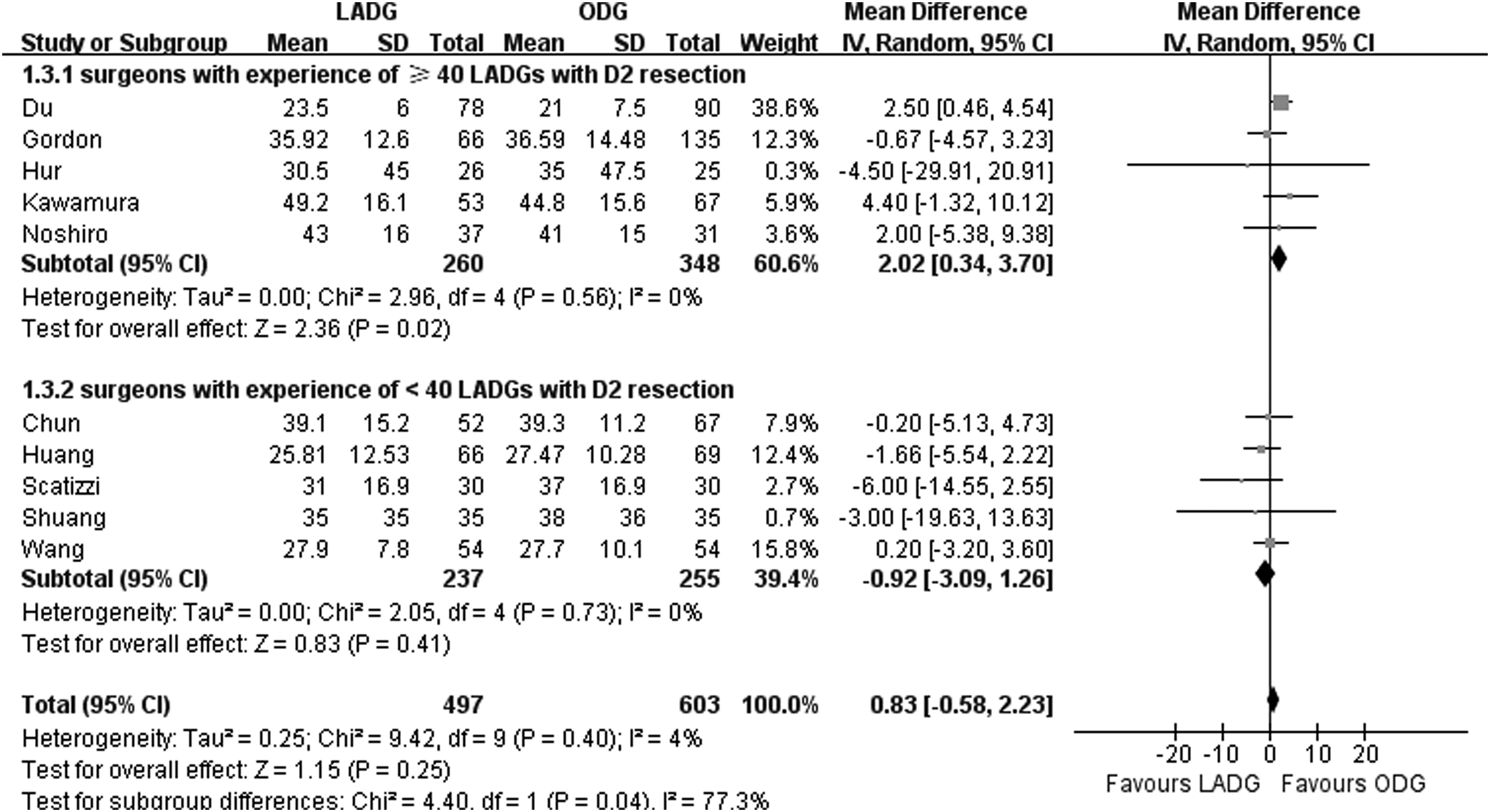
Meta-analysis of studies comparing dissected lymph nodes between laparoscopic-assisted distal gastrectomy (LADG) and open distal gastrectomy (ODG). The solid squares denote individual weighted mean difference (WMD), and the horizontal lines represent 95% confidence intervals (CIs). The diamonds show pooled WMD. SD, standard deviation; IV, inverse variance.
