
Abstract
Abstract
Background:
Minimal access surgery is moving toward reduced size and fewer ports. The aim of this article is to describe our experience with the intrahepatic Glissonian approach for single-port laparoscopic left lateral sectionectomy.
Subjects and Methods:
We have performed this procedure on 8 consecutive patients. A transumbilical incision is performed, and a single-incision platform is introduced. The operation begins with ultrasound examination of the liver. Intrahepatic Glissonian access of the portal pedicle from segments 2 and 3 is performed, and the pedicle is divided with a stapler. The liver is transected, and the left hepatic vein is divided with a stapler. A surgical specimen is retrieved through the single umbilical incision. No drains are left in place.
Results:
The median operative time was 68 minutes, and there was minimal bleeding. The median hospital stay was 1 day. Six patients were operated on for liver adenoma. There was no morbidity or mortality. During follow-up (median, 12 months), no patient developed incisional hernia. The cosmetic appearance of the incision was excellent in all cases.
Conclusions:
Single-port laparoscopic left lateral sectionectomy is feasible and can be safely performed in specialized centers.
Introduction
I
Liver surgery is an extremely challenging field, and surgical management of liver diseases continues to grow. Laparoscopic liver resection has been increasingly used in the past decade.5–7 However, among the several types of laparoscopic liver resection, left lateral sectionectomy (i.e., the removal of segments 2 and 3) is the only one being considered as the gold standard. 8 The purpose of this article is to describe our initial experience with 8 consecutive cases of single-port laparoscopic left lateral sectionectomy. A detailed technical description with standardization is provided. 7 To the best of our knowledge, this is the largest single-port laparoscopic left lateral sectionectomy series in the English literature.
Subjects and Methods
Between July 2012 and July 2013, eight single-port laparoscopic left lateral sectionectomies were performed. The patients were informed about the advantages and risks of the technique, and they gave their consent for its use.
Surgical technique
