
Abstract
Abstract
Purpose:
The aim of this study was to evaluate short- and intermediate-term results of laparoscopic liver resection in selected patients with hepatocellular carcinoma (HCC).
Patients and Methods:
Eighty-five patients with HCC were subjected to liver resection between February 2007 and January 2013. From these, 30 (35.2%) were subjected to laparoscopic liver resection and were retrospectively analyzed. Special emphasis was given to the indication criteria and to surgical results.
Results:
There were 21 males and 9 females with a mean age of 57.4 years. Patients were subjected to 10 nonanatomic and 20 anatomic resections. Two patients were subjected to hand-assisted procedures (right posterior sectionectomies); all other patients were subjected to totally laparoscopic procedures. Conversion to open surgery was necessary in 4 patients (13.3%). Postoperative complications were observed in 12 patients (40%), and the mortality rate was 3.3%. Mean overall survival was 29.8 months, with 3-year overall and disease-free survival rates of 76% and 58%, respectively.
Conclusions:
Laparoscopic treatment of selected patients with HCC is safe and feasible and can lead to good short- and intermediate-term results.
Introduction
H
Resection, a therapeutic alternative that can be performed readily and with lower costs compared with liver transplantation, has become a safe procedure in the last years with mortality rates in specialized centers lower than 5%.8,9 In selected cases, good long-term results can be achieved (50%–70% 5-year overall survival). However, resection is followed by high rates of morbidity and mortality in patients with chronic liver disease, being possible only in patients with preserved liver function. 10
Despite the controversy between resection and transplantation, groups specializing in both liver surgery and liver transplantation, in the context of a long waiting list for transplant (more than 6–9 months), have advocated resection for the treatment of solitary HCC in patients with preserved liver function. It has also been shown that in patients within the Milan criteria, the long-term outcome of those listed for liver transplantation (intention-to-treat analysis) was similar when compared with patients who underwent resection. 11 There are many other arguments other than the avoidance of a long waiting list favoring liver resection for HCC: immediately applicability, lower mortality rate, the availability of a surgical specimen for histological and molecular evaluation, and good long-term results. 12
Most of the groups that deal with patients with liver diseases use a screening program to detect early HCC, thereby increasing the number of patients diagnosed with small HCC nodules in the last few years.13,14 It has already been shown that laparoscopic liver resection (LLR) for HCC, especially when indicated for solitary, small, and peripheral tumors in patients with preserved liver function, is safe and can lead to good short- and long-term results. 15 The enthusiasm for minimally invasive treatment of HCC led to the publication of many case series showing very good results.16–19 Recent meta-analyses showed that laparoscopic resection led to shorter hospital stay, decreased blood loss, and lower rates of postoperative morbidity (less ascites) compared with open liver resection.8,20,21
The aim of this study was to evaluate short- and intermediate-term results of LLR for selected patients with HCC. The authors also present their guidelines for the treatment of HCC.
Patients and Methods
From a prospective hepatobiliary surgical database, 85 patients with HCC were subjected to liver resection in our unit between February 2007 and January 2013. From these patients, 30 (35.2%) were subjected to LLR and were retrospectively analyzed. All patients were subjected to clinical evaluation and liver function laboratory tests. Preoperative workup included helicoidal computed tomography (CT) scan or magnetic resonance, thoracic CT, and bone scintigraphy. Diagnosis was based on image characteristics; none of the patients was subjected to liver biopsy. In patients in whom CT or magnetic resonance imaging depicted signs of portal hypertension, upper digestive endoscopy was performed. Radiological studies were reviewed in a multidisciplinary meeting held weekly.
Treatment guidelines for HCC in our unit are shown in Figure 1.
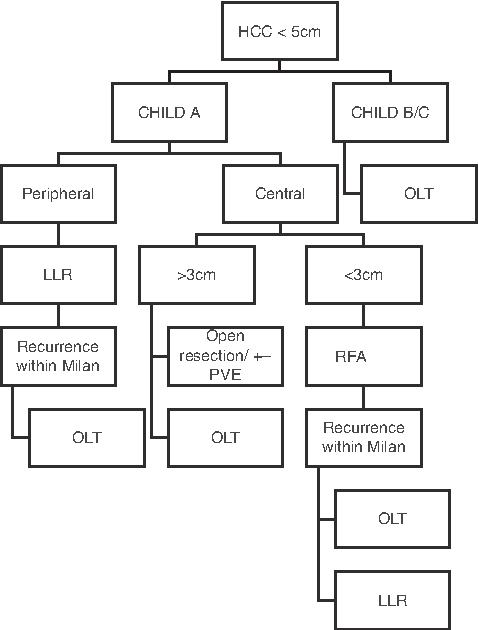
Guidelines for the treatment of single hepatocellular carcinoma (HCC) within the Milan criteria. LLR, laparoscopic liver resection; OLT, orthotopic liver transplant; RFA, radiofrequency ablation; PVE, portal vein embolization.
