
Abstract
Abstract
Background:
Solid pancreatic pseudopapillary tumors make up 1%–3% of all pancreatic tumors, occur predominantly in females, and usually present in the third and fourth decades of life. Less frequently, these tumors may present in children. Complete surgical excision is the treatment of choice with excellent outcomes. Usage of a laparoscopic approach has become more common for adult patients. However, the laparoscopic approach is not routinely used in the pediatric population.
Materials and Methods:
A literature review was performed noting 13 documented cases of solid pancreatic pseudopapillary tumors resected laparoscopically in children. We report our case series of three children with a solid pancreatic pseudopapillary tumor treated through a minimally invasive approach.
Results:
In the literature, most patients had the tumor in the body or distal pancreas. The most common complication was pancreatic fistula, which was managed with total parenteral nutrition. In addition, there were reports of recurrence after biopsy of the tumor. In our case series 2 of the 3 patients received a splenectomy because of the proximity of the tumor to the spleen. There were no intraoperative or postoperative complications. Follow-up length from 13 to 36 months revealed no evidence of recurrence.
Conclusions:
In the pediatric population, solid pancreatic pseudopapillary tumors located in the body or tail of the pancreas can be managed with a laparoscopic distal pancreatectomy.
Introduction
S
SPTs can be managed by a minimally invasive laparoscopic approach, given their low rate of malignancy. 2 These tumors are rare, seen more frequently in younger females, and usually occur in their third and fourth decades of life. Occasionally, they occur in children. 3 To date, there have been no genetic features and tumor markers identified to be associated with these lesions. However, a recent study by Laje et al. 4 has shown a unique immunostaining pattern for CD99 in surgical specimens. Surgery is the most definitive treatment because of its effectiveness as complete surgical resection results in favorable outcomes in 95% of cases. In comparative studies, the minimally invasive resection has been associated with superior cosmetic results, shorter hospital stay, quicker return to normal activities, lower complication rates, including intraoperative blood loss, and more successful splenic salvage. 2 Over 500 laparoscopic resections have been performed in adult patients, and although the technique is considered “advanced,” its adoption is gaining increased acceptance.2,5,6 In contrast, the application of laparoscopy for tumor resections in children is not reported frequently in the literature. We present our institutional series of 3 cases of children found to have a pancreatic mass. Given the rarity of pancreatic tumors in children, our presumptive diagnosis in each case was SPT. We discuss the minimally invasive management via the laparoscopic technique, review the current literature, and aim to enhance the pediatric case series literature on minimally invasive treatment of this rare tumor.
Case Reports
Case 1
A 14-year-old girl presented with 1 week of fever and right lower quadrant pain. Clinical and radiological evaluation with a computed tomography (CT) scan was consistent with a perforated appendicitis with diffuse phlegmon and an incidental finding of a 2.5-cm mass in the dorsal aspect of the tail of the pancreas (Fig. 1). She was treated with a course of intravenous antibiotics and underwent interval appendectomy 6 weeks later. At 2 months, a follow-up CT scan revealed a persistent perisplenic pancreatic mass measuring 2.2×1.8 cm, consistent with a solid tumor. She underwent diagnostic laparoscopy with the plan to perform a distal pancreatectomy. A 12-mm trocar was used through the umbilicus to accommodate the standard 10-mm 30° laparoscope and a 12-mm endoscopic stapler, as well as a 10-mm laparoscopic ultrasound probe. Three additional 5-mm trocars were used, at the right and left midaxillary lines and in the left midclavicular line. We approached the pancreas by taking down the gastrocolic ligament with a Harmonic® (Ethicon, a Johnson & Johnson Company, Somerville, NJ) scalpel, and full exposure to the pancreas was done by tacking the stomach to the anterior abdominal wall using transabdominal 2-0 polydioxanone (PDS™; Ethicon) sutures. Hook electrocautery and the Harmonic scalpel were used to dissect the pancreas. Proximal-to-distal dissection was carried out given the location of the tumor. Intraoperative findings, including an intraoperative ultrasound, revealed the mass to be abutting the splenic hilum. Therefore, she underwent a laparoscopic distal pancreatectomy with splenectomy.