The patient is placed in a supine and reverse Trendelenburg position with the surgeon between the patient's legs. The first assistant is positioned on the right side of the patient with the monitor placed on the patient's cranial side. With the patient under general anesthesia, a transumbilical 3-cm skin incision is made. A single-incision advanced access platform with a gelatin cap, a self-retaining sleeve, and a wound protector (GelPoint®; Applied Medical, Rancho Santa Margarita, CA) is introduced through this incision (Fig. 1a).
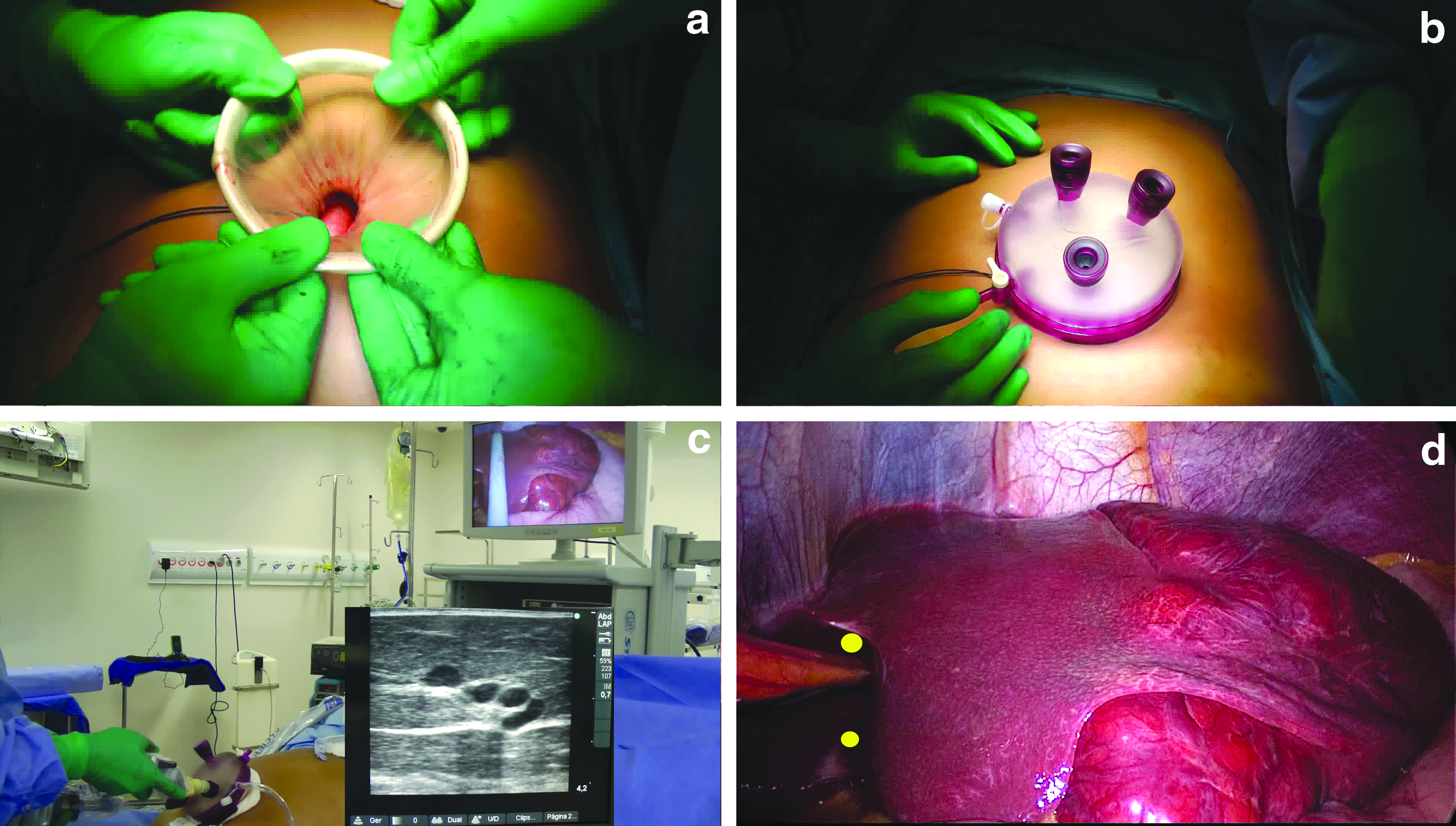
The single-port platform setup and intraoperative ultrasound.
Three trocars (5–11 mm) are introduced through the single-port device. No articulated instruments are required because of the gel cap and sleeves. CO2 pneumoperitoneum is established at 12 mm Hg. A rigid 30° 10-mm laparoscope is introduced. This single-port platform is able to accommodate three or four instruments at the same time with no triangulation prejudice (Fig. 1b). We used two large instruments, such as a 10-mm laparoscope and a 12-mm flexible stapler, with a 5-mm instrument. This configuration allows for enough mobility and triangulation with a 30-mm skin and apouneurosis opening, which was applied in all cases.
The operation begins with exploration of the abdominal cavity with the laparoscope. An intraoperative laparoscopic ultrasound probe (SonoSite®, Inc., Bothell, WA) is introduced. The liver is examined to rule out other lesions and to ascertain liver anatomy (Fig. 1c). It may be useful to locate the Glissonian pedicle from segments 2 and 3. The left liver is then mobilized by sectioning the falciform and the left triangular and left coronary ligaments with a Harmonic scalpel (Ultracision®; Ethicon Endo Surgery, Cincinnati, OH). The left lobe is pulled upward, and the lesser omentum is divided.
The next step is to perform intrahepatic Glissonian access for retrieval of the portal pedicles from segments 2 and 3, as previously described. 7 Two incisions are performed: one above the proximal part of the Arantius ligament and the second incision at the left side of the basis of the round ligament (Fig. 1d). A large vascular clamp is introduced through these incisions and closed. After a few moments, ischemic delineation of segments 2 and 3 is obtained (Fig. 2a). If the delineation confirms adequate access to the pedicles of segments 2 and 3, the clamp is replaced by a vascular endoscopic stapler (Fig. 2b). The stapler is fired, and the portal pedicle from segments 2 and 3 is divided. The future line of transection is marked with a cautery according to the ischemic delineation. The liver transection progresses with the Harmonic scalpel. The last step is to divide the left hepatic vein with a stapler.
