
Abstract
Abstract
Introduction:
We previously reported our experience with standard laparoscopic ileocecectomy, but we have recently used a single-incision laparoscopic approach.
Patients and Methods:
We conducted a retrospective review of a single surgeon's experience from 2009 to 2013.
Results:
Twenty-eight children 11–18 years of age (mean, 15.5 years) with a mean body mass index of 18.9±3 kg/m2 underwent single-incision laparoscopic ileocecectomy for Crohn's disease. Mean operative time was 86.5±25.9 minutes (range, 56–166 minutes). There were no extra ports placed or conversions to open surgery. Five children (18%) were on parenteral nutrition at time of surgery, 14 (50%) were on steroids, and 9 (32%) were on tumor necrotic factor inhibitors. A stapled extracorporeal anastomosis was performed in all children. Complications included abscess (n=4), small bowel obstruction (n=3), superficial wound infection (n=3), and small bowel perforation (n=1). Some patients had more than one complication. Of those with complications, 5 (56%) were on steroids, 5 (56%) were on tumor necrotic factor inhibitors, and 1 patient was on both. The perforation occurred at a point of adhesiolysis also involved with Crohn's disease. There were no anastomotic leaks. Median follow-up was 17 months (range, 1–47 months).
Conclusions:
Single-incision laparoscopic ileocecectomy is safe and feasible in pediatric patients with Crohn's disease.
Introduction
I
Although single-incision laparoscopic ileocectomy has been described in adults, only a handful of pediatric cases has been published.1,2,4,11,12 Therefore we present our experience with pediatric single-incision laparoscopic ileocecectomy to document outcomes and identify variables associated with complications from these procedures.
Patients and Methods
We conducted a retrospective review of a single surgeon's experience with single-incision laparoscopic ileocecectomy for Crohn's disease from June 2009 to January 2013. Institutional review board approval was obtained prior to data collection. Demographic data, operative details, and outcomes were recorded.
Data analysis was performed using the chi-squared test with Yates's correction where appropriate for categorical variables. Children with complications were compared with those without complications. Values of P<.05 were considered significant.
Operation
A vertical incision was made through the center of the umbilicus, and a sheath for a 5-mm Step™ bladeless trocar (Covidien Surgical, Norwalk, CT) was placed through the center of the umbilical stalk. After insufflation, a stab incision was used about 1 cm on each side of the trocar to place 5-mm working instruments directly through the fascia (Fig. 1). These instruments usually seal the hole traversed to maintain insufflation. Additionally, we turned the flow up to the near-maximum rate to assure that air potentially leaking from these sites will not influence the working space.

Intraoperative image of port placement.
The cecum and terminal ileum were mobilized by taking down the lateral colonic attachments, which can be done bluntly or with scissors. The right colon is usually simple to mobilize up to the hepatic flexure, which needs to be taken down; otherwise, it prevents bringing up enough right colon for a simple anastomosis. Finally, the base of the mesentery was mobilized off the retroperitoneum such that the ileal region can be grasped and pushed easily up over the top of the transverse colon. This mobilization overcomes the difficulty of a short, thick ileal mesentery, which is often created by the disease. The base of the appendix was then grasped, the trocar was removed, and the three incisions were connected using the laparoscopic instruments in the inferior and superior incisions as a guide to cauterize over (Fig. 2A). The incision usually needs to be incrementally enlarged until the affected area of bowel can be brought out (Fig. 2B).
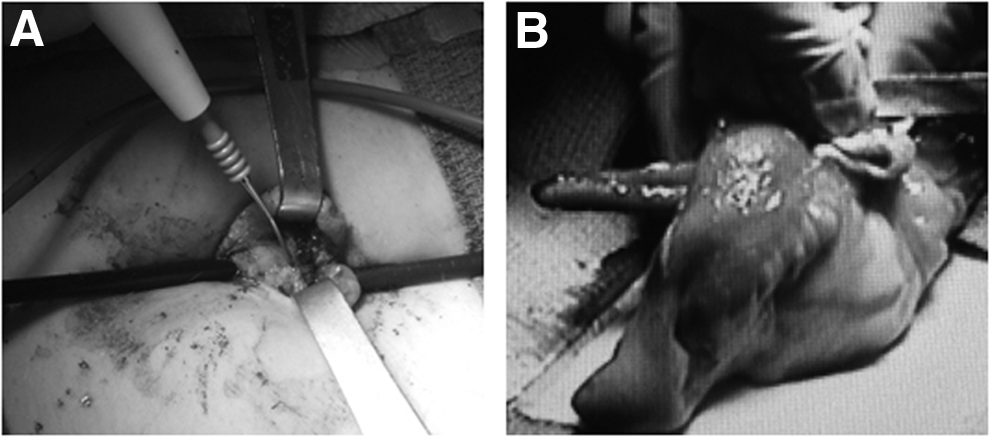
Intraoperative images.