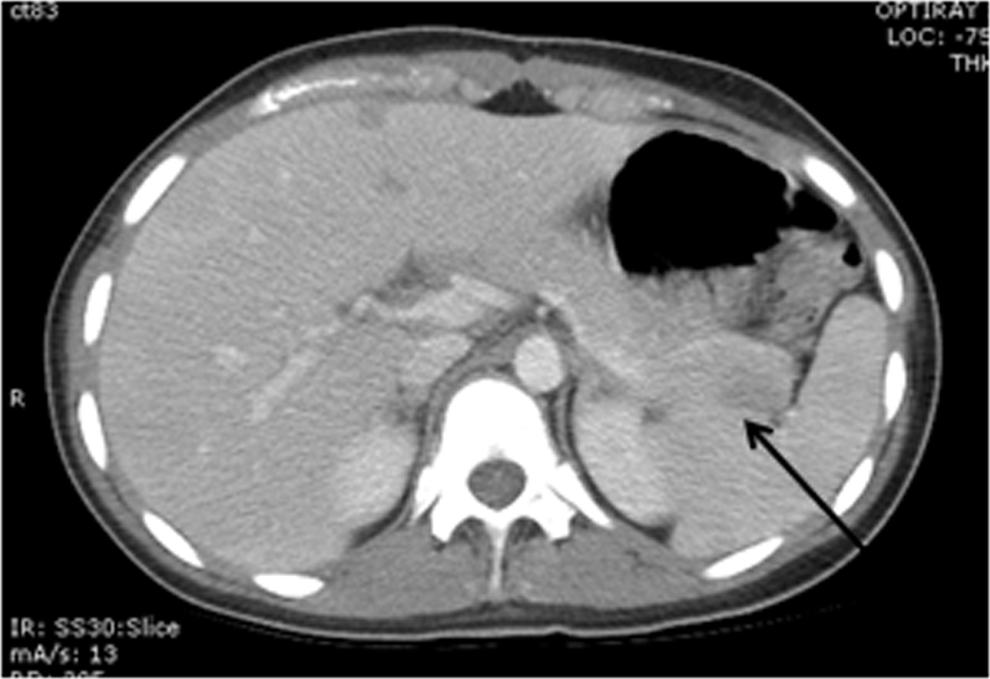
Computed tomography of a 2.5-cm solid pseudopapillary tumor that has low enhancement in the tail of the pancreas.
All cases were done in a similar fashion. Splenic preservation was attempted in all the cases. In 2 cases intraoperative ultrasound was used to verify the margins (Table 1 gives details).
ASA, American Society of Anesthesiologists.
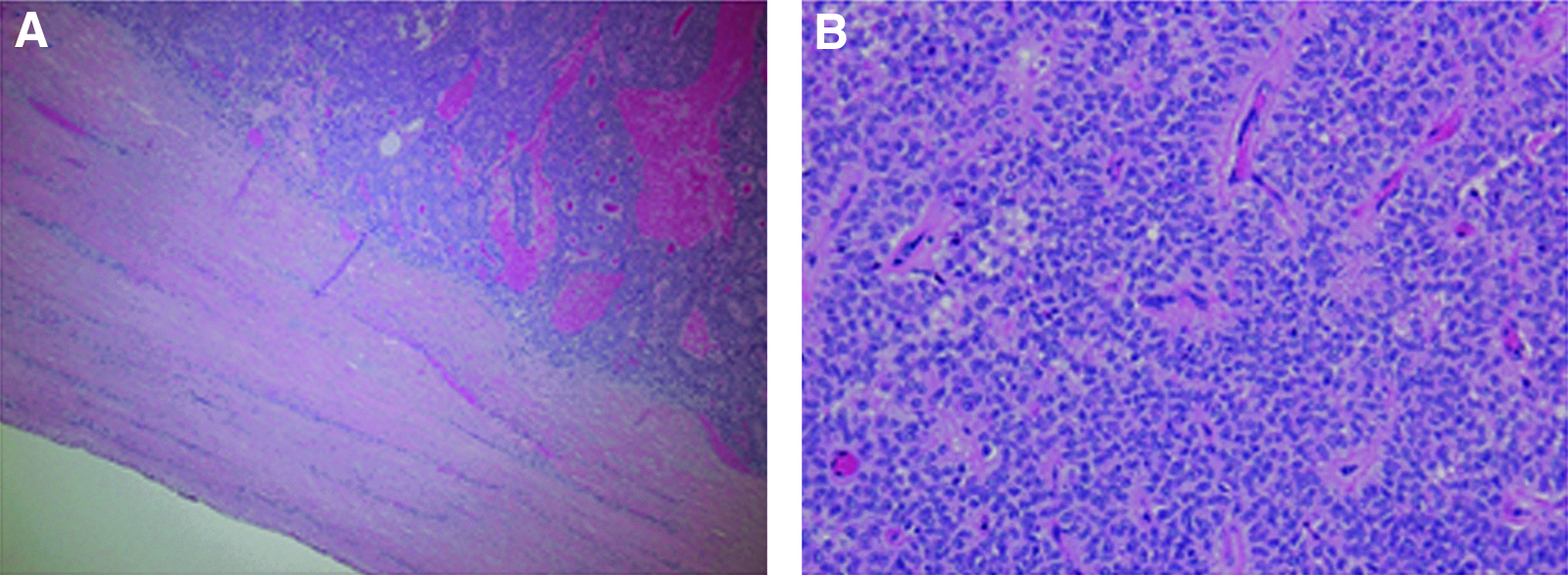
Pathology revealed an intact unilocular pancreatic mass measuring 2.1×1.2×1.1 cm that abutted but did not invade the splenic hilum. Microscopically, the mass was well circumscribed with a fibrous capsule (Fig. 2A) and consisted of medium-sized cells with round nuclei and a moderate amount of eosinophilic cytoplasm with a pseudopapillary architecture (Fig. 2B). The spleen appeared to be grossly normal. The proximal pancreatic margin was negative for tumor. The pathologic findings of the pancreas were consistent with an SPT. Her postoperative course and 13-month follow-up visit were unremarkable.
Case 2
A 13-year-old healthy girl was found to have a distal pancreatic mass on an abdominal CT scan that was obtained for the work-up of intermittent abdominal pain. Imaging revealed a 3-×2.5-cm mass in the distal pancreas that was consistent with a pancreatic tumor. Diagnostic laparoscopy revealed a mass in the body and tail of the pancreas with encasement of the splenic vein. Laparoscopic distal pancreatectomy with splenectomy was performed. Pathology revealed a 3-×2.1-×2.5-cm, poorly defined, bosselated, bilobed, and focally hemorrhagic lesion with cystic features. Microscopic examination showed areas of hemorrhage, papillary formation, and focal perineural invasion (Fig. 3). Surgical margins, splenic vein, and lymph nodes were negative for tumor. Her postoperative course was uneventful. There was no recurrence or evidence of metastatic disease on abdominal CT scan at the 3-year follow-up.