Postoperative recovery parameters
There were eight and five studies that provided data on the time to first flatus and time to liquid diet, respectively.19,20,22,23,25,26–28 Subgroup analysis of surgeons with experience of 40 or more LADGs showed that the time to flatus and that to liquid intake were, respectively, 0.96 and 0.98 days earlier in the LADG group than in the ODG group (P<.0001 and P<.00001, respectively). In contrast, according to subgroup analysis of surgeons with experience of <40 LADGs, no significant differences could be detected between the LADG and ODG groups when analyzing the above two recovery parameters (P=.09 and P=.94, respectively) (Fig. 3 and Table 4).
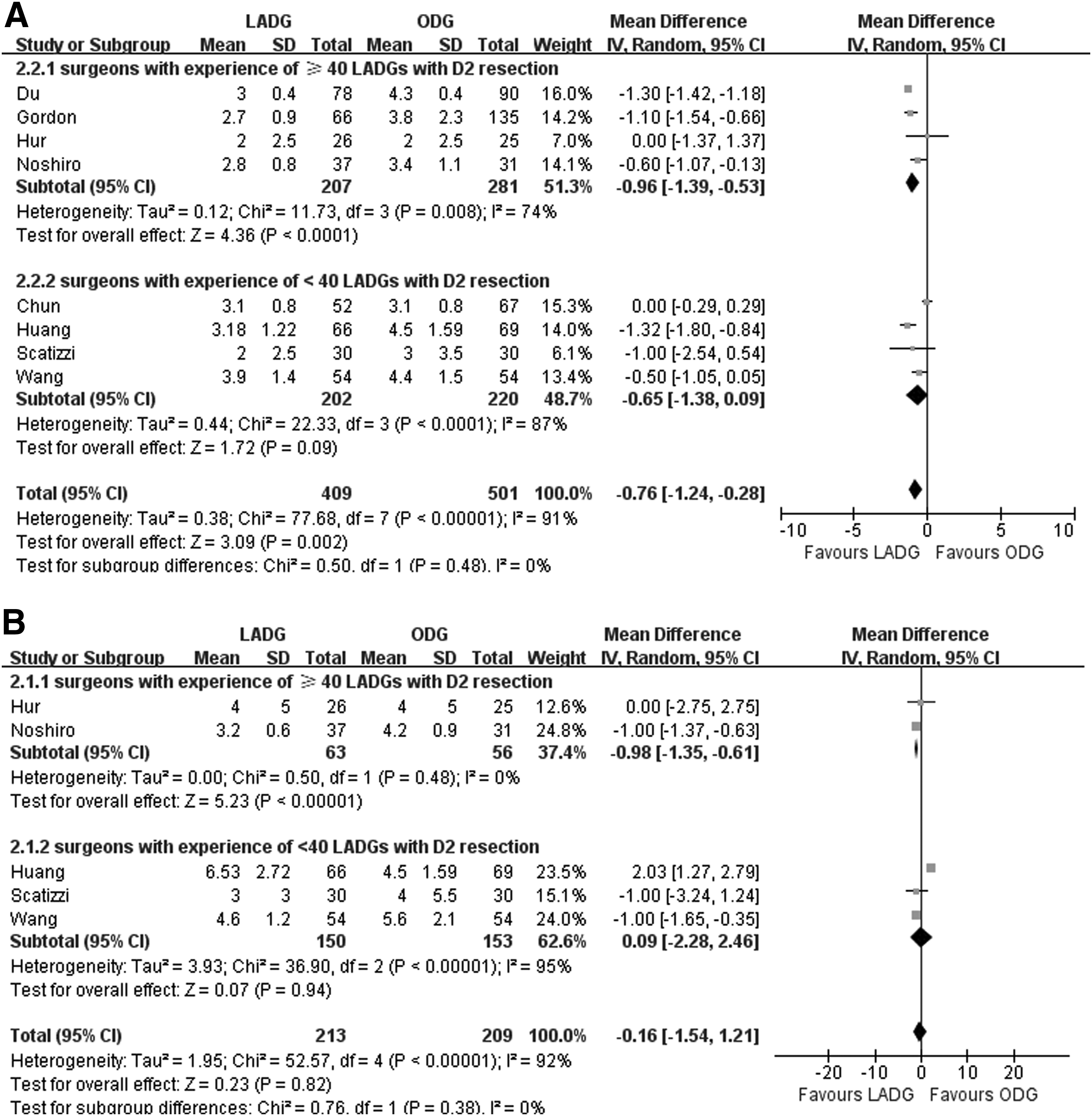
Meta-analysis of studies comparing postoperative recovery parameters including
Meta-analysis of nine included studies20–28 demonstrated that in both of the subgroups, the length of postoperative stay was significantly shorter in the LADG group than in the ODG group (P=.0003 and P=.0003, respectively) (Table 4).