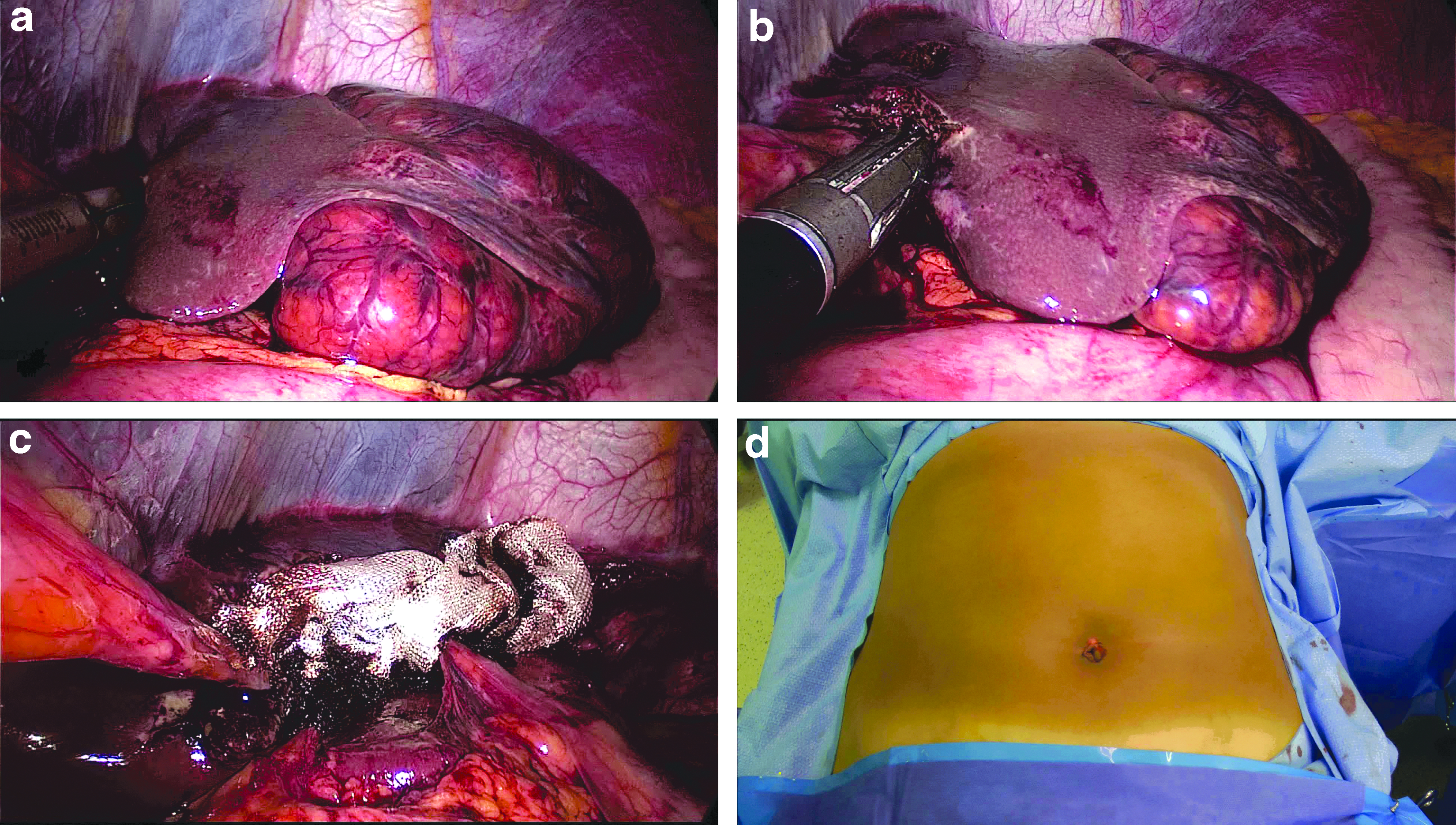
Single-port laparoscopic left lateral sectionectomy.