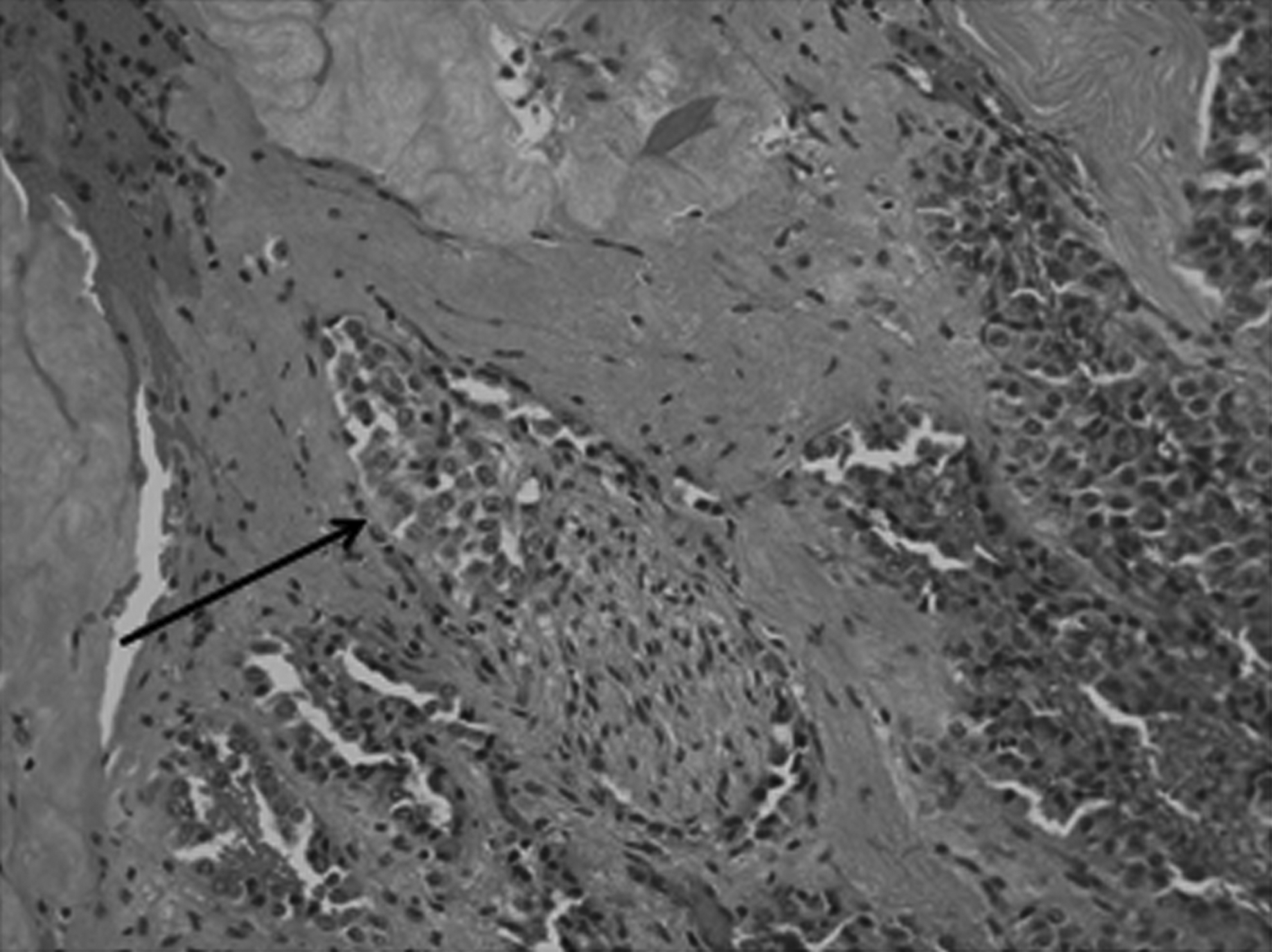
Solid pseudopapillary pancreatic tumor with perineural invasion.
Case 3
A 13-year-old girl with a history of sickle cell trait presented with abdominal pain and a palpable left upper quadrant mass on examination. An abdominal CT scan demonstrated a 13-×11-×9.4-cm solid mass originating in the body with extension into the tail of the pancreas without evidence of metastatic disease (Fig. 4). The patient underwent laparoscopic distal pancreatectomy with splenic preservation. Intraoperative ultrasound was used to confirm the normal proximal pancreatic margin and its anatomical relationship to the superior mesenteric vasculature prior to resection. The pathology revealed a well-circumscribed mass, 12×11×10.5 cm, weighing 711 g, with extensive central necrosis surrounded by a viable tumor forming solid sheets of pseudopapillary structures with a thick, fibrous capsule. Bland cells—pink cytoplasm with round nuclei and scattered mitoses—were present, and the proximal resection margin was negative for tumor. Her postoperative course was uncomplicated, and follow-up at 24 months showed no recurrent disease.