Postoperative complications
As shown in Figure 4 and Table 4, all of the 10 studies reported data regarding the overall postoperative complications with no heterogeneity (HG=4.04, P=.91). The overall complications after LADG (11.13%, 55/494) were significantly fewer than those after ODG (17.25%, 104/603) (OR, 0.62; 95% CI, 0.43–0.89; P=.01). However, when further analysis was performed, only the subgroup of surgeons with experience of 40 or more LADGs revealed an obvious lower overall complications rate in LADG than in ODG (9.34% versus 17.24%; OR, 0.55; 95% CI, 0.33–0.92; P=.02), but in the subgroup of surgeons with experience of <40 LADGs this rate was no different between the laparoscopic and open approaches (13.08% versus 17.25%; OR, 0.69; 95% CI, 0.41–1.17; P=.17).
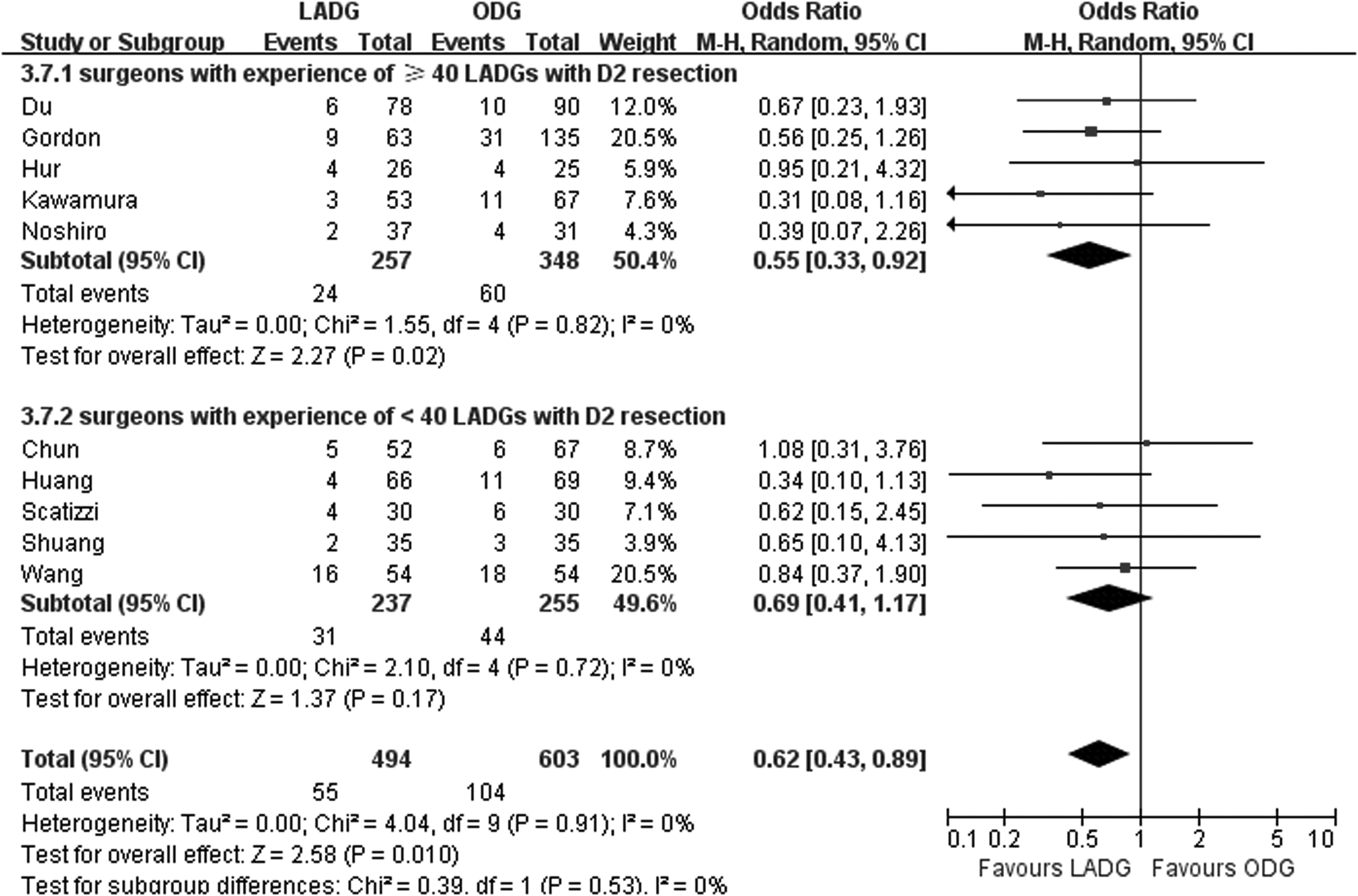
Meta-analysis of studies comparing overall complications between laparoscopic-assisted distal gastrectomy (LADG) and open distal gastrectomy (ODG).The solid squares denote individual odds ratio (OR) values, and the horizontal lines represent 95% confidence intervals (CIs). The diamonds show pooled OR values. M-H, Mantel–Haenszel.
