
Abstract
Abstract
Background:
Few reports have examined the impact of laparoscopic approach on survival outcomes in patients with early-stage (IA2–IB1) cervical cancer (CC). In this study we aimed to compare disease recurrence and survival outcomes of total laparoscopic radical hysterectomy (TLRH) with those for open radical hysterectomy (ORH) and pelvic lymphadenectomy in patients with early-stage CC.
Patients and Methods:
A single-center, retrospective analysis was conducted in a total of 68 patients who treated with TLRH (n=22) or ORH (n=46) between 2007 and 2010. The primary endpoint of the study was progression-free survival (PFS).
Results:
Median follow-up time was 42.50 months (range, 38.40–55.42 months) for the TLRH group and 43.50 months (range, 37.66–52.65) for the ORH group. The study groups were comparable in terms of baseline characteristics except the ORH group had more patients with tumor size greater than 2 cm (P=.026), depth of stromal invasion greater than 33% (P<.0001), and International Federation of Gynecology and Obstetrics stage IB1 disease (P=.019). However, these factors had no impact on overall and PFS in Cox regression analyses. In total, three recurrences were observed in the TLRH group. Two of the 3 patients were alive with no evidence of disease, and the remaining individual was alive with disease (AWD). In the ORH group, 5 patients had recurrences. Two of the 5 patients died of disease, and three were AWD. The estimated 3-year PFS (86.1% versus 90.6%, respectively; P=.32) and overall survival (100% vs. 95.4%, respectively; P=.82) were comparable in the TLRH and ORH groups.
Conclusions:
TLRH and ORH have similar survival outcomes in patients with early-stage CC.
Introduction
M
In the current study, we evaluated the impact of laparoscopic approach on disease recurrence and survival outcomes in patients with early-stage (stage IA2–IB1) CC.
Patients and Methods
Study design and patients
In total, 96 patients with CC who underwent surgery at Akdeniz University Hospital, Antalya, Turkey, between 2007 and 2010 were retrospectively analyzed. Demographic, clinicopathologic, and survival data, including the age at surgery, date and type of surgical procedure, histological type, tumor size, depth of stromal invasion, lymphovascular space invasion (LVSI), length of parametria resected, parametrial involvement, length of vaginal edge resected, surgical margin involvement, number of lymph nodes (LNs) removed, LN involvement, stage of the disease, adjuvant treatment, disease recurrence or progression, survival status, and the date of last follow-up, were extracted from the institutional database, operative notes, and patient charts following Institutional Review Board approval.
Patients were included to the analysis if they had International Federation of Gynecology and Obstetrics (FIGO) stage IA2 or IB1 disease and a surgical procedure performed via laparoscopy or laparotomy that included radical hysterectomy with pelvic lymphadenectomy as primary treatment. Exclusion criteria were FIGO stage IB2 or more advanced disease, the use of chemotherapy, radiotherapy, or chemoradiotherapy as primary or neoadjuvant treatment, presence of intraperitoneal disease or LN involvement detected during intraoperative observation and frozen section examination, or patients with no survival data.
Procedures
As a routine procedure at our institution, patients with newly diagnosed untreated invasive CC are offered treatment with TLRH if they had FIGO stage IB1 or less disease, a body mass index of ≤35 kg/m2, or no pregnancy, history of previous abdominal radiotherapy, or evidence of metastatic disease by imaging studies. During the counseling period, we clearly declare the common known advantages and disadvantages of the laparoscopic technique to all patients, including less postoperative discomfort, shorter hospital stays, less convalescence time, less blood loss, and lower wound infection rates versus longer operative time, technical difficulties, the possibility of conversion to open laparotomy, and unclear oncologic outcomes with regard to the tumor recurrence and dissemination through the port site or peritoneum. However, the final decision for TLRH or conventional open abdominal radical hysterectomy (ORH) is at the patients' discretion.