The selection criteria for the laparoscopic approach were as follows:
• Solitary nodule, smaller than 5 cm in diameter • Preserved liver function (Child–Pugh Class A) • Peripheral location on the liver • Resection of up to two segments of the liver • Platelet count of >100,000/mL • American Society of Anesthesiologists score lower than 3 • Patients with portal hypertension and esophageal varices Grade 1 or 2 (with platelet count of >100,000/mL) in Child Class A patients were not excluded.
In brief, all patients were positioned in a supine French position with the surgeon positioned between the legs. For right lateral resections, the patient was placed in a left lateral (45°) position. Pneumoperitoneum was set at 12 mm Hg, and intraoperative staging was performed. Parenchyma transection was performed with the use of a Harmonic® scalpel (Ultracision®; Ethicon Endosurgery, Cincinnati, OH) or LigaSure™ (Valleylab, Boulder, CO). For the resection of a segment or section, the transection of the portal pedicle and hepatic veins was done with the use of vascular staplers. Specimen removal was done inside a plastic bag through the umbilical or a suprapubic incision. During parenchyma transection all patients were maintained with low central venous pressure levels (between 3 and 5 cm H2O). No routine drainage was used.
In the last 2 patients with tumors located in the right posterior section, a hand-assisted procedure was performed through a small upper midline incision. 22
Liver resections were defined according to the Brisbane 2000 classification. 23 Intraoperative and immediate postoperative data collected included perioperative transfusions, conversions to open procedure (hybrid procedure), surgical margins, postoperative complications, length of hospital stay, and mortality. Postoperative complications were classified according to the Clavien–Dindo classification. 24 Postoperative follow-up was performed every 4 months, including clinical, laboratory, and radiological evaluation. Data collected included disease recurrence and mortality.
Continuous variables were expressed as median (range) and were compared by means of the Mann–Whitney test. Categorical variables were compared by the chi-squared test or Fisher's exact test. Survival and recurrence-free survival were measured from the date of operation to the time of death or at the time when a recurrent tumor was first diagnosed, respectively. Survival analysis was estimated by the Kaplan–Meier survival method, and the differences in survival between the groups were compared by the log-rank test. Differences were considered as statistically significant when the P value was <.05.
Results
There were 21 males and 9 females with a mean age of 57.4 years (ranging from 28 to 77 years). The etiology of liver cirrhosis is depicted in Table 1. All patients presented a solitary nodule with a mean size of 3.7 cm (range, 2–5 cm). In 21 patients nodules were peripheral or located in a lateral position within liver parenchyma.
HCV, hepatitis B virus; HCV, hepatitis C virus; NASH, nonalcoholic steatohepatitis.
Patients were subjected to 10 nonanatomic resections and 20 anatomic resections (14 left lateral sectionectomies, 4 segmentectomies 6/7, 1 right hemi-hepatectomy, and 1 left hemi-hepatectomy). One patient without any comorbidity with a 5-cm nodule located in the middle of the right hemi-liver was subjected to a right hepatectomy. All surgical margins were free of tumor for at least 1 cm.
Two patients were subjected to hand-assisted procedures (right posterior sectionectomies); all other patients were subjected to totally laparoscopic procedures.
Conversion to open surgery was performed in 4 patients (13.3%) because of bleeding in 3 patients and staple failure in the other. Intraoperative transfusion was performed in 6 (20%) patients. The median and mean length of hospital stay was 6 days and 7.8 days, respectively (range, 2–24 days).
As seen in Table 1, postoperative complications were observed in 12 patients (40%); these included ascites in 5 patients, nondialytic acute renal failure in 2, encephalopathy in 1, biliary fistula in 1, postoperative ileus in 1, colonic perforation in 1, and sepsis due to pneumonia in 1 (right hepatectomy). An unidentified colonic perforation was diagnosed after 7 days, leading to re-operation, multi-organ dysfunction, and death after 24 days, leading to a mortality rate of 3.3%.