Our meta-analysis revealed a significant lower incidence rate of pulmonary infection in the LADG group than in the ODG group (0.94% versus 5.74%; OR, 0.30; 95% CI, 0.09–0.96; P=.04) (Table 4). No differences could be detected between LADG and ODG with regard to incidences of postoperative bleeding (P=.85), duodenal stump fistula (P=.55), anastomotic stenosis (P=.83), ileus (P=.24), and wound infection (P=.21). Subgroup analysis did not demonstrate any differences between LADG and ODG with regard to the occurrences of the above complications.
Short-term mortality
Meta-analysis of short-term mortality was impossible to perform because there was only one included study, that by Chun et al., 26 that reported one case of short-term postoperative death in the LADG group.
Publication bias
Egger's test and graphical test with Begg's funnel plot were used to detect the publication bias. As outlined in Table 5 and Figure 5, no publication bias was detected in any of the clinical parameters (P>.05).
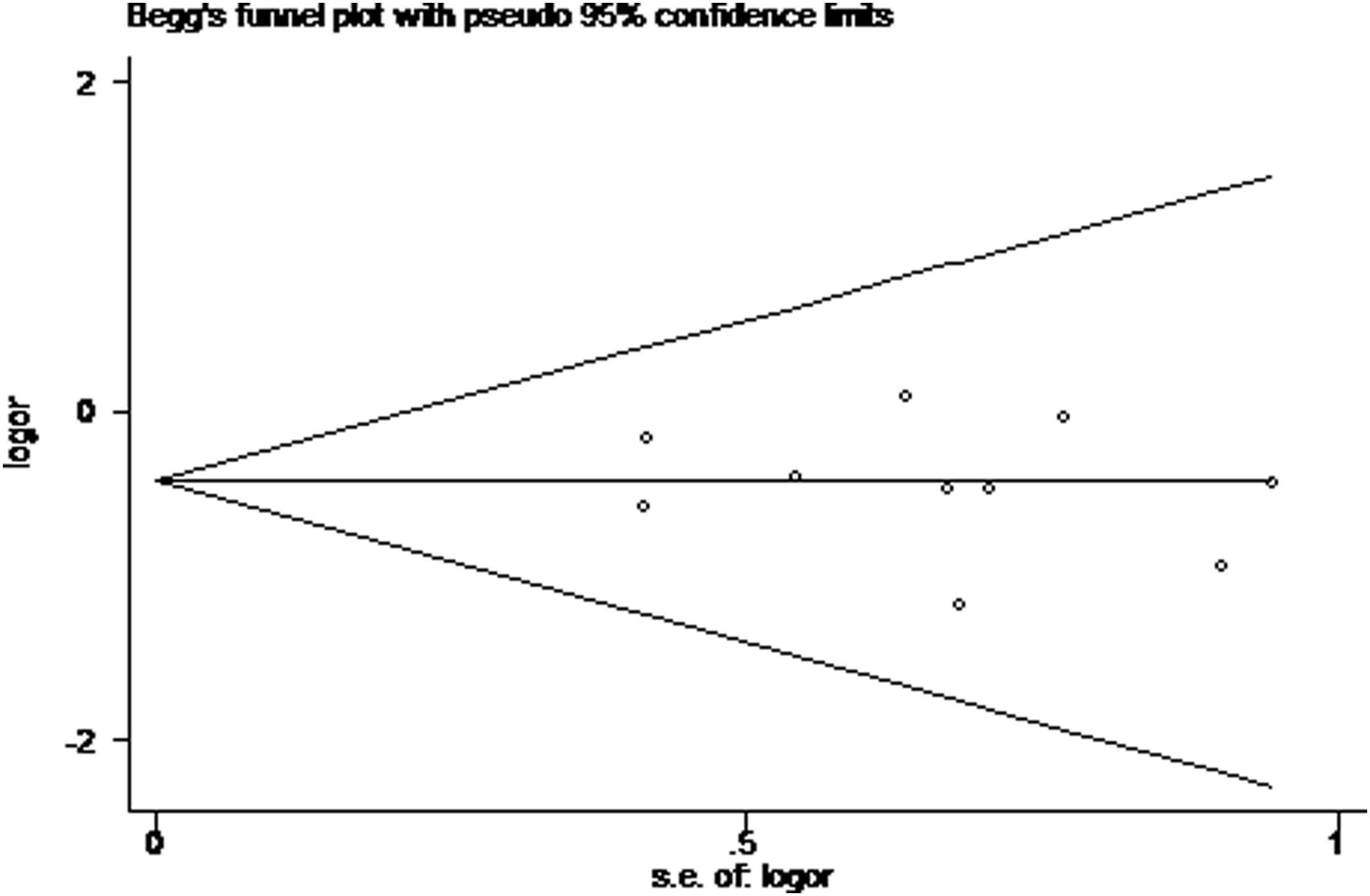
Begg's funnel plot (with pseudo 95% confidence intervals) to detect publication bias for pooled studies comparing the overall complications between laparoscopic-assisted distal gastrectomy and open distal gastrectomy. Odds ratio (or) values are presented on a logarithmic scale. s.e., standard error.