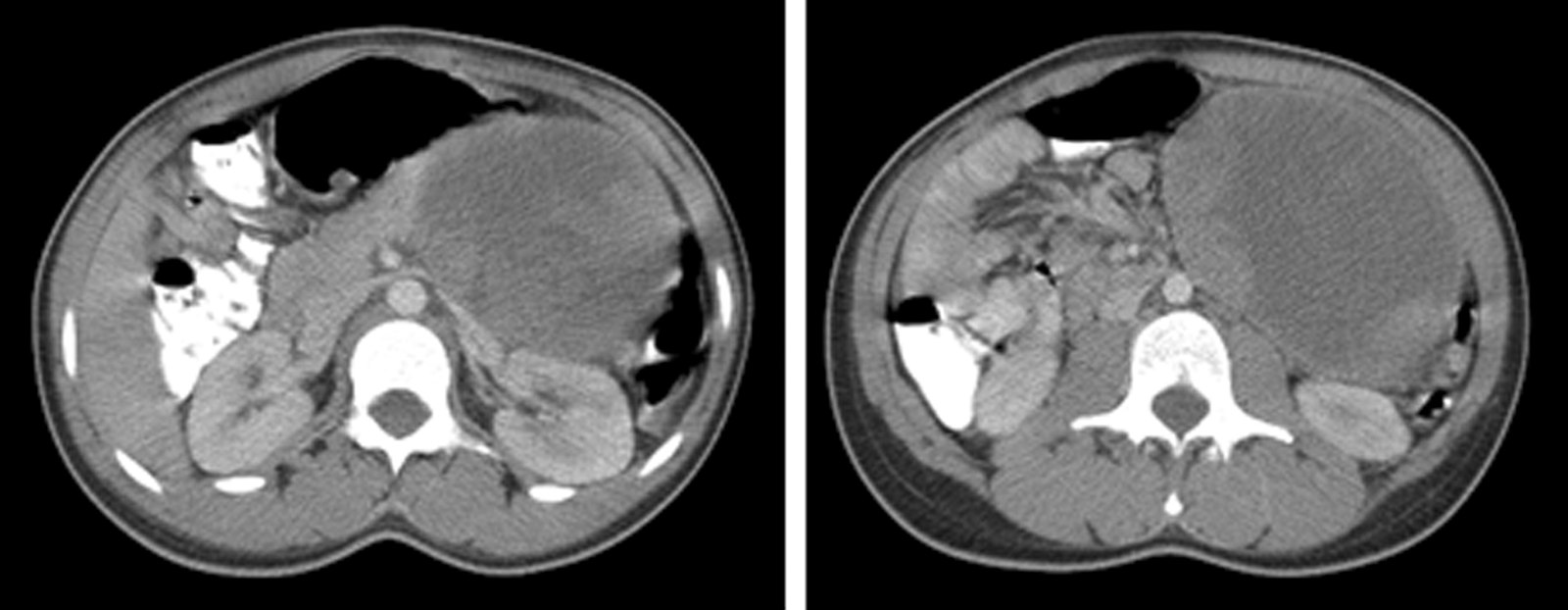
A large solid pseudopapillary tumor of the pancreas measuring 13×11×9.4 cm originating from the body of the pancreas. The mass is predominantly cystic with enhancing solid components.
Discussion
SPTs make up 1%–3% of pancreatic tumors. 7 It is more common in young women: 85% of patients are under 30 years of age, and 80% are female.5,7 These neoplasms rarely occur in males or in pediatric patients. The neoplasm is generally slow growing, with low malignant potential, and has one of the best prognoses of malignant pancreatic tumors in children. 8 SPTs appear as large, well-encapsulated masses with mixed solid and cystic components on ultrasonography and CT scan; however, they cannot be visualized well on magnetic resonance imaging.9,10 SPTs, however, are often misdiagnosed in children because they are rare and because symptoms associated with tumor compression of adjacent organs are not distinct. 11 The diagnosis is usually only confirmed by pathology, after surgical resection.2,12,13 Authors in some studies have obtained a preoperative diagnosis with biopsy,14,15 including endoscopic ultrasound scan with fine-needle aspiration. 16
Most SPTs are localized to the pancreas at the time of presentation, with metastasis in only 10%–15% of cases.9,13 Pancreatectomy is advocated for nearly every case of SPT and may be accompanied by duodenectomy or splenectomy, depending on the proximity of the lesion to these surrounding structures. Greater than 95% of tumors limited to the pancreas are cured by complete surgical resection. 17 Recurrence rate after complete resection is 10%. 15 The 5-year survival rate following surgery is 95%–98%. 18
In the 1990s, laparoscopic distal pancreatectomy was initially performed in adults. 2 Since then, over 500 procedures have been reported in the English literature, and retrospective analysis has shown that it has comparable morbidity with significantly shorter hospital stay and better cosmetic results than an open approach. In addition, laparoscopic distal pancreatectomy affords greater magnification and superior visualization of splenic vessels, aiding in splenic conservation, compared with the open approach. In a series of 58 consecutive laparoscopic distal pancreatectomies performed to treat solid and cystic tumors, Melotti et al. 19 reported shorter hospitalization, no conversions to open technique, and comparable rate of complications. The most prevalent complication for both laparoscopic and open operations is postoperative pancreatic fistula; reduction of this risk requires management of the pancreatic stump.