Both open and laparoscopic procedures were performed with the patient under general anesthesia. Patients underwent bowel preparation and were administered perioperative antibiotics. Ureteral catheters or stents were not used routinely. All patients underwent insertion of a Foley urinary catheter, and it was usually removed within 5 days following the surgery. During the surgery, first, the abdominal cavity was inspected, and the parametria and pelvic LNs were palpated. If a gross parametrial extension, intraabdominal disease, or a bulky metastatic LN was identified, the radical hysterectomy was abandoned, and the procedure was converted to paraaortic lymphadenectomy and/or pelvic LN debulking. Otherwise, first, the systematic pelvic lymphadenectomy was performed with the removal of external iliac, internal iliac, and obturator LNs. Suspicious, enlarged LNs were sent for frozen section analyses. If a positive pelvic LN was identified, then the radical hysterectomy was also terminated, and the LN dissection was extended to the paraaortic region up to the renal vessels as mentioned above. If the frozen section examination revealed no evidence of pelvic LN metastasis, then the Type C1 radical hysterectomy was completed as described by Querleu. 6 Both approaches were similar with regard to the extent of resection and surgical technique.
The port placement and operating procedures for the laparoscopic approach were carried out as reported previously. 7 TLRH was performed using scissors and monopolar cautery for the dissection of the paravesical space, pararectal space, perivascular soft tissues, retroperitoneum, and small vessels, and the LigaSure™ vessel sealant device (ValleyLab, Boulder, CO) or bipolar cautery was used for the isolation and ligation of gonadal vessels, uterine artery, uterine vein, and paracervical tissue. A vaginal probe (Apple Medical Corp., Marlboro, MA) was used to facilitate the dissection and excision of vaginal edges. The LNs and uterus was removed by using endobags through the port site and vagina, respectively.
Our institutional protocols for the postoperative adjuvant treatment of CC includes cisplatin-based concurrent chemoradiation for patients with positive pelvic LN, positive surgical margin, and/or positive parametrium, and pelvic irradiation alone is used for patients with at least two of the following risk factors: (1) ≥33% stromal invasion, (2) LVSI, and/or (3) tumor size of >4 cm.
The standard surveillance practice of our institution was to follow-up patients who achieved a complete remission or no evidence of disease after initial treatment every 3 months for 2 years, every 6 months for the next 3 years, and then annually.
Statistical analysis
We expressed data as median and interquartile range (IQR) for continuous variables. We report binary variables as counts and percentages. When appropriate, we compared groups with a Mann–Whitney U test, Student's t test, or chi-squared test.
The primary outcome was progression-free survival (PFS), and the secondary outcome was overall survival (OS). We measured PFS from the date of surgery to the date of disease progression or relapse or death from any cause, and OS was defined from the date of surgery to the date of death from any cause. Patients alive without progression or relapse were censored at the date they were last known to be alive in PFS analyses. Patients still alive were censored at the date they were last known to be alive in OS analyses. The log-rank test was used to compare the Kaplan–Meier curves for PFS and OS. The Cox proportional hazards model was used to obtain the hazard ratio for the treatment comparison and its 95% confidence interval, unadjusted or adjusted for all factors. All P values were two-sided with the level of significance set at <.05. The statistical analysis used the Stata software package (Special Edition version 11.2 for Macintosh OSX; StataCorp, College Station, TX).
Results
Patient characteristics
In total, 96 patients were assessed for inclusion. Twenty-eight patients were excluded from the analysis: 5 had stage IA1 disease, 9 had stage IB2 disease, 2 underwent primary radical abdominal trachelectomy, 6 underwent radical parametrectomy with upper vaginectomy for the treatment of occult invasive CC detected during previous simple hysterectomy, 4 received chemoradiotherapy, and 2 had no survival data. Thus, final analyses were performed in a total of 68 patients, including 46 patients in the ORH group and 22 patients in the TLRH group.