Discussion
In the past two decades, laparoscopic-assisted gastrectomy has been widely accepted for treating early gastric cancer because of its advantages of minimal invasiveness and oncological radicality comparable to that of the conventional open approach. Currently, several centers are moving toward the feasibility of LADG for advanced gastric cancer. However, laparoscopic second-tier lymph node dissection under a two-dimensional video image makes training for laparoscopic skills more difficult than D1 surgery in terms of making a clear operative field, selecting a reasonable surgical approach, and achieving en bloc resection. The length of time to overcome the learning curve of LADG with D2 surgery varies among surgeons, and it is often associated with the surgeon's ability, the training program, previous experience of laparoscopy, hospital volume, and patients' characteristics. 29 The definition of the completion of learning is still arbitrary. To determine whether the learning curve has been overcome, some authors used the minimization of operative complications, whereas others used the reaching of a steady mean operative time and the number of retrieved lymph nodes as measures.30,31
In this meta-analysis, we divided the included studies into two subgroups according to the status of the surgeons' level of experience, and we chose the “threshold of 40 cases” because of the following three reasons. First, according to the reports from some large clinical centers, in the first 20–30 cases, surgeons who have insufficient education of LADG with D2 lymphadenectomy achieve relatively slow progress in operation time and the number of retrieved lymph nodes; however, when surgeons achieve up to 25–40 cases, the decreasing slope of the learning curve appears apparent.32–34 The operation time and the number of retrieved lymph nodes both reach plateaus after the 50th cases. Second, the “threshold of 40 cases” was calculated based on the statistical analysis where multiple data points were examined, and “40 cases” was the one with the greatest difference. Finally, before we chose the “threshold point,” we used data from our own center to perform an ROC curve analysis to state what the optimal experience would be. Figure 6 indicates that three surgeons with few experiences of LADG could retrieve amounts of lymph nodes comparable to those in open surgery after their 35th, 38th, and 43th laparoscopic cases, respectively. Figure 7 revealed that when these three surgeons had accomplished their 36th, 38th, and 41th cases, respectively, the operation time reached a plateau. So, we chose the “threshold of 40 cases” as the optimal experience point.