Resection and anastomosis were then performed extracorporeally by surgeon preference, and after placing the anastomosis in the abdomen, one can decide if another look in the abdomen is required. If abdominal re-inspection was required, such as running the bowel to assess for other lesions, a multilumen port, such as the SILS™ three-lumen port (Covidien, Mansfield, MA), can easily be placed in the enlarged umbilical defect to assure adequate insufflation and working capacity.
Results
Between June 2009 and January 2013, 28 children 11–18 years of age (mean, 15.5 years) with a mean body mass index of 18.9±3 kg/m2 consecutively underwent a primary single-incision laparoscopic ileocecectomy for Crohn's disease. The majority of the children were female (19 [68%]). Mean time from Crohn's disease diagnosis to the operation was 2.2±2.6 years. There were no extra ports placed or conversions to the open approach. Indications included pain (n=13), obstruction/stricture (n=11), perforation (n=2), mass (n=1), and failure to thrive (n=2). One child had more than one indication.
Mean operative time was 86.5±25.9 minutes (range, 56–166 minutes). A stapled extracorporeal anastomosis was performed in all cases. There were no diverting ileostomies used. There were two incidental abscesses found at operation. Five children (18%) were on parenteral nutrition at time of surgery, 14 (50%) were on steroids, and 9 (32%) were on tumor necrotic factor inhibitors (7 on infliximab [Remicade®; Janssen Biotech, Inc., Horsham, PA] and 2 on adalimumab [Humira®; Abbott Laboratories, Abbott Park, IL]). Seven children (25%) had unscheduled re-admissions within 30 days from operation.
Nine children (32%) developed a total of 11 postoperative complications: abscess (n=4), small bowel obstruction (n=3), superficial wound infection (n=3), and small bowel perforation (n=1). There were no anastomotic leaks. Average postoperative day of complication was 8±6 days. Two of these complications were in children who had incidentally discovered abscesses at the time of surgery (one small bowel obstruction and one small bowel perforation).
Three children (11%) required a repeat abdominal operation. In one child, this was due to a small bowel perforation at a point of adhesiolysis on postoperative Day 3. The area of perforation was histologically confirmed to be involved with Crohn's disease. Another child required further exploration because of a small bowel obstruction on postoperative Day 17. The third child required repeat exploration on postoperative Day 1 due to tachycardia, fever, and peritoneal signs. She was found to have an intraluminal hematoma and partial obstruction at exploratory laparoscopy.
Of those with complications, 3 patients were on total parenteral nutrition, 5 were on steroids, and 5 were on Remicade (1 patient was on both steroids and Remicade). There were no significant correlations between the use of immunosuppression and development of complications. No children on Humira developed complications. Two children developed subsequent Crohn's disease complications requiring re-operation: one small bowel resection due to stricture proximal to the previous operation and one orchiectomy with debridement for paratesticular abscess likely due to fistulization.