A surgical specimen is retrieved inside a plastic bag through the single-port incision. The incision needs to be enlarged depending on the size of the specimen, but, most of the time, the left lateral segment can be retrieved through the usual 3-cm umbilical incision. Benign liver tumors are macerated inside a plastic bag without enlargement of the umbilical incision. The raw area of the liver is checked for bleeding and bile leaks. Hemostatic tissue is applied to the raw surface of the liver (Fig. 2c). The single-port platform is then reattached. Meticulous closure of the incision is performed in order to avoid incisional hernias, and the procedure is finished. No drains are left in place.
Results
We have performed this procedure on 8 consecutive patients. Seven patients were women. The median duration of the procedure was 68 minutes (range, 45–100 minutes). Bleeding was minimal in all cases (less than 100 mL) with no need for blood transfusion. Intraoperative ultrasound was performed in all cases, and no unexpected lesions were found. The median hospital stay was 1 day (range, 1–2 days). The final pathology was liver adenoma in 6 cases, focal nodular hyperplasia in 1 case, and cholangiocarcinoma in 1 case (male patient). There was no morbidity and no mortality. The median follow-up was 12 months (range, 8–18 months), during which no patient developed incisional hernia. The cosmetic appearance of the incision was excellent in all cases (Fig. 2d).
Discussion
Laparoscopic liver surgery has experienced significant growth in the last few years. This technique has become a less invasive alternative to liver surgery, and both preoperative and intraoperative imaging advances have resulted in better anatomic assessment and better surgical planning. 5 Our experience, published in 2012, 6 with laparoscopic liver resections began in 2007. Progressive improvement of our expertise in laparoscopic surgery has allowed us to perform more complex operations, such as extended right hepatectomy, mesohepatectomy, and two-stage liver resection. 6 However, only a few centers are performing laparoscopic liver resection on a routine basis.5,6 For most surgeons, the laparoscopic approach for left lateral sectionectomy is considered the gold standard. 8 Furthermore, we consider that any anatomical liver surgery can be done by laparoscopy, but we do agree that it should be done by experts only.5,6
The single-incision laparoscopic method is less invasive than conventional multiport laparoscopy, but there may be unique difficulties for the laparoscopic surgeon.9–15 First, retraction is significantly limited. The introduction of a camera and various instruments parallel to each other may result in decreased mobility and the collision of instruments.9–11 The single-incision platform used in our series allows for the use of standard instruments. There was no loss of triangulation due to the presence of self-retaining sleeves, which maximize the internal working diameter. We were able to use a high-definition 10-mm laparoscope during all steps of the operation.
We have chosen to begin our experience in single-port hepatectomy with laparoscopic left lateral sectionectomies because this procedure is the easiest to perform by laparoscopy and is already well standardized.7,8 In the English literature, there are only a few articles dealing with single-port liver resection.9–15 The main reason is that the majority of systems available for a single-site laparoscopic surgery need specific articulating instruments, use small laparoscopes, and allow for poor triangulation. Our initial experience with single-port laparoscopic left lateral sectionectomy showed no exposure or triangulation difficulties. The operative time was not superior to our other laparoscopic cases, and there was no morbidity or mortality.
One of the potential disadvantages of the single-port surgery compared with conventional multiport laparoscopy is the development of incisional hernias. 16 However, prospective studies did not confirm these findings, which may be the result of the learning curve. In our series, there was no incisional hernia in late follow-up. Although several issues such as cost and the learning curve of this technique remain to be studied, the cosmetic benefits of single-incision approach are obvious.10,12,15
In conclusion, single-port laparoscopic left lateral sectionectomy is feasible and can be safely performed in specialized centers by experienced laparoscopic surgeons. We believe that this new system may reduce the learning curve for single-port laparoscopy, as it provides better maneuverability than previous platforms. As soon as more experience is obtained in this technique, we expect that single-port left lateral sectionectomy may become the method of choice.
Footnotes
Disclosure Statement
No competing financial interests exist.