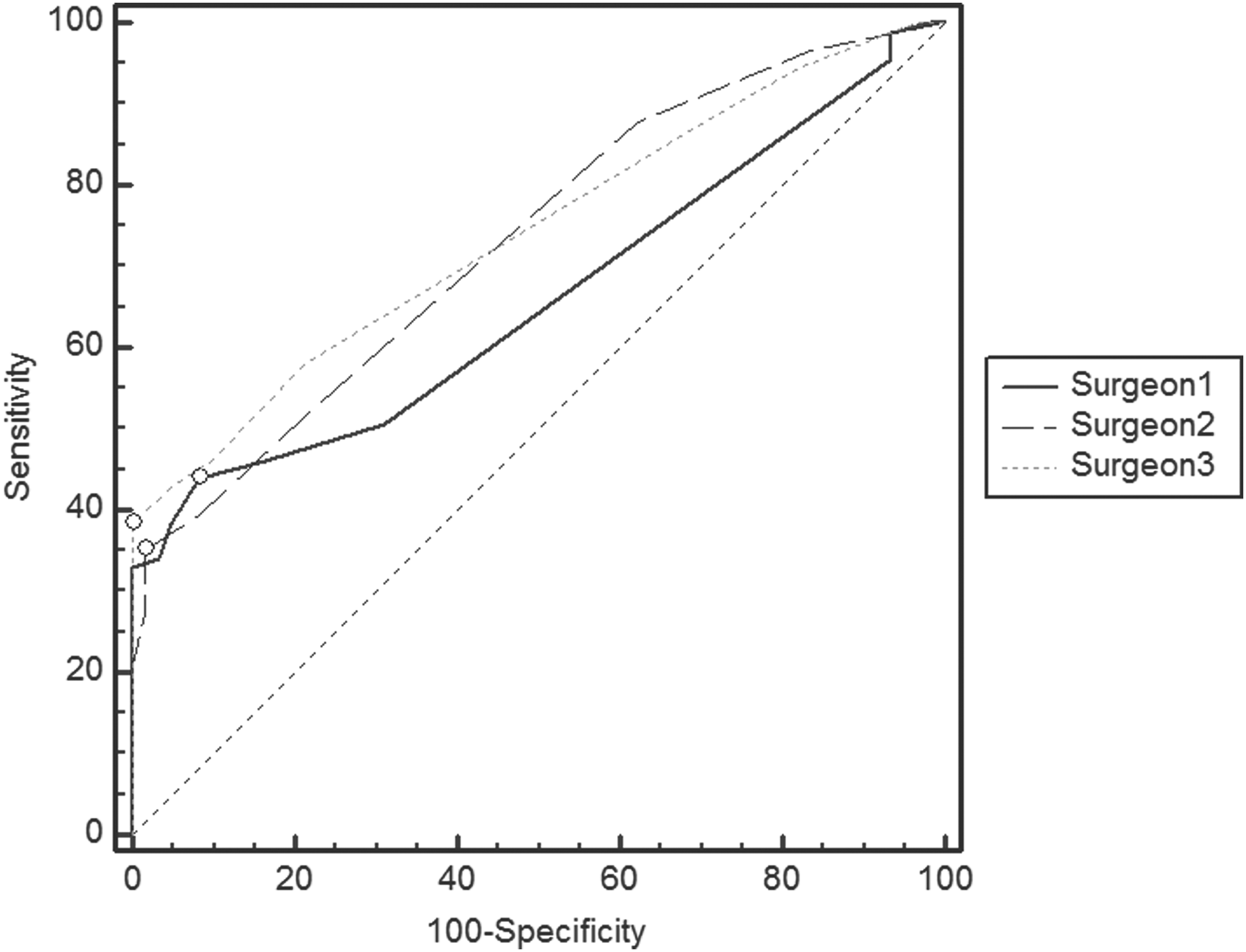
The receiver operator characteristic curve indicates that three surgeons with little experiences of laparoscopic-assisted distal gastrectomy could retrieve amounts of lymph nodes comparable to those during open surgery after their 35th, 38th, and 43th laparoscopic cases, respectively. Pairwise comparison of receiver operator characteristic curves showed there were no differences among the areas under the curves (P>.05).
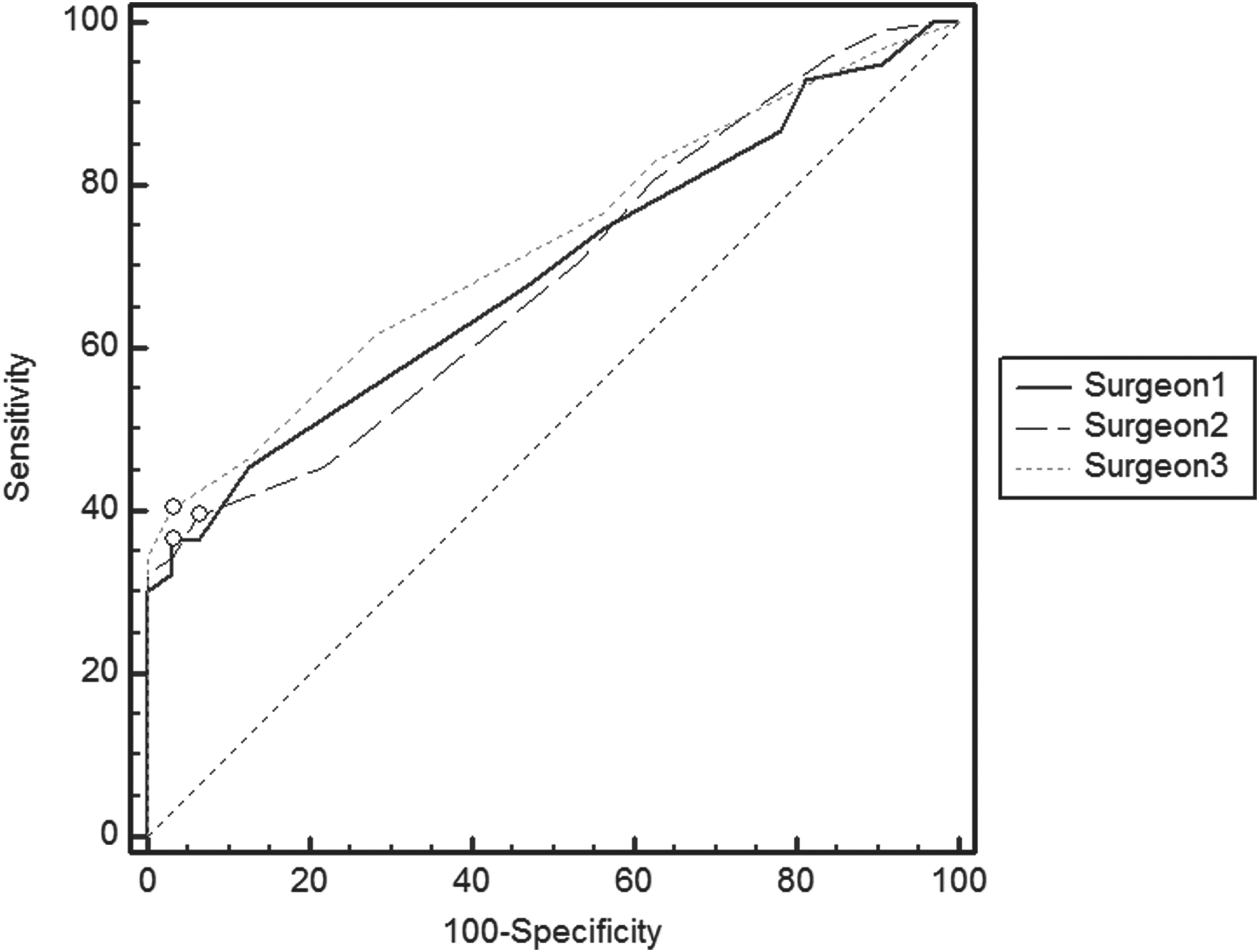
The receiver operator characteristic curve revealed that when the three surgeons represented in Figure 6 had accomplished 36, 38, and 41 cases, respectively, the operation time reached a plateau. Pairwise comparison of receiver operator characteristic curves showed there were no differences among the areas under the curve (P>.05).
The operation time is considered as a representative indicator for evaluating the extent of proficiency of a new technique. The present meta-analysis revealed that the operative time for LADG with D2 resection was longer than that for ODG, but surgeons with experience of 40 or more cases could on average reduce the LADG operation time by 20 minutes compared with that of surgeons with experience of fewer than 40 cases. Our data were similar to the findings by Song et al., 34 who found that the operation time for LADG with D2 dissection would decrease abruptly during a surgeon's 30th–40th surgery; they reported that the beginner surgeon could reach his or her operation time plateau of less than 300 minutes after he or she had completed 30 consecutive cases of LADG. Kim et al. 33 suggested that there was another time plateau in the later learning course of LADG. The mean operation time reached its second plateau of less than 200 minutes after accumulation of 70 consecutive laparoscopic D2 cases experiences. However, other centers showed that the “first optimum proficiency point” could only be achieved with experience of 50–60 LADG D2 cases.10,32 These differences may caused by the patient volume of these centers or the number of conventional open D2 gastrectomies performed by their teams.