During long-term follow-up 1 patient developed an umbilical hernia that was surgically treated with good outcome. Ten of 29 patients (34.4%) had recurrent disease as follows: liver-only in 6, lung in 2, adrenal gland in 2, and epigastric port site in 1. Of the 6 patients with liver-only recurrence, 4 were subjected to intra-arterial embolization or radiofrequency ablation as a bridge to liver transplantation. Two of these patients were subjected to orthotopic liver transplant with good outcome.
The other 2 patients with liver-only recurrence were subjected to palliative intra-arterial embolization, whereas 2 patients with lung metastasis underwent systemic treatment with sorafenib. One patient with adrenal metastasis was subjected to adrenal laparoscopic resection, and the other one with abdominal wall recurrence was subjected to local resection.
Mean overall survival was 29.8 months with a 3-year survival of 76% and 3-year disease-free survival of 58% (Fig. 2).

Overall survival and disease-free survival curves for patients with hepatocellular carcinoma subjected to laparoscopic liver resection.
Discussion
LLR is gaining worldwide acceptance recently because of the excellent results shown by expert surgeons in specialized centers. The feasibility and safety of LLR even for major resections have also been confirmed. 25 However, when dealing with patients with HCC, issues such as liver function, size of the remnant liver, bleeding control during a diseased parenchyma section, surgical margins, and postoperative morbidity have to be considered.
Recent series of laparoscopic resection of HCC published by very skilled surgeons have shown excellent results not only when morbidity and mortality were evaluated, but also long-term results.16,20,21,26–29 These enthusiastic results have led to a discussion of the real place of LLR in the treatment algorithm for HCC. In our group, beginning in 2006 we proposed a guideline for the curative treatment of HCC based on a case-by-case multidisciplinary discussion.
As liver function is considered the most important determinant of postoperative morbidity and mortality following liver resection, resection should be reserved for Child–Pugh Class A patients, with those being Child–Pugh Class B or C referred for transplantation. Fan et al. 30 have shown that for Child Class A patients within the Milan criteria, resection can lead to the same results independently of the presence of normal liver parenchyma, chronic hepatitis, or cirrhosis. According to the European and American guidelines for the treatment of HCC, the presence of portal hypertension is considered as a contraindication for liver resection because of the higher risk of liver dysfunction and mortality; however, this statement is not widely accepted. 31 Capussoti et al. 31 showed that for Child–Pugh Class A patients, the presence of portal hypertension did not affect survival following liver resection. Indeed, Cucchetti et al. 32 also stated that the presence of portal hypertension should not exclude from surgery patients who could potentially benefit from curative resection. In our series, all patients had a preserved liver function and small nodules and, with the exception of 1 case, were subjected to limited resections; thus, the presence of small varices in patients with platelet counts >100,000/mL did not lead to an increase in morbidity or mortality.
Owing to the improvement of screening programs in patients with chronic liver disease, small HCC (early-stage) cases have been more frequently diagnosed. Patients with preserved liver function and small tumors are the best candidates for laparoscopic treatment. There are three different approaches for LLR: totally laparoscopic, hand-assisted, and hybrid resections. Our group prefers the totally laparoscopic approach except in patients with tumors located in the posterior segments of the right hemi-liver (segments 6 and 7), where a hand-assisted or a hybrid procedure seems to be easier and faster.22,33 Koffron et al. 34 presented their experience with a laparoscopic-assisted method (hybrid method) where liver mobilization and hilar dissection are done laparoscopically with hand assistance and the small hand port is used for liver transection; this maneuver turns a tedious and slow right liver mobilization into a simple, fast, and safe procedure. Nitta et al. 35 have also shown the usefulness of the laparoscopy-assisted technique for major liver resections.
A point of discussion is the type of resection for HCC. Anatomical surgery, where one or more entire segments with their portal pedicle are resected, has been advocated as the ideal treatment for HCC. It is well known that for HCC the main tumor pathway spread is through the portal vein; thus the en bloc resection of the tumor and its portal vein territory may lead to better oncological results. 36 However, in patients with chronic liver disease and cirrhosis, parenchyma-sparing procedures are mandatory to avoid postoperative liver failure. Thus, the choice between a nonanatomic wedge resection and an anatomic resection should be individualized. In our series, we tried to perform anatomical resections except in cases with small peripheral subcapsular nodules or in patients with signs of portal hypertension.