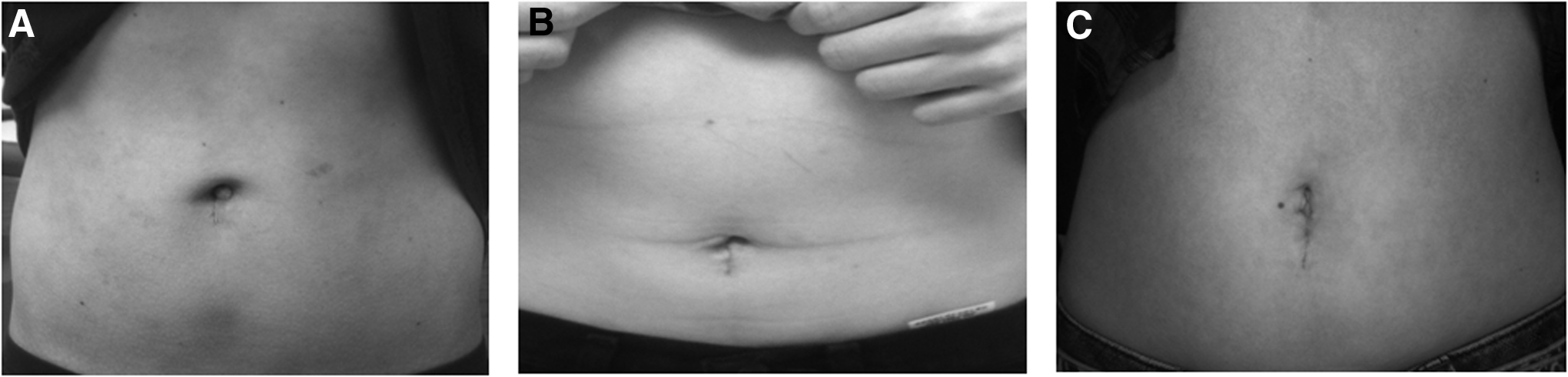
The mean number of postoperative days to a clear liquid diet was 1±1 day, and to a regular diet was 3±1.7 days. Mean length of stay was 6±4 days (range, 2–18 days). At the time of last follow-up, average number of bowel movements was 5/day (range, 1–11 bowel movements/day). Median follow-up was 17 months (range, 1–47 months). Cosmetic outcomes, although not objectively measured, appeared favorable in most cases, with no patient or parent concerns expressed about the appearance (Fig. 3).
Discussion
Laparoscopic ileocecectomy has been shown previously to be both safe and effective for the treatment of medically refractory Crohn's disease in pediatric patients. 1 Laparoscopic ileocecectomy has been shown to have advantages, including decreased adhesion formation, blood loss, length of stay, analgesic requirement, and earlier return of bowel function and convalescence.11,13–21
This report outlines our first experience with 28 consecutive single-incision laparoscopic ileocecectomies, which were all successfully completed without the use of addition ports or conversion to an open procedure. The mean operative time of 86 minutes compares favorably with the published average operative time in adult single-site ileocecectomy of 137 minutes. 12 Although this is not a comparative study, our overall outcomes are similar to previously published reports of single-incision laparoscopic ileocecectomy when compared with the standard laparoscopic counterpart.22,23 Given that the two children who had incidentally discovered abscesses at time of surgery developed complications (one small bowel obstruction and one small bowel perforation), the evidence of an abscess at time of surgery may increase the risk of postoperative complications. It is interesting that, although 55% of those children who developed postoperative complications were on steroids, 56% were on Remicade, and 33% were on total parenteral nutrition at the time of surgery. Although these factors did not correlate with a significant increased risk of postoperative complications, this study was likely underpowered to find such an association.
As opposed to most abdominal operations, where the single-site approach crowds the hands, decreases triangulation, and increases surgical difficulty, the ileocectomy is not particularly more difficult than the standard laparoscopic approach.8,10 This is because the final length of the umbilical incision will be determined by the size of the inflammatory mass. Knowing that, even with a small area of inflammation, the incision will need to be large enough to reduce the anastomosis, the surgeon can begin with an incision about 2 cm outside the umbilical ring. This provides enough room, combined with the distance of the umbilical ring, to place two working instruments with enough triangulation to allow natural laparoscopic movements (Fig. 1). This technique also requires no specialized laparoscopic instruments, decreasing complexity and cost.12,17,24 The only example of specialized equipment we periodically used was a SILS three-lumen port if re-inspection of the abdomen was desired after reduction of the anastomosis. This large gel port creates a nice seal in the now larger incision and allows instrument access for inspecting the bowel and suctioning. This prevents the cumbersome maneuver of partial umbilical closure over a port, which provides a generally poor seal and limits instrumentation.
Thus single-incision laparoscopic ileocecectomy is safe and feasible in pediatric patients with medically refractory Crohn's disease and is our method of choice.
Footnotes
Disclosure Statement
No competing financial interests exist.