Lymphadenectomy is the core part of radical gastrectomy, and the number of retrieved lymph nodes is thought to be related with patients' prognosis. Most studies published before 2005 showed that the number of harvested lymph nodes during laparoscopic gastrectomy was significantly lower than during ODG.35–37 Then, as the operative technique has developed, the number of lymph nodes dissected by LADG has gradually increased. Our meta-analysis demonstrated that surgeons with experience of fewer than 40 cases reached the same amount of dissected lymph nodes compared with the ODG group, but, more notably, our data showed that surgeons with experience of 40 or more cases could retrieve on average more 2.02 lymph nodes than those in the ODG group did. This exciting result suggested that the laparoscopic procedure did not limit the feasibility of an oncological radical resection and extended D2 lymphadenectomy. The difficulty of the second-tier lymph node dissection lies in full-length vascularization of major blood vessels, which requires a good deep exposure of the surgical field. In general, D2 lymph node dissection is achieved by the removal of station 11p (along with the splenic artery), 12a (along with the proper hepatic artery) lymph nodes, 14v (surface of the superior mesenteric vein at the level of the lower border of pancreas), and D1+β lymph node stations. Du et al. 22 demonstrated that experience with a reasonable surgical approach might be helpful in reducing the operation time as well as improving the number of retrieved lymph nodes. Song et al. 34 reported that when compared with those with ODG experience, surgeons with adequate experience of LADG could achieve comparable numbers of 12a and 14v lymph nodes, which are considered to be the most difficult anatomical positions for laparoscopic surgery. Thus, greater experience in LADG improves the eradication of a sufficient lymphadenectomy around the paragastric arteries, parapancreatic vessels, and celiac trunk.