The optimal resection margin for HCC resection is still controversial. In a randomized trial comparing a wide 2-cm margin with a margin aiming at 1 cm, Shi et al. 37 found lower postoperative recurrence rates and better survival in the wide margin group. However, it is accepted that a 1-cm disease-free margin is adequate for the majority of patients with HCC. 37 Shi et al. 37 have recently shown that marginal resection (free margins smaller than 1 mm) did not negatively affect postoperative recurrence-free survival. In our series, all patients had free margins larger than 1 cm, and no recurrence at the operation site was observed. In a recent meta-analysis, Zhou et al. 38 showed no differences in surgical margins when comparing the open liver resection group with the LLR group.
The potential risk of intraoperative bleeding during laparoscopic liver resection in patients with HCC remains a matter of concern. However, most series have shown less bleeding and necessity of transfusion compared with open surgery. Aldrigheti et al. 19 emphasized the hemostatic effect of the pneumoperitoneum and the advantage of image magnification to reduce blood loss during LLR. The improvement of energy devices and staplers used for liver transection is also an important factor for bleeding control. 19 In our series, fewer than 20% of the patients required blood transfusion, and the Pringle maneuver was used in 4 patients in whom conversion to open surgery was necessary. In a multi-institutional European series with 163 LLRs, 9.2% of the procedures were converted to open or hand-assisted surgery, mostly because of bleeding or technical difficulties. 18
LLR presents the advantages of a minimally invasive procedure such as less postoperative pain, fast recovery, and early return to work. Although there are no controlled trials comparing LLR and open resection for the treatment of HCC, most case-control studies and small series of patients have shown advantages over the open approach in well-selected cases. In a recent meta-analysis, operative blood loss, blood transfusion, and length of hospital stay were significantly lower in the LLR group. 20 Moreover, lower incidences of postoperative ascites were observed compared with the open procedure in almost all series of LLR, probably as a consequence of the preservation of the abdominal wall and umbilical round ligament collateral venous circulation.12,16,18,19,27,29,39–41 Another potential advantage is the avoidance of adhesions in patients subjected to LLR with recurrent disease and candidates for a rescue future liver transplant. 12 Two of our patients presented with postoperative ascites; however, both were easily controlled with medical treatment (sodium restriction and diuretics). No other signs of postoperative liver failure such as jaundice or encephalopathy were observed.
The major drawback of liver resection for HCC is the high recurrence rate of about 40% in the first year. Despite a higher recurrence rate after resection, most authors have shown that those patients can be subjected to salvage liver transplantation. Belghiti et al. 42 showed that patients subjected to salvage transplantation present the same long-term results as those subjected to transplantation as the primary treatment. Indeed, Cherqui et al. 43 have shown that among their patients with recurrent HCC following LLR, 77% were transplantable (within the Milan criteria). The same group indicated that LLR when compared with open liver resection for HCC had decreased morbidity after salvage liver transplantation. 12 In our experience, 8 patients had recurrence only in the liver; 6 of them (75%) were transplantable and were subjected to bridge procedures for liver transplantation. Two patients were subjected to liver transplantation without any significant difficulty.
In our series, 3-year overall survival and disease-free survival were 76% and 58%, respectively. Belli et al., 44 in a case-control study, presented similar overall and disease-free survival rates comparing the conventional approach with LLR, showing that from an oncological point of view that the minimally invasive approach was comparable to open surgery. In a recent article with 65 patients subjected to LLR for HCC, the same authors showed long-term results comparable to the open procedure. 16 Other well-balanced case-control series showed similar overall and disease-free survival rates.9,28,45 Zhou et al., 21 in a recent meta-analysis, have also shown similar overall and disease-free survival rates comparing open with LLR.
Thus laparoscopic treatment of selected patients with HCC is safe and feasible and can lead to good long-term results. LLR can be considered as a curative therapy for a significant number of patients or, for those with recurrence, as a bridge procedure for curative liver transplantation. But, above all, LLR should be part of the therapeutic armamentarium for the curative treatment of HCC.
Footnotes
Acknowledgments
We thank Mr. Marcio Augusto Diniz from the Laboratory of Epidemiology and Statistics, Department of Gastroenterology, School of Medicine, University of São Paulo Medical School.
Disclosure Statement
No competing financial interests exist.
Author Contributions
P.H. designed and wrote the manuscript. M.V.P. and F.F.C. revised the manuscript and did the statistical analysis. G.M.F. and F.deL.M.L. performed research on the patient database and revised the manuscript. J.A.P.K., R.M.L., and I.C. revised the manuscript.