Table 1 compares the clinical and pathological characteristics of patients. The median follow-up time was 42.50 months (IQR, 38.40–55.42 months) for the TLRH group and 43.50 months (IQR, 37.66–52.65 months) for the ORH group. All patients were followed up for longer than 36 months. Study groups were comparable for age (P=.096), tumor histology (P=.41), tumor size (P=.11), LVSI (P=.08), length of parametria resected (P=.80 for the right and P=.83 for the left), parametrial involvement (P=0.71), length of vagina resected (P=.27), surgical margin involvement (P=1.00), number of LNs removed (P=.23), LN involvement (P=.72), and adjuvant treatment (P=.50).
CI, confidence interval; FIGO, International Federation of Gynecology and Obstetrics; IQR, interquartile range; SD, standard deviation.
The ORH group had more patients with tumor size of ≥2 cm (P=.026), depth of stromal invasion ≥33% (P<.0001), and stage IB1 disease (P=.019). However, the univariate analysis revealed no relationship between any of those parameters and progression or death (Table 2).
Unadjusted and adjusted data, if any, were obtained by univariate and multivariate analyses, respectively.
CI, confidence interval; FIGO, International Federation of Gynecology and Obstetrics; HR, hazard ratio.
Survival analysis
TLRH was associated with similar survival outcomes in comparison with ORH. The estimated 3-year PFS was 86.1% and 90.6% for the TLRH and ORH groups, respectively (P=.32). The 3-year OS was 100% and 95.4% for the TLRH and ORH groups, respectively (P=.82) (Figs. 1 and 2 and Table 3).
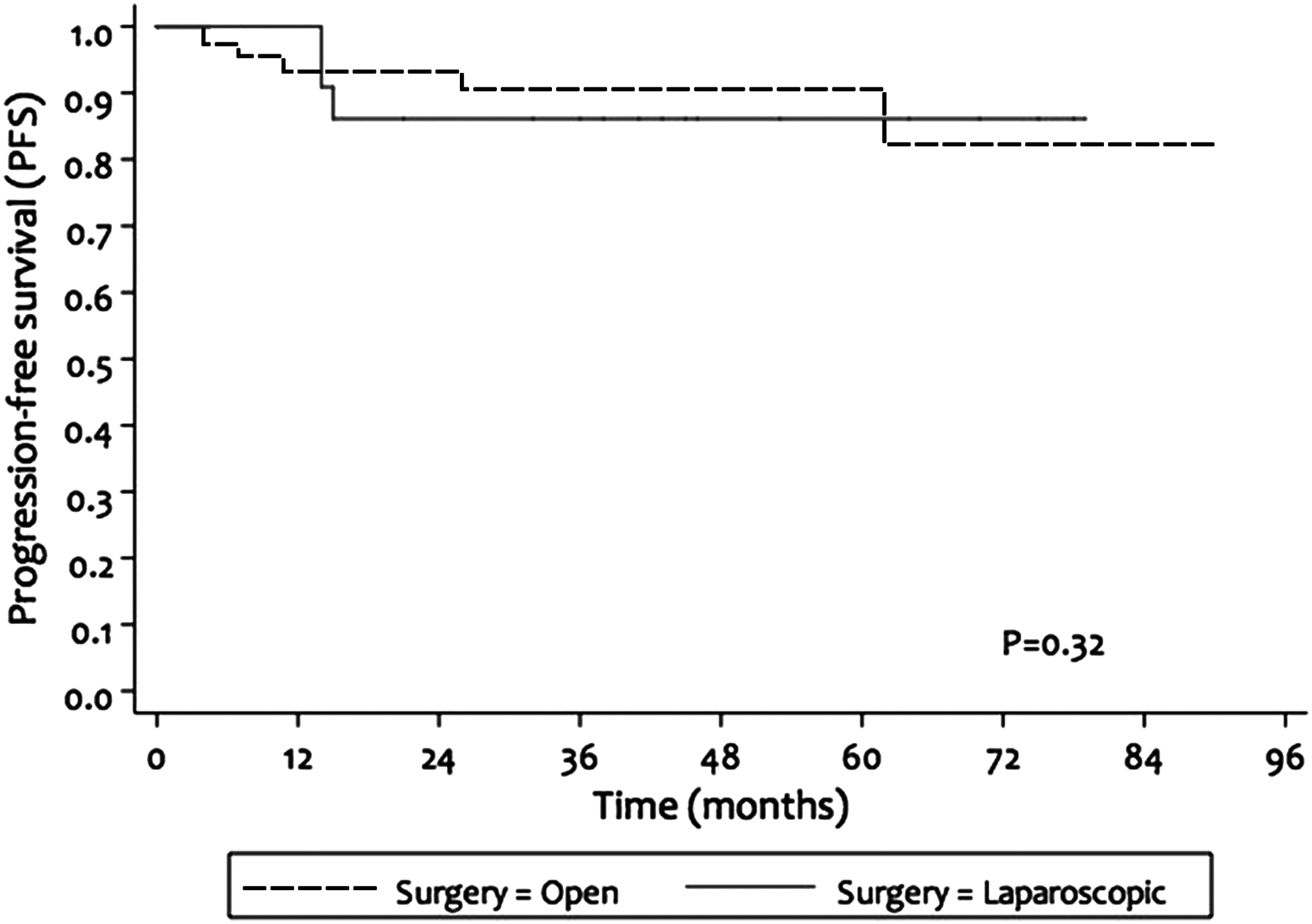
Progression-free survival analyses.
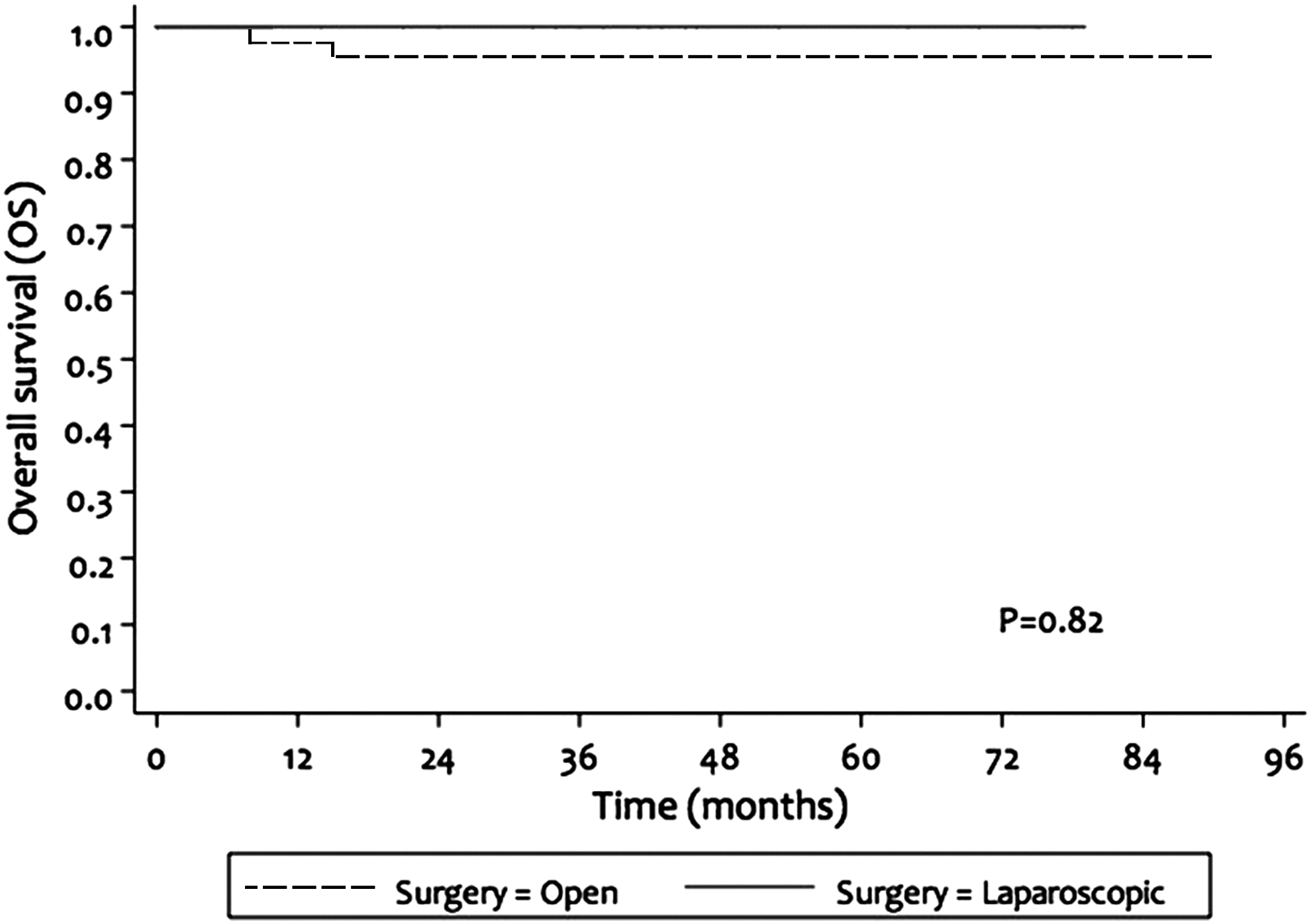
Overall survival analyses.