Thirteen laparoscopic pancreatectomy procedures have been reported in pediatric patients with SPTs. Ten of the tumors were located in the pancreatic tail, two were in the uncinate process, and one was in the central portion or body of the pancreas.5,9,10,13–15,20–22 Of the tumors resected with a laparoscopic distal pancreatectomy, only two included splenectomy because the splenic vessels could not be separated from the neoplasm and pancreas.20,23 In our series, 2 of the 3 patients required splenectomy because of the inability to separate the tumor from the spleen without risking spillage of tumor. In fact, the patient with by far the largest tumor (Case 3) was able to undergo laparoscopic distal pancreatectomy with splenic preservation because the tumor was located more proximally in the pancreas.
Complications after laparoscopic distal pancreatectomy have been reported by Fais et al., 15 who described three children, all of whom developed recurrences of SPT and were subsequently managed by open surgery. The distinction from our series is that each of those 3 patients underwent initial laparoscopic biopsy either prior to or at the time of resection. The third patient in that series underwent an initial laparoscopic biopsy followed by delayed resection. Carricaburu et al. 24 described a case of recurrence in a patient who received a laparoscopic biopsy prior to open resection of a SPT. Even when one considers an open resection for these types of pancreatic lesions in children, any type of biopsy is not recommended pre- or perioperatively.13,23 This likely had direct impact on tumor recurrence and peritoneal dissemination. Mukherjee et al. 20 reported one pancreatic fistula/pancreatic leak out of 2 pediatric patients who underwent laparoscopic distal pancreatectomy for SPT. The leak resolved after a 15-day course of total parental nutrition. The occurrence of a pancreatic fistula was not reported elsewhere in children, although adult studies have reported it as a common complication in both laparoscopic and open distal pancreatectomy (0%–26% versus 0%–32%, respectively). 20
Given the low incidence of SPTs, especially in children, a randomized trial of laparoscopic distal pancreatectomy to treat this tumor is not feasible. Cavallini et al. 13 performed a retrospective review in 2011 of 10 patients (8 women, 2 men) who underwent a laparoscopic pancreatectomy for this tumor. Three of the patients in their series were children (11, 13, and 17 years of age). For all 10 patients there has been no evidence of tumor recurrence (median follow-up, 47 months). Although they concluded that laparoscopic surgery is a safe approach for tumor removal, they suggested that application in pediatric cases is still under development.
According to the available literature and our own results, it appears that compared with open surgery, laparoscopic resection of SPT in children is an acceptable approach when applied in the appropriate clinical setting (e.g., tumors in body or tail versus head of the pancreas).7,13,24 Although there are no standardized protocols for postsurgical follow-up, it is essential to follow these patients for a minimum of 5 years as this is the time during which most recurrences are experienced. Our follow-up consists of yearly evaluation along with CT scan. Alternatively, ultrasonic evaluation may be considered for follow-up in these patients; however, this has not been done by our institution. Splenic conservation may be possible, depending on the proximity of the SPT to the spleen and the involvement of splenic vessels with the tumor, as with the open procedure. In the hands of an experienced surgeon, laparoscopic distal pancreatectomy could be the preferred method of treatment for SPT in pediatric patients.
Footnotes
Disclosure Statement
No competing financial interests exist.