Not only the operation time and the competence of radical resection should be of concern, but also patients' safety should be considered. The relationship between the learning curve of LADG and the occurrence of postoperative complications still remains unclear. Some studies indicated that a high frequency of postoperative complications occurred mainly in the very early period of the learning curve.38,39 However, Yoo et al. 40 reported that the completion of the first 50 LADG cases would result in a significant improvement in operative time but did not correspond with a significant reduction in complications. In our study, subgroup analysis of surgeons with experience of fewer than 40 cases revealed no differences between LADG and ODG D2 gastrectomy in terms of overall complication rate, whereas this rate was significantly lower in patients undergoing LADG than in those undergoing ODG in the subgroup of surgeons with experience of 40 or more cases. This result reflected that although the time point at which proficiency is reached might vary greatly and could be affected by many factors, LADG could achieve a sustainably lower complication rate than ODG through adequate training of the surgeon.
Owing to the enlarged laparoscopic surgical field, accurate operation, and the use of special instruments, including an ultrasonic scalpel and ligatures, the beginner surgeon may not require a traditional learning period. 41 However, in the present study, analysis of the learning curve effect on patients' postoperative recovery suggested that the surgeon's experience still played an important role in improving the advantages of laparoscopic surgery. Our data showed that surgeons with experience of fewer than 40 cases could already achieve less blood loss and better postoperative recovery in the LADG group than in the ODG group; however, after the surgeon had had experience with the 40th LADG case, even less intraoperative bleeding and a shorter time to flatus, time to liquid diet, and length of hospital stay were observed. Compared with postoperative fasting or feeding, time to flatus is thought to be an ideal objective indicator for gastrointestinal motility recovery, which is mainly affected by the extent of surgical trauma. Our results indicated that the advantages of minimally invasive surgery were evident even in the early stage of learning curve, and these advantages could be expanded by an experienced surgeon who could perform LADG with a more subtle operative technique and reduced the adverse effects of the surgical trauma.
There were two limitations that must be taken into account. First, all of the included studies are retrospective ones because up until now there has been no published RCT in particular comparing LADG and ODG with D2 resection. Therefore, adequate blind methodology and allocation concealment were absent. This methodological handicap may exaggerate the treatment effectiveness of LADG ascribed to the detection bias generated from outcome measurement and performance bias introduced by unequal application of co-intervention. In view of this, we eliminated the studies in which matching was not equivalent in terms of age, sex, tumor staging, extent of lymphadenectomy, and co-intervention between LADG and ODG. Second, the heterogeneity and potential reporting bias might exaggerate the overall effect size of outcome measures, although we already used the random model. In our meta-analysis, when comparing each kind of the postoperative complication, the current sample size might not be large enough to distinguish the differences between LADG and ODG. Nevertheless, because of the absence of RCTs, our results from high-quality comparative studies would be powerful, and it was also useful in guiding researchers toward properly informed randomization in future RCTs.
The fast pace of development and innovation of laparoscopic surgery has led to its use for standard D2 lymphadenectomy. Although the advances in surgical instruments help the beginners in improving short-term outcomes during their early period of training, our meta-analysis indicated that the learning curve still has significant effects on most of the important surgical and short-term recovery outcome parameters. For beginners, overcoming the learning curve means a shorter operative time, more dissected lymph nodes, faster gastrointestinal motility recovery, and fewer incidences of complications. Therefore, our study suggested that accomplishment of 40 cases of LADG with D2 lymphadenectomy is required to achieve optimum proficiency.
Footnotes
Acknowledgments
The authors thank Dr. Pengyuan Zhuang for critical review and comments and assistance in the literature search. This work was supported by the Medical Scientific Research Fund of XinHua Hospital, Shanghai Jiaotong University, School of Medicine (grant 11XJ22004). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure Statement
No competing financial interests exist.