CI, confidence interval; HR, hazard ratio; NR, not reached; OS, overall survival; PFS, progression-free survival.
We observed a total of eight recurrences, including three (13.6%) in the TLRH group and five (10.9%) in the ORH group. Clinical and demographic features of patients with recurrent disease are summarized in Table 4. All patients with disease recurrence had FIGO stage IB1 disease.
Adeno-ca, adenocarcinoma; Adeno-sq, adenosquamous carcinoma; AWD, alive with disease; Chm-rad, chemoradiation; Chmt, chemotherapy; DOD, dead of disease; DSI, deep stromal invasion; LCNEC, large cell neuroendocrine carcinoma; LN, lymph node; LN Inv, lymph node involvement; LVSI, lymphovascular space involvement; NED, alive with no evidence of disease; ORH, open radical hysterectomy; Prmt Inv, parametrial involvement; RT, radiotherapy; SMI, surgical margin involvement; Sq cell, squamous cell carcinoma; TLRH, total laparoscopic radical hysterectomy; WLE, wide local excision.
In the TLRH group, 1 of the 3 patients had squamous cell carcinoma; positive LVSI was the only risk factor for disease recurrence. She received no adjuvant treatment. Liver metastasis was observed 14 months after the surgery. She is still under treatment with chemotherapy and alive with disease (AWD). The second patient had no risk factor for recurrence. She had endocervical adenocarcinoma, 1 cm in diameter. She did not receive adjuvant treatment. She underwent vaginal cuff recurrence 14 months following the surgery, was treated with radiotherapy, and is still alive with no evidence of disease. A port-site metastasis was detected 15 months after the primary surgery in the last patient. She had adenosquamous carcinoma. Microscopic LN involvement was detected in the final pathology. She received adjuvant chemoradiation. She presented with a suspicious 3-cm soft tissue mass around the left paramedian port site. This was treated with wide local excision of the recurrence and the port-site track and further treated with external beam irradiation. She is alive with no evidence of disease.
In the ORH group, 2 of the 5 patients with recurrence died. One had large cell neuroendocrine carcinoma with pelvic LN involvement, received adjuvant chemoradiotherapy, and died 8 months following the recurrence. The other one had squamous cell carcinoma, deep stromal invasion, large tumor size, and positive LVSI, received adjuvant chemoradiotherapy, and died 12 months after the recurrence. Both recurrences occurred as either local-regional or distant metastasis. Three of the 5 patients with recurrent disease are AWD. One had endocervical adenocarcinoma with parametrial involvement; and received adjuvant chemoradiotherapy. She developed lung metastasis and pelvic side-wall recurrence 26 months after the primary surgery. The other 2 patients had squamous cell carcinoma. They received adjuvant pelvic irradiation alone due to LVSI and deep stromal invasion. One of them developed multiple metastatic masses fixed to the abdominal wall 6 months after the primary surgery, and the other one developed lung metastasis 62 months following the primary surgery. Both patients were further treated with chemotherapy for recurrence.
Discussion
Wertheim 8 first described the radical abdominal hysterectomy for the surgical treatment of CC more than a century ago. Later, this radical approach became the basis for the treatment with minor modifications. In the 1990s, Canis et al. 9 and Nezhat et al. 10 described the laparoscopic technique for this surgery. This led to the questioning of the role of classical ORH, especially in early-stage disease. Following these initial reports, a certain number of studies assessed the surgical outcomes of TLRH and indicated the feasibility and safety of this procedure.1–5 However, only a few reported the survival outcomes.11–14
The current study represents the comparison of TLRH with ORH for patients with early-stage (IA2–IB1) CC. The study showed that surgical and survival outcomes of the laparoscopic and classical open modalities were comparable. We did not require conversion to laparotomy in any of the TLRH procedures. We observed three (13.6%) recurrences in the TLRH group. All had clinically FIGO stage IB1 disease, and recurrences occurred within the first 18 months.
In a study including 78 consecutive patients with stage IA2 and IB disease, Spirtos et al. 11 reported eight recurrences (10.3%) and five deaths in patients who underwent TLRH with lymphadenectomy during 3 years of follow-up. This was the first report providing information about the recurrence rates and survival data of this approach. The estimated 5-year OS and disease-free survival for the entire cohort were 93.6% and 89.7%, respectively. Three of 8 patients had a recurrence on the pelvic side wall, 1 patient had recurrence on the vaginal cuff, and the others had distant metastasis. Pomel et al. 12 reported a 6% recurrence rate in a series of 50 patients with stage IA2 and IB1 disease. The median follow-up time was 44 months, and the estimated 5-year OS and disease-free survival were 96.8% and 90.5%, respectively. In a recent study examining the role of TLRH as the standard surgical modality in stage IA2–IIA disease, Hong et al. 13 reported the results of consecutive 118 patients. The median follow-up time was 31 months. Eight (6.8%) patients had recurrence. The 3-year relapse-free survival and the OS were 92% and 95%, respectively. However, these studies did not include a control group and were not designed for the survival comparison.
Recently, in a matched cohort study, Nam et al. 14 reported that TLRH (n=263) and ORH (n=263) groups were comparable in terms of 5-year relapse-free survival (92.8% versus 94.4%, respectively; P=.49) and OS (95.2% versus 96.4%, respectively; P=.45). Sixteen patients in the TLRH group and 15 in the ORH group had relapsed disease (P=1.000), and 12 and 11 patients in each group died of disease, respectively (P=1.000). In the TLRH group, primary sites of recurrences were the vaginal cuff in 2 patients, the pelvic cavity in 5, regional LNs in 5, and distant organs in 4. However, approximately 12% of patients had stage IB2 and IIA disease in this study. Our results confirmed that TLRH and ORH had similar disease outcomes in early-stage CC.
Our results are comparable with those of previous reports. Strengths of our study include the administration of standard adjuvant treatment according to certain pathologic risk factors, the adequacy of relatively uniform surgical procedures/techniques performed by subspecialized gynecologic oncologists, and the detailed analysis of various clinicopathologic factors those may have an impact on prognosis. Potential limitations of our study include possible entry bias with case selection, the relatively short median follow-up time, and the small number of patients, especially in the TLRH group. However, selection bias is an inevitable risk of retrospective studies. The rarity of CC in our region is also a barrier to reach a satisfactory sample size.
Conclusions
Based on our results and available data in the literature, the laparoscopic approach may be a safe and feasible procedure with comparable surgical and survival outcomes compared with conventional ORH. The small sample size and nonrandomization do not allow a concrete conclusion. However, the number of patients included in most series is too small to draw conclusions. So, we think that the results of the current study are important. Multicenter prospective randomized controlled trials with longer follow-up are needed to determine the impact of the laparoscopic approach on long-term oncological outcomes with a high level of scientific evidence.
Footnotes
Disclosure Statement
No competing financial